
Abstract
Objective
To assess the real-world efficacy and safety of the first sodium-glucose cotransporter-2 inhibitor, canagliflozin, in the treatment of patients with type 2 diabetes mellitus (T2DM).
Methods
This observational study assessed the efficacy and tolerability of canagliflozin in T2DM patients. Primary study outcomes were changes in HbAlC and weight, and percentage of patients reporting adverse effects of therapy.
Results
The study criteria were met by 111 patient records. Baseline patient characteristics were: average age, 59 ± 9 years; mean duration of T2DM, 11.9 ± 7.3 years; 57.6% of patients were male; 92.8% were Caucasian; baseline BMI, 38.9 ± 11 kg/m2; and mean baseline HbAlC, 7.53 (58.8 mmol/mol) ± 1.08%. HbAlC and weight were significantly reduced by 0.37% and 4.4 kg, respectively. Adverse effects were reported by 21 patients, and 17 (15.3%) discontinued canagliflozin because of adverse reactions.
Conclusion
Canagliflozin was generally well tolerated and significantly reduced HbAlC levels and body weight in patients with T2DM when added to a regimen of other anti-hyperglycemic agents.
Introduction
Type 2 diabetes mellitus (T2DM) is an increasingly prevalent disease, with an estimated 29.1 million Americans, or 9.3% of the US population, having diabetes, including 25.9% of patients 65 years of age and older. 1 Diabetes was the seventh-leading cause of death in the United States in 2010 and patients with T2DM have roughly a two- to four-fold greater risk of death caused by cardiovascular disease compared to those without diabetes. 1
T2DM is a progressive, complex disease state with multiple pathophysiologic abnormalities. 2 Metformin is the recommended first-line pharmacologic therapy for T2DM,3,4 and sulfonylureas have historically been used early in the course of disease. However, these agents are associated with high secondary failure rates, 5 and sulfonylurea therapy is associated with hypoglycemia and weight gain.
More than 40% of adults with T2DM in the US have not obtained goal glycemic control. 6 Patients often require combinations of anti-hyperglycemic agents to maintain glycemic control, because of the progressive nature of T2DM. Thus, combination therapy using drugs with complimentary mechanisms of action should be utilized for appropriate glycemic control.2,3 Agents that can improve glycemic control without increasing hypoglycemia, promote weight loss, and improve β-cell function are especially desirable. Although the sodium-glucose co-transporter 2 (SGLT-2) inhibitors have not been shown to be a disease-modifying agent in regards to preserving β-cell function, they have been shown to improve blood glucose levels and have a positive effect on body weight and blood pressure. 7 SGLT-2 inhibitors possess a unique pharmacologic mechanism of action, which is independent of insulin secretion and therefore effective despite the duration of disease. Furthermore, the action of SGLT-2 inhibitors is additive to that of other diabetes medications. Canagliflozin lowers the renal threshold for glucose and increases urinary glucose excretion. This results in decreased plasma glucose levels, as well as a mild osmotic diuresis and a net caloric loss, thus promoting lower HbAlC, weight loss, and systolic blood pressure reduction, all with a minimal risk of hypoglycemia.
Because of the wide prevalence of T2DM, drug efficacy and drug safety are important considerations in drug selection for patients with diabetes. The goal of this study was to assess the real-world efficacy and safety of canagliflozin in patients with T2DM already receiving anti-hyperglycemic therapy.
Methods
Research design and data collection
This pre-post observational study assessed the efficacy and tolerability of canagliflozin in type 2 diabetes patients from a private endocrinology practice. The study protocol was approved by the Albany College of Pharmacy and Health Sciences Institutional Review Board. The study population consisted of T2DM patients who were prescribed canagliflozin in 2013. A computerized text search of the medication and problem lists of patient electronic medical records (EMR) was used to identify potential subjects. Search terms included canagliflozin, Invokana, and SGLT-2 inhibitor. Individual records of identified patients were reviewed to ascertain if all applicable study criteria were met. Inclusion criteria were: age between 18-95 years, documented diagnosis of type 2 diabetes mellitus, and use of canagliflozin 100 mg or 300 mg for a minimum of 6 months (unless discontinued due to side effects or cost issues). Exclusion criteria included: patients with renal impairment (GFR < 45 mL/min/1.73 m2; 0.75 mL/s/1.73 m2), patients with type 1 diabetes mellitus, patients with any other change in medication for diabetes (except insulin), hypertension (except diuretics) or lipid medication therapy during the evaluation period, and patients receiving prescription medications for weight loss during the evaluation period (Table 1).
Study inclusion and exclusion criteria.

A data collection form was utilized to collect the following patient information: baseline patient demographic information (age, gender, and race), duration of diabetes, medical history, current medications, laboratory data (HbAlC, cholesterol profile, serum creatinine, blood urea nitrogen (BUN), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels), blood pressure, height, weight, and reported adverse drug events. Drug efficacy was evaluated by a comparison of HbAlC levels, weight, blood pressure, and cholesterol profiles of patients on daily canagliflozin. Drug safety was evaluated by review of BUN and serum creatinine data as well as by review of documented reports of drug side effects.
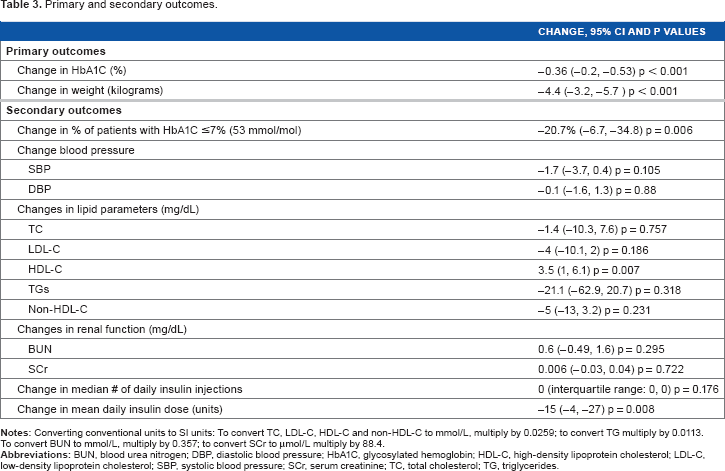
Primary study outcomes were changes in HbAlC and weight, and percentage of patients reporting adverse effects of therapy. Secondary outcomes were differences in the percentage of patients achieving an HbAlC level of <7% (53 mmol/mol), changes in systolic and diastolic blood pressures, changes in lipid levels (TC, LDL-C, HDL-C, TGs, and non-HDL-C), changes in BUN and serum creatinine levels, change in the number of insulin injections per day, and change in the average daily insulin dose.
Statistical analysis
As this was a pre-post observational study, each patient served as his/her own control. Statistical analysis was performed using paired t tests, the Fisher exact test, and the Wilcoxon signed rank test, as appropriate. P values <0.05 were considered statistically significant.
Results
The computerized text search of EMRs identified 256 possible study candidates. Of these, 47 patients were excluded because of a lack of a six-month or later follow-up appointment (despite receiving therapy for at least six months), 77 were excluded as they had received therapy for a duration of less than six months, 13 patients were excluded because of a change in their diabetes medication regimens while receiving canagliflozin, and 8 patients were excluded because of a diagnosis of type 1 diabetes mellitus.
The remaining 111 patients met the study criteria. Demographic and baseline characteristics of the study population are listed in Table 2. Overall, this was a middle-aged, morbidly obese, Caucasian population, with an average duration of diabetes of 12 years, who were already receiving a median of three diabetes medications. At baseline, three-quarters of patients received metformin therapy, almost two-thirds received insulin, and nearly 60% received GLP-1 analog therapy. The use of sulfonylurea and meglitinide therapies was uncommon. Microvascular complications were documented in 43.2% of the study population, while 26.1% of patients had a history of macrovascular disease. At baseline, 93.7% and 96.4% of patients were receiving lipid lowering (median of 1; mean of 1.4) and antihypertensive agents (median of 2; mean of 1.8), respectively.
Patient demographics and baseline characteristics.

Patients received canagliflozin for an average of 9 ± 2 months (range 6-12) of therapy. Two-thirds of patients received a daily canagliflozin dose of 300 mg; the remaining third of patients received 100 mg daily. During this time, HbA1C and weight significantly decreased, by an average of 0.37% and 4.4 kg respectively (Figs. 1 and 2). Furthermore, HDL-C levels significantly increased (3.5 mg/dL; 0.091 mol/L) (Table 3). In addition, 20.7% more patients receiving canagliflozin achieved an HbAlC of <7% (53 mmol/mol) at follow-up (p < 0.05), compared to baseline, and the mean daily insulin dose significantly decreased by 15 units from an average daily dose of 85 units. There were no significant changes in blood pressure, other lipid levels, BUN or creatinine levels, or number of daily insulin injections.
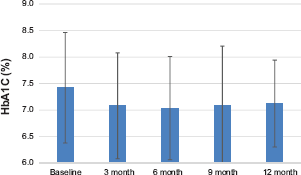
Changes in HbA1C.

Changes in weight.
Primary and secondary outcomes.
The overall rate of drug discontinuation was 27%, with 11.7% (13 patients) discontinuing because of third party payer/cost issues, and 15.3% (17 patients) discontinuing therapy due to adverse effects. Six of these patients reported balanitis and two patients reported vaginal yeast infections. Other reasons for drug discontinuation included hyperglycemia (n = 2), polyuria (2), urinary tract infection (2), stomach upset (1), fatigue (1), and atrial fibrillation (1). There were no reports of hypoglycemic events, hyponatremia, hyperkalemia, or renal insufficiency. An additional four of the 111 patients reported adverse drug events but continued therapy; one patient developed a urinary tract infection that resolved with ciprofloxacin treatment; two patients complained of orthostasis from the medication, and one patient developed two yeast infections, which resolved with fluconazole therapy.
Discussion
This is the first reported observational study regarding the real-world safety and efficacy of the SGLT-2 inhibitor canagliflozin, in patients with T2DM concomitantly receiving other classes of anti-hyperglycemic agents. Patients in this study demonstrated significantly reduced HbAlC and weight and a significant increase in mean HDL-C levels with the addition of canagliflozin.
This study reported a modest decrease in mean HbAlC level with the use of canagliflozin compared to results from randomized controlled trials. The Canagliflozin Treatment and Trial Analysis (CANTATA) trials reported mean reductions in HbAlC ranging from 0.73-1.03% after 26 or 52 weeks of therapy.8–12 The mean 0.36% reduction demonstrated in this study may be due to the lower average HbAlC at initiation of drug therapy compared to that seen in the controlled clinical trials (7.5% [58.5 mmol/mol] vs. 8.0% [63.9 mmol/mol]). It is well documented that reduction in HbAlC is less at lower baseline levels of HbAlC versus higher baseline levels. 13 In addition, HbAlC reduction in this study was achieved despite a 17.6% reduction in mean insulin dose. Figure 1 demonstrates the consistent glycemic effect over 12 months.
In addition to improved glycemic profiles, canagliflozin therapy provided statistically significant and clinically relevant weight reductions in T2DM patients originally managed with other anti-hyperglycemic agents. This study demonstrated a significant mean reduction in body weight of 4.4 kg (3.95%). This result is consistent with those of the CANTATA trials, which reported mean weight losses of 2.2-4.2% in patients in whom canagliflozin was added to a baseline regimen of metformin, sulfonylurea, metformin with pioglitazone, or metformin with sulfonylurea.8–12 Figure 2 shows the change in weight over 9 months. As there were only 23 patients with weight data at baseline and 12 months, these results are not presented. (However, weight in these 23 patients decreased from 123.5 ± 35.4 kg to 117.3 ± 33.3 kg).
In our patient population, 63.1% of patients received insulin therapy at baseline. Patients receiving insulin were able to decrease their insulin doses by a mean of 15 units per day from an average of 85 units; this may have contributed to the weight loss. Several studies evaluating the addition of SGLT-2 inhibitors to insulin therapy have reported similar reductions in insulin doses.8–12 Finally, 59.5% of patients in this study received GLP-1 analog therapy at baseline. Bell recently published a case report of a patient with a 13.2 kg (11.8%) weight loss over a 4-week period using GLP-1 agonist therapy in combination with canagliflozin. 14
This study did not demonstrate any significant reduction in mean systolic blood pressure (SBP). In contrast, four of five of the CANTATA trials reported significant reductions in SBP, ranging from –2.9 to –5.1 mmHg. One explanation for the apparent lack of SBP reducing effect in this study could be the well-controlled SBP at baseline (124 mmHg). The CANTATA trials reported mean baseline SBPs of 126–130 mmHg. Another reason for the apparent lack of SBP reduction in this study could be the fact that diuretic therapy was typically discontinued or the dose reduced by 50% at the initiation of canagliflozin therapy. This was done in an abundance of caution to prevent potential orthostasis from the osmotic diuretic response associated with canagliflozin therapy.
Comparable to the CANTATA studies, this study found a significant increase of HDL-C levels (3.5 mg/dL; 0.091 mol/L) with the treatment of canagliflozin. However, unlike the controlled clinical trials, this study found no changes in other lipid levels. In the CANTATA studies, canagliflozin use was associated with significant increases in non-HDL-C of 2.1–5.1 mg/dL (0.05–0.13 mmol/L) (1.5–3.6%) from a baseline of 140–147 mg/dL (3.62–3.8 mmol/L), while LDL-C levels increased by 4.4–8.2 mg/dL (0.114–0.212 mmol/L) (4.5–8%), from a baseline of 104–110 mg/dL (2.7–2.85 mmol/L). In contrast, baseline lipid levels in our patient population included a mean non-HDL-C of 114 mg/dL (2-95 mmol/L) and LDL-C of 79 mg/dL (2.05 mmol/L).
Controlled clinical trials have identified the following as the most common adverse effects associated with canagliflozin use: female and male genital mycotic infections, urinary tract infections, pollakiuria, and thirst. These side effects are consistent with the mechanism of action of the drug. As a standard of practice, patients were typically counseled on appropriate medication administration and possible adverse reactions prior to the initiation of treatment. Adverse drug effects were reported by 18.9% of this study population, and canagliflozin was discontinued by 15.3% of patients because of adverse events, with 11 of the 17 discontinuations (64.7%) attributable to the common side effects listed above. One of these patients discontinued medication because of new-onset atrial fibrillation, which occurred within a week of drug initiation. This adverse event could have been caused by possible changes in serum electrolytes. Weir et al reported changes in serum electrolytes, including a decrease in serum potassium, associated with the osmotic diuresis resulting from canagliflozin therapy. 15
SGLT-2 inhibition possesses a unique mechanism of action for the treatment of diabetes, addressing the last of the underlying defects of the ominous octet of T2DM pathophysiology. 2 In healthy individuals with a glomerular filtration rate of greater than 90 mL/min/1.73 m2 (1.5 mL/s/1.73 m2), approximately 180 L of plasma are filtered through the kidneys each day, which translates to approximately 180 grams of filtered glucose daily. There is a proportional relationship regarding the amount of plasma glucose concentration and filtered glucose. All filtered glucose is reabsorbed until the resorptive capacity of the tubules is reached. In patients without diabetes, the renal threshold (the blood glucose level at which glycosuria begins) is approximately 180 mg/dL (10 mmol/L). In patients with T2DM, the glucose renal threshold is approximately 240 mg/dL (13.3 mmol/L). 16 SGLT-2 inhibitor therapy resets the renal threshold to approximately 70–90 mg/dL (3.9–5 mmol/L), and by doing so increases urinary glucose excretion in patients with hyperglycemia. This results in a decrease in plasma glucose, an osmotic diuresis, and a net caloric loss of approximately 400 kcal per day, 11 thus promoting weight loss as well as a decrease in HbAlC. 17
SGLT-2 inhibitors reduce fasting and post-prandial glucose levels and their unique pharmacologic mechanism of action is independent of insulin secretion. One would therefore expect it to be effective regardless of the duration of diabetes. Because insulin levels are not increased with the use of SGLT-2 inhibitors, they have a placebo-like risk of hypoglycemia when used alone or with diabetes medications that don't cause hypoglycemia. Lastly, SGLT-2 inhibitor therapy is additive to that of other diabetes medications. Canagliflozin was approved for use by the FDA in March of 2013 and represents the first SGLT-2 inhibitor approved in the US.
There are several limitations to this study. First, cause and effect cannot be established as this was not a prospective study. For example, this study did not control for diet, exercise, frequency of glucose monitoring, or timing of canagliflozin administration. Although food does not affect bioavailability, taking canagliflozin before a meal may delay intestinal glucose absorption, 18 thereby reducing postprandial hyperglycemia. All of these factors could affect glucose control. Second, the sample size was relatively small. Significant changes in other outcomes may have been demonstrated with a larger sample size. Third, this study did not assess patient compliance. In a real-world (non-study) setting, a once-daily oral therapy could lead to less missed doses compared to oral medications or injections with multiple frequencies. Fourth, this study consisted of a relative homogenous patient population, a predominately white (92.8%), middle-aged (59 ± 9 years) population of patients with long-standing (12 ± 7 years) diabetes. It is possible that the results demonstrated here may not be reflective of other, more diverse patient populations. Finally, as data were collected by review of EMR, only documented adverse effects were captured. It is possible that more adverse effects occurred than were reported.
Conclusion
In this pre-post observational study, canagliflozin therapy was associated with significant reductions in HbAlC and weight, and a significant increase in mean HDL-C levels. Canagliflozin was generally well tolerated with an adverse effect profile consistent with that reported in controlled clinical trials. Overall, canagliflozin appears to be a useful therapeutic option in patients with T2DM who are inadequately controlled on other anti-hyperglycemic agents.
Author Contributions
Conceived and designed the experiments: AN, MPK. Analyzed the data: RAH. Wrote the first draft of the manuscript: AN, MPK. Contributed to the writing of the manuscript: AN, MPK, RSB, JW, RAH. Agree with manuscript results and conclusions: AN, MPK, RSB, JW, RAH. Jointly developed the structure and arguments for the paper: AN, MPK, RSB, JW, RAH. Made critical revisions: AN, MPK, RSB, JW, RAH. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgements
The authors acknowledge the assistance of Sara J. Micale, Pharm. D, for her contributions regarding the initiation of this project. In addition, the authors state that initial three-month results of this research were presented in poster format at the American Society of Health-System Pharmacy Mid-Year Clinical Meeting, December 10, 2013 in Orlando, FL.