
Abstract
Current guidelines for treatment of type 2 diabetes mellitus (T2DM) indicate a patient-centered approach that should go beyond glycemic control. Of the many antihyperglycemic agents available for treatment of T2DM, sodium-glucose cotransporter 2 (SGLT2) inhibitors offer the advantages of reduced glycated hemoglobin (A1C), body weight (BW), and systolic blood pressure (SBP) and are associated with a low risk of hypoglycemia when used either as monotherapy or with other agents not typically associated with increased risk of hypoglycemia. Collaborative, multidisciplinary teams are best suited to provide care to patients with diabetes, and clinical pharmacists can enhance the care provided by these teams. This review aims to provide insight into the mode of action, pharmacology, potential drug–drug interactions, clinical benefits, and safety considerations associated with use of the SGLT2 inhibitor canagliflozin in patients with T2DM and to provide information to enhance clinical pharmacists' understanding of canagliflozin.
Introduction
Current guidelines for management of type 2 diabetes mellitus (T2DM) recommend individualized glycemic goals and treatment strategies. T2DM is associated with microvascular and macrovascular complications that affect morbidity and mortality. Each of the drug classes currently available for the treatment of T2DM affects glycemic control and the risk of these complications differently. Metformin is recommended as the first-line therapy for most patients with T2DM, in addition to diet and exercise.1,2 When second-line therapy is needed, the selection of antihyperglycemic agents (AHAs) should consider the patient's glycemic goals and current control, balanced by their comorbidities and risk factors (eg, for weight, and cardiovascular and renal events).2,3 The effect of an AHA on body weight (BW) and hypoglycemia is an especially important consideration, given the prevalence of obesity among patients with T2DM and the impact of hypoglycemia on improved glycemic control, adherence, and cardiovascular risk.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors are the latest approved class of oral medication for treatment of T2DM. They offer the advantages of reduced glycated hemoglobin (A1C), BW, and systolic blood pressure (SBP), as well as a low risk of hypoglycemia when used either as monotherapy or in combination with other AHAs not typically associated with increased risk of hypoglycemia.4,5 Canagliflozin (Invokana®) was the first SGLT2 inhibitor to receive FDA approval, followed by dapagliflozin (Farxiga®) and empagliflozin (Jardiance®).6–8 SGLT2 inhibitors are included as a treatment option in dual and triple therapies for T2DM in the Standards of Medical Care in Diabetes of the American Diabetes Association (ADA); 2 the American Association of Clinical Endocrinologists diabetes management algorithm also includes SGLT2 inhibitors as a monotherapy treatment option and a second option in metformin failure patients. 1
This review aims to enhance understanding of canagliflozin by discussing the mechanism of action of SGLT2 inhibitors as a class, the pharmacology of canagliflozin specifically and the clinical benefits and safety considerations associated with canagliflozin use, and the important role pharmacists can play in utilization of canagliflozin in the management of T2DM.
Mechanism of Action of SGLT2 Inhibitors
In healthy individuals, the kidneys filter ∼180 g of glucose per day, virtually all of which is reabsorbed from the renal filtrate.5,9 SGLT2, a high-capacity, low-affinity transporter that is expressed on the luminal surface of the proximal tubule, accounts for ∼90% of renal glucose reabsorption. 10 Under normal conditions, sodium-glucose cotransporter 1 (SGLT1), a low-capacity, high-affinity transporter that is expressed in the proximal tubule and in the small intestine, accounts for the remaining glucose reabsorption. 10 The renal threshold for glucose (RTG), or plasma glucose concentration at which glucosuria occurs, is 180–200 mg/dL in healthy individuals, but in patients with T2DM, SGLT2 expression and renal glucose uptake is increased. This can further contribute to hyperglycemia.5,11 SGLT2 inhibitors currently on the market are competitive, reversible, selective inhibitors of the SGLT2 transporter in the proximal tubule of the kidney, which results in a reduction in reabsorption of renal filtrate glucose leading to increased urinary glucose excretion (UGE) and reduction of plasma glucose (Fig. 1). 12

Mode of action of SGLT2 inhibitors in the kidney. Copied with permission from Scheen. 12
Canagliflozin Pharmacology
Chemistry
Canagliflozin or (1S)-1,5-anhydro-1-[3-[[5-(4-fluorophenyl)-2-thienyl]methyl]-4-methylphenyl]-

The structure of canagliflozin. 13
Pharmacokinetics
Pharmacokinetic parameters in patients with T2DM are shown in Table 1. After single- and multiple-dose administration of canagliflozin for seven days, the mean area under the plasma concentration–time curve (AUC) and maximum plasma concentration (Cmax) increased in a dose-dependent manner between day 1 and day 7.
14
Canagliflozin was rapidly absorbed after oral administration (median time at which C was observed [tmax] = 1.5 hours). Canagliflozin half-life (t
Pharmacokinetic parameters (mean [SD]) after single- and multiple-dose administration of canagliflozin in patients with T2DM. 14

Pharmacodynamics
In patients with T2DM, canagliflozin doses of ≥100 mg/day lowered the 24-hour mean RTG from 98–104 mg/dL to 77–85 mg/dL. 14 Canagliflozin 100 and 300 mg increased UGE (to ∼100 g/day at doses ≥100 mg), resulting in reduced fasting plasma glucose and 24-hour mean plasma glucose levels.14,16 In a Phase 2 study in patients with T2DM, canagliflozin at all doses increased UGE, which persisted without attenuation through 12 weeks. 17 While canagliflozin can be taken with or without food, it is recommended that it is taken before the first meal of the day. 13 In healthy subjects and patients with T2DM, treatment with canagliflozin 300 mg has been shown to delay intestinal glucose absorption and reduce postprandial glucose excursion.18,19 This effect was transient and was observed only during the first meal following 300 mg dose administration and is likely due to luminal concentrations of canagliflozin being high enough to inhibit intestinal SGLT1. Furthermore, in a separate trial, canagliflozin 300 mg significantly lowered the RTG, increased UGE, and reduced postprandial glucose excursion more than dapagliflozin 10 mg in healthy subjects. 20
Drug– Drug Interactions
Canagliflozin and Metformin, Glyburide, Simvastatin, Warfarin, and Hydrochlorothiazide
Coadministration of canagliflozin with metformin or glyburide did not result in increased exposure to metformin or glyburide. 21 Additionally, no clinically meaningful changes in mean plasma glucose were observed, and coadministration did not lead to increased incidence of hypoglycemia in healthy adults. 21 Exposure to simvastatin increased by 12% (maximum plasma concentration) and 9% (area under the curve) when canagliflozin 300 mg was coadministered, but this change did not require dose adjustments. 21 Similarly, no changes requiring dose-adjustment were observed when canagliflozin was coadministered with the anticoagulant warfarin. 22 Importantly, hydrochlorothiazide (HCTZ) and canagliflozin both target the kidneys and exert a diuretic effect. Coadministration of HCTZ 25 mg and canagliflozin 300 mg increased geometric least squares (LS) mean AUC during the dosing interval at steady state (AUCτ,ss) of canagliflozin by ∼12%, and increased geometric LS mean Cmax at steady state (Cmax,ss) of canagliflozin by ∼15%. These changes are unlikely to be clinically relevant. AUCτ,ss and Cmax,ss of HCTZ were similar with and without canagliflozin. 23
Canagliflozin and Digoxin
Digoxin is a substrate of P-glycoprotein, which is weakly inhibited by canagliflozin in vitro. 22 In healthy volunteers, coadministration of canagliflozin 300 mg with digoxin (0.5 mg on day 1, followed by 0.25 mg for six days) increased plasma exposure to digoxin (Cmax, +36%; AUC, +20%). 22 However, the amount of digoxin excreted into the urine during the first 24 hours after administration and its renal clearance (CLR) are similar with or without canagliflozin, suggesting that urinary elimination of digoxin is not affected by canagliflozin. 22 The upper limit of the therapeutic concentration range for digoxin (0.8–2.0 ng/mL) was not exceeded for any patient treated concomitantly with digoxin and canagliflozin. However, given the narrow therapeutic index of digoxin, patients receiving combined treatment with canagliflozin and digoxin should be monitored appropriately. 22
Canagliflozin and Rifampin
Canagliflozin is mainly metabolized by uridine diphosphate-glucuronyltransferases (UGT) 1A9 and UGT2B4 and also by cytochrome P450 (CYP) 3A4 (∼7%). 15 Therefore, a strong inducer of UGT, such as the antibiotic rifampin, may increase the elimination of canagliflozin. Coadministration of rifampin 600 mg with canagliflozin 300 mg decreased canagliflozin exposure (AUC, −51%; Cmax, −28%) and hence may decrease its efficacy. It is therefore recommended that when canagliflozin is used in patients with T2DM who also receive a strong inducer of UGT, canagliflozin dose is increased to 300 mg in patients who tolerate canagliflozin 100 mg and have an estimated glomerular filtration rate (eGFR) of ≥60 mL/minute/1.73 m2, or to add a different AHA in patients with an eGFR of <60 mL/minute/1.73 m2.13,24
Clinical Benefits: Meeting Treatment Goals
Selection of AHAs should be driven by several factors including baseline A1C, comorbidities, contraindications and precautions, adverse effects, hypoglycemic risk, cost, and patient preference, but additionally by factors that can contribute to cardiovascular risk reduction, which includes management of BW, especially visceral fat or central adiposity, and blood pressure (BP). 2 Most patients with T2DM should be managed to achieve A1C levels of <7.0% and BP <140/90 mmHg. 2 Low-density lipoprotein cholesterol of <100 mg/dL was previously recommended; 25 however, the most recent guidelines advise treatment by cardiovascular risk status rather than specific lipid values. 2
Effect on A1C
As monotherapy, canagliflozin 100 and 300 mg reduced A1C by 0.91% and 1.16%, respectively, relative to placebo after 26 weeks. 26 Added on to metformin, canagliflozin 100 and 300 mg reduced A1C by 0.82% and 0.93%, respectively, after 52 weeks, which was similar (canagliflozin 100 mg) and greater (canagliflozin 300 mg) to reductions achieved with glimepiride (GLIM; mean dose 5.6 mg/day; −0.81%). 27 The effect on A1C was sustained through 104 weeks. 28 Also added on to metformin, after 52 weeks, A1C reduction with canagliflozin 100 mg (−0.73%) was similar to that with sitagliptin 100 mg, while A1C reduction with canagliflozin 300 mg (−0.88%) was greater compared with sitagliptin 100 mg (−0.73%). 29 In triple therapy, added to metformin and a sulfonylurea, A1C reduction with canagliflozin 300 mg was greater than with sitagliptin 100 mg (1.03% versus 0.66%) over 52 weeks. 30
When canagliflozin was added to insulin (>20 IU/day, mainly basal-bolus, mean daily insulin dose 60 IU/day), placebo-subtracted A1C reductions of 0.62% and 0.73% were observed with canagliflozin 100 and 300 mg, respectively, at 18 weeks; these results were maintained at 52 weeks. 31
Canagliflozin 100 and 300 mg significantly reduced fasting and two-hour postprandial glucose in clinical studies.26–38 Improvements in glycemic control occurred regardless of baseline A1C or known duration of T2DM, with greater A1C reductions from baseline observed in canagliflozin-treated patients with higher baseline A1C levels.26,30 Consistent with site of action (renal tubules), the A1C-lowering efficacy of canagliflozin was shown to be independent of pancreatic beta cell function or insulin sensitivity. 39
Canagliflozin Effect on Cardiovascular Risk Factors
Use of canagliflozin is associated with dose-dependent, sustained reductions in BW of ∼3%–5% across studies.26–30 Added on to metformin, canagliflozin 100 and 300 mg were associated with BW reductions of 4.2% and 4.7%, respectively, versus an increase of 1% with GLIM (mean dose 5.6 mg/day) after 52 weeks, 27 with effects sustained up to 104 weeks. 28 Compared with sitagliptin, canagliflozin was also associated with significantly larger BW reductions after 52 weeks when added on to metformin (canagliflozin 100 mg: 3.8%; canagliflozin 300 mg: 4.2%; sitagliptin 100 mg: 1.3%) 29 or metformin plus sulfonylurea (canagliflozin 300 mg: 2.5%; sitagliptin 100 mg: +0.3%). 30 The initial weight reduction associated with canagliflozin can be attributed to fluid loss, 40 but two-thirds of the continued reduction in weight at 52 weeks were due to loss of fat mass. 27
Clinically meaningful reductions in SBP have been observed with canagliflozin compared with placebo and active comparators. As monotherapy, canagliflozin 100 and 300 mg significantly reduced SBP compared with placebo at 26 weeks (−3.3 and −5.0 mmHg versus +0.4 mmHg, respectively). 26 Added on to metformin, canagliflozin 100 and 300 mg reduced SBP at 52 weeks (−3.3 and −4.6 mmHg), while GLIM (mean dose 5.6 mg/day) was associated with an increase of +0.2 mmHg. 27 Compared with sitagliptin 100 mg, canagliflozin 100 and 300 mg significantly reduced SBP (−3.5 and −4.7 mmHg versus −0.7 mmHg, respectively) at 52 weeks. 29 Added on to metformin plus sulfonylurea, canagliflozin 300 mg also significantly reduced SBP compared with sitagliptin 100 mg (−5.1 mmHg versus −0.9 mmHg, respectively). 30
Treatment with canagliflozin has been associated with decreases in fasting triglycerides (−5.2% and −7.6% placebo-subtracted change with canagliflozin 100 and 300 mg), increases in fasting high-density lipoprotein cholesterol (5.4% and 6.3% placebo-subtracted change with canagliflozin 100 and 300 mg, respectively), and dose-related increases in fasting low-density lipoprotein cholesterol (LDL-C; 4.5% and 8.0% placebo-subtracted change with canagliflozin 100 and 300 mg, respectively) and fasting total cholesterol (2.5% and 4.3% placebo-subtracted change with canagliflozin 100 and 300 mg, respectively). 41 In a 52-week study in patients with moderate renal impairment, fasting LDL-C increased over time with canagliflozin 100 and 300 mg and placebo, but was not different between canagliflozin and placebo. 42 The mechanism for changes in LDL-C with canagliflozin is unknown; however, it is advisable to monitor cholesterol levels in patients with diabetes treated with canagliflozin and adjust medication as required.
The cardiovascular safety of canagliflozin is being evaluated in the ongoing Canagliflozin Cardiovascular Assessment Study (CANVAS, NCT01032629) and CANVAS-R studies (NCT01989754). An interim meta-analysis of data from Phase 2 and 3 studies suggests that canagliflozin treatment is not associated with an increased cardiovascular risk. 43
In a post hoc analysis of a Phase 3 study comparing various quality measures between canagliflozin 300 mg and sitagliptin 100 mg as an add-on therapy to metformin plus sulfonylurea, a higher proportion of patients treated with canagliflozin 300 mg achieved A1C levels of <8.0% (85.0% versus 66.0% with sitagliptin) or <7.0% (47.6% versus 35.3% with sitagliptin 100 mg) at 52 weeks (Fig. 3). 44 Additionally, the proportion of patients achieving BP < 140/90 mmHg was higher with canagliflozin 300 mg than with sitagliptin 100 mg (84.5% versus 71.9%). 44 Moreover, a higher proportion of patients receiving canagliflozin 300 mg achieved the combined quality measure of A1C < 8.0%, BP < 140/90 mmHg, and LDL-C < 100 mg/dL, compared with those receiving sitagliptin 100 mg (35.5% versus 27.8%). 45

Proportion of patients who met quality measures at baseline and achieved quality measures at week 52 in a randomized, double-blind, active-controlled, Phase 3 study that compared canagliflozin 300 mg with sitagliptin 100 mg as an add-on therapy to metformin plus sulfonylurea in patients with T2DM. Figure reproduced with permission from Bailey et al. 44
Clinical Benefits of Canagliflozin in Patients with Reduced Renal Function
Based on the new Kidney Disease Improving Global Outcomes classification, 46 prevalence of chronic kidney disease (CKD) in patients with T2DM is 43.5%, while more severe renal impairment (eGFR < 45 mL/minute/1.73 m2) is observed in < 10% of patients with T2DM. 45 Moderate-to-severe renal impairment (eGFR < 60 mL/minute/1.73 m2) has been reported to occur in ∼20%–30% of patients with T2DM. 47 In a clinical study, canagliflozin 100 and 300 mg reduced A1C in patients with Stage 3 CKD (defined as eGFR ≥ 30 mL/minute/1.73 m2 and eGFR ≤ 50 mL/minute/1.73 m2 in this study).32,48 Since the efficacy of SGLT2 inhibitors is dependent on the ability of the kidneys to filter glucose, it is not surprising that the A1C-lowering efficacy is attenuated in patients with moderate renal impairment (Stages 3A and 3B CKD) compared with those with normal renal function or mild renal impairment (Fig. 4). 33 Attenuated but significant reductions in BW, and SBP reductions similar to those observed in patients with normal renal function, were also observed in patients with Stage 3 CKD treated with canagliflozin 100 and 300 mg.33,42 It is important to note that canagliflozin 100 mg is the indicated dose in T2DM patients with an eGFR of 45 to <60 mL/minute/1.73 m2 and that treatment should not be initiated in patients with an eGFR of <45 mL/minute/1.73 m2. 13

Canagliflozin reduces A1C in people with T2DM and CKD. Figure reproduced with permission from Yamout et al. 33
Safety Considerations with use of Canagliflozin
In a pooled analysis of four 26-week, placebo-controlled studies, the overall incidence of adverse events (AEs), including those considered serious and those leading to discontinuation, was generally similar with canagliflozin relative to placebo. 41 Because of their mechanism of action (ie, increasing UGE), SGLT2 inhibitors are associated with increased incidence of genital mycotic infections (GMIs) and urinary tract infections (UTIs).49,50 The incidence of GMIs associated with canagliflozin 100 and 300 mg was higher compared with placebo in both women (10.4% and 11.4% versus 3.2%, respectively) and men (4.2% and 3.7% versus 0.6%, respectively).41,51 Patients with a prior history of GMI and uncircumcised men tended to be at higher risk of experiencing a GMI with canagliflozin treatment.13,41,51 There was no difference in incidence of GMI in patients aged ≥65 years compared with patients aged <65 years. 33 GMIs associated with the use of canagliflozin mostly occurred during the first three months after treatment initiation, with incidence decreasing over time.51,52 GMIs were generally mild or moderate in intensity and responded well to standard treatment.13,36,41,51 In clinical trials, most GMIs were treated with antifungal agents, often initiated by the patients themselves. Topical and oral antifungal treatment appeared to be equally effective in female patients. 51 Only a small proportion of patients discontinued due to GMI (∼1%). 52 The incidence of UTIs (primarily those associated with the lower urinary tract) was modestly higher with canagliflozin 100 and 300 mg compared with placebo (5.9% and 4.3% versus 4.0%, respectively).41,53 Importantly, there was no notable difference in upper UTIs between canagliflozin and placebo. 53 Not all studies reported a higher risk: the incidence of UTIs with canagliflozin 100 and 300 mg was similar to that with sitagliptin 100 mg29,30 and only slightly higher compared with that with GLIM (mean dose 5.6 mg/day).27,28 Canagliflozin was also not associated with increased incidence of UTIs in patients aged ≥65 years compared with those aged <65 years. 36 Increased UGE contributes to the osmotic diuresis observed with SGLT2 inhibitors, which may result in volume depletion and hypotension. 49 AEs related to osmotic diuresis, such as thirst or increased urination (polyuria or pollakiuria), occurred more often with canagliflozin 100 and 300 mg compared with placebo (6.7% and 5.6% versus 0.8%, respectively). 41 When compared with GLIM (mean dose 5.6 mg/day)27,28 and sitagliptin 100 mg,29,30 the incidence of osmotic diuresis-related AEs was slightly higher. These events tended to develop within the first six weeks of canagliflozin treatment, with incidence waning thereafter. 41
Pooled data from a four 26-week study analysis reported similar rates of volume depletion-related events (eg, hypotension, postural dizziness, and orthostatic hypotension) with canagliflozin 100 and 300 mg and placebo (1.2%, 1.3%, and 1.1%). 41 Incidence of volume depletion-related AEs was slightly higher in patients aged ≥65 years. 36 Across eight clinical studies, patients aged ≥75 years, patients with an eGFR of 30–60 mL/minute/1.73 m2, and patients using loop diuretics were at an increased risk of volume depletion-related AEs when treated with canagliflozin 300 mg. 13
In a pooled analysis of data from Phase 3 studies, no meaningful changes from baseline in sodium, potassium, bicarbonate, and calcium were seen with canagliflozin relative to placebo, and small mean percent increases from baseline in serum magnesium and phosphate were noted. 54 The proportion of patients with serum potassium elevations meeting predefined outlier criteria (>5.4 mmol/L [5.4 mEq/L] and >15% increase from baseline) was increased with canagliflozin 300 mg, but not with canagliflozin 100 mg versus placebo in patients with moderate renal impairment and typically taking agents that affect potassium excretion.13,55 AEs related to changes in serum electrolytes (ie, potassium, sodium, magnesium, bicarbonate, phosphate, and calcium) occurred infrequently among patients with T2DM receiving canagliflozin 100 or 300 mg, with or without renal impairment. 55 Canagliflozin treatment (100 and 300 mg) reduced serum uric acid levels by 0.7 mg/dL (∼13%) after 26 weeks. 56
Modest improvements in indicators of liver function (such as alanine aminotransferase and aspartate aminotransferase) have been reported in patients with T2DM receiving canagliflozin as monotherapy,26,37 as double therapy, 34 and as double or triple therapy (pooled analysis). 41 In a pooled study population of patients with T2DM, canagliflozin 100 and 300 mg have been associated with an initial, transient mean increase in serum creatinine 13 and a subsequent reduction in eGFR after treatment initiation, which stabilizes or attenuates toward baseline levels over time. 41 In a Phase 3 trial comparing canagliflozin with GLIM, eGFR initially decreased, but subsequently attenuated and remained stable over 104 weeks with canagliflozin 100 and 300 mg versus a progressive decline in eGFR throughout the 104-week treatment period observed with GLIM (mean dose 5.6 mg/day; Fig. 5). 28 In older patients, eGFR also initially decreased, followed by stabilization at baseline level at 26 weeks; eGFR remained stable with continued treatment for 104 weeks. 38 The development of renal impairment was rare, occurring in 0.1% of those receiving canagliflozin 100 or 300 mg. 41 Findings were similar in patients with Stage 3 CKD. 33 SGLT2 inhibitors have been shown to lower glucose and SBP and reduce albuminuria and hyperfiltration, which suggests that they may provide renoprotection in patients with T2DM. 56 A Phase 3 clinical study, the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation Trial (CREDENCE, NCT02065791), is ongoing and has been designed to assess whether canagliflozin has a renal protective effect in patients with T2DM, Stage 2 or 3 CKD, and macroalbuminuria.
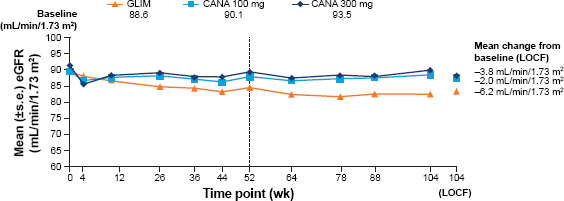
Mean eGFR in patients with T2DM receiving canagliflozin 100 or 300 mg, or GLIM over 104 weeks. Reproduced with permission from Leiter et al. 28
In patients not on background antihyperglycemic therapy associated with hypoglycemia, incidence of hypoglycemia was low with canagliflozin 100 and 300 mg, and generally comparable with placebo. 41 As anticipated, the incidence of hypoglycemia with canagliflozin is increased in patients using a sulfonylurea or insulin.31,41 Incidence of hypoglycemia with canagliflozin was similar compared with sitagliptin when added to metformin and sulfonylurea 30 and lower compared with GLIM.27,28 We advise to consider adjusting insulin or secretagogue dose when starting a patient with SGLT2 inhibitors.
Recently, the FDA issued a Drug Safety Communication indicating that SGLT2 inhibitors may lead to diabetic ketoacidosis (DKA). Based on cases in the FDA Adverse Event Reporting System database, patients may present atypically, with only slightly increased blood glucose levels. 57 A series of nine cases of incidental euglycemic DKA associated with SGLT2 inhibitor use has since been described. Of note, in seven of these cases, the subject had been diagnosed with type 1 diabetes mellitus (T1DM). 58
An analysis of 17,596 patients from 15 finalized and ongoing trials of the canagliflozin clinical trial program identified 12 patients on canagliflozin or not on canagliflozin within a total of 13 unblinded serious AEs of DKA, ketoacidosis, metabolic acidosis, or acidosis. 59 Of the 12 patients with a reported DKA-related event, six patients (all treated with canagliflozin) were found to have T1DM, latent autoimmune diabetes of adulthood, and/or antibodies for glutamic decarboxylase. Most of these patients did present with blood glucose levels >300 mg/dL, were treated with insulin, and had one or more known precipitating factors for DKA at the time of the event. 59 The authors conclude that the incidence of DKA in these patients from the canagliflozin clinical trial program was low and consistent with reported observational data in general diabetes populations.59,60 Further research will be required to clarify the potential association of SGLT2 inhibitors with DKA in patients with T2DM and identify patients who are at risk of developing DKA. Instructing patients starting on SGLT2 inhibitors on signs of DKA and on how to properly act on these symptoms is advisable.
Patient Selection, Counseling, and Support: The Pharmacist's Role
Canagliflozin has been demonstrated to be effective and well tolerated in a wide range of patients with diabetes at various stages of disease progression. To reiterate, canagliflozin is not indicated in patients with an eGFR of <45 mL/minute/1.73 m2, while for patients with an eGFR of ≥45 mL/minute/1.73 m2 but <60 mL/minute/1.73 m2, only canagliflozin 100 mg should be used. 13 Use of canagliflozin is associated with more frequent occurrence of GMIs, but these are usually mild or moderate in intensity and respond to standard treatment.13,36,41,51 Incidence of GMIs is highest early in treatment, and declines with time. In patients who have a history of GMIs, pharmacists can counsel on the importance of good hygiene. Remember to tell the patients to stay clean and dry, to wear moisture-absorbent undergarments, and to wipe from front to back to decrease the risk of GMIs (note that this has not specifically been tested in a prospective trial with canagliflozin). In addition, consider asking patients who come to refill their prescription if they have used any over-the-counter creams to treat GMIs as these will not be documented by most clinicians. Pharmacy records of patient medication history can be used to identify patients at risk of specific AEs, such as use of loop diuretics, which can suggest an increased risk of AEs related to volume depletion. Be aware if a patient is starting on an SGLT2 inhibitor in combination with a diuretic, or if you think the person could become easily dehydrated. Older adults (≥75 years), patients with moderate renal impairment (eGFR ≥30 to <60 mL/minute/1.73 m2), and those receiving loop diuretics may be at higher risk of AEs related to volume depletion. 13 Therefore, consider reducing the dose of any loop diuretic prior to initiating canagliflozin treatment, and preexisting volume depletion should be corrected prior to starting canagliflozin therapy. 13
Prior to initiating canagliflozin, healthcare providers should consider whether patients have other risk factors for falling (eg, dementia) or for negative outcomes from falling, since canagliflozin is associated with a small increased risk of fractures in patients with known cardiovascular disease or at high risk of cardiovascular disease (ie, the recruited population in the CANVAS/CANVAS-R trials). 61 Fractures were observed as early as 12 weeks after treatment initiation, were more likely to be low trauma (eg, fall from no more than standing height), and affect the upper extremities (hand and wrist). Conversely, there was no increased risk of fracture with canagliflozin in a pooled analysis of patients from the Phase 3 clinical trials, excluding those from CANVAS trials. 13 Two years of treatment with canagliflozin in older adults (55–80 years old) led to no significant changes in bone mineral density (BMD) at the femoral neck, lumbar spine, and distal forearm and small, significant decreases in BMD at the total hip compared with placebo, which were associated with weight loss observed with canagliflozin. 62 Patients experiencing osmotic diuresis-related events such as thirst, polyuria, or pollakiuria may appreciate knowing that these reactions also tend to wane with time. Importantly, tell all patients to drink enough water to stay hydrated at the start of therapy.
Pharmacists can contribute to the care of patients with T2DM receiving canagliflozin therapy by monitoring for efficacy, AEs, and adherence. Pharmacists with BP monitors in their clinics or pharmacies can monitor BP in patients starting and continuing canagliflozin.
Due to their mode of action (increasing UGE), use of SGLT2 inhibitors will lead to positive urine glucose tests, and use of these tests is not recommended with the use of SGLT2 inhibitors. A consequence of increasing UGE is the prevention of renal reabsorption of 1,5-anhydroglucitol (1,5-AG), leading to a decrease in serum 1,5-AG. Use of canagliflozin has been shown to interfere with testing for 1,5-AG levels (GlycoMark®; GlycoMark Inc.), leading to falsely low results, which would indicate poorer glycemic control.63,64
Through a simple medication review, pharmacists are exceptionally well positioned to capture elements of patient history that other healthcare providers may not have direct access to, and to advise on intervention when needed. Reports indicate that pharmacists can make a significant contribution to the primary care of patients with T2DM.65,66 Specifically, adding a pharmacist to a primary care team increased the proportion of patients meeting A1C and BP goals. 65 Some pharmacists advise the prescribing clinician following their assessment of the patient, while others have the autonomy to prescribe medication. 65 It is therefore important for clinical pharmacists serving as members of healthcare teams to understand the mode of action, pharmacokinetics and pharmacodynamics, and efficacy and safety aspects of the many AHAs available for the management of T2DM.
Conclusions
In summary, canagliflozin has been shown to reduce A1C, BW, and SBP in a wide range of patients with T2DM, including those with moderate renal impairment, though efficacy wanes as renal function declines. Canagliflozin is generally well tolerated, but is associated with AEs related to the mechanism of action (GMIs, osmotic diuresis-, and volume depletion-related AEs). Incidence of hypoglycemia with canagliflozin is low in patients who are not on insulin or a sulfonylurea. We believe that monitoring the clinical benefits of canagliflozin by pharmacists, as well as patient education about which AEs may occur and how to manage these, may increase patient adherence and the overall positive effect of therapy.
Footnotes
Author Contributions
Jointly developed the structure and arguments for the paper, contributed to the writing of the manuscript, made critical revisions, and approved the final version: CT and SC.