
Abstract
Diffuse large b-cell lymphoma (DLBCL) is an aggressive and potentially curable lymphoma that presents itself as stage I-II in 30% of all cases. It is known that in these localized stages, 15-20% of patients treated without rituximab eventually relapse, but less data exist regarding rituximab era. We have analyzed clinico-pathological features and risk of relapse in 98 patients with I-II stage DLBCL in complete response (CR) or unconfirmed CR (CRu) after first-line treatment consisting of immunochemotherapy. Twelve patients (12.2%) eventually relapsed. Late relapse, more than two years after diagnosis, occurred in three patients, and early relapse, less than two years after diagnosis, was documented in nine patients. Median time from diagnosis to relapse was 0.61 years for patients with early relapse and 3.66 years for patients with late relapse. The second CR rate obtained was similar in the late and in early relapsing patients, being 33% versus 44% (p = 0.072), respectively. Three-year overall survival (OS) was 22% for early relapsing patients and 33% for late relapsing patients (p = 0.65). In conclusion, patients who are diagnosed with stage I-II DLBCL and achieve a CR/CRu with first line immunochemotherapy have a good prognosis. However, a proportion of patients relapse, and this is less frequent in patients treated with first line with immunochemotherapy. These patients have a poor prognosis.
Introduction
DLBCL is the most frequent subtype of lympho proliferative disorder in the Western world and constitutes approximately 30% of all non-Hodgkin's lymphoma. It presents as a localized disease, at stage I or II, in 30% of cases, and these patients have a good prognosis with complete response rates around 75-90% with chemotherapy without rituximab. The addition of rituximab improves the outcome of patients with the localized disease.1–3 However, in patients treated without rituximab, between 15 to 20% of these patients eventually relapse, mainly in the first 2 years following treatment. Late relapses4–7 are known to occur, but are considered rare events. This subgroup has been considered to have a better prognosis compared to early relapse patients. Most studies of relapsing patients are in patients treated without rituximab and little data exists regarding rituximab era. 8 The aim of the present study is to analyze the main clinicobiological features, relapse and the outcome of a series of patients diagnosed with localized DLBCL. These patients were followed-up in a single institution, in CR or CRu after first line treatment, mainly consisting of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) plus rituximab.
Patients and Methods
Patients
128 patients diagnosed with stage I-II DLBCL in a single institution between 2002 and 2011 were included in the study. 98 patients (76.5%) achieved a complete response (CR) or complete response unconfirmed (CRu). This group of 98 patients was the subject of the present study. The main initial features of these patients are described in the Results section and in Table 1.
Patient characteristics at initial diagnosis.

Histological Features
The diagnostic features of DLB-CL were based on the criteria established in the World Health Organization (WHO) classification Figure 1. 9 Morphologic and immunophenotypic studies were performed in all patients in Hospital Bellvitge based on usual routine practice. GC and non-GC profiles were defined according to the Hans algorithm. 10
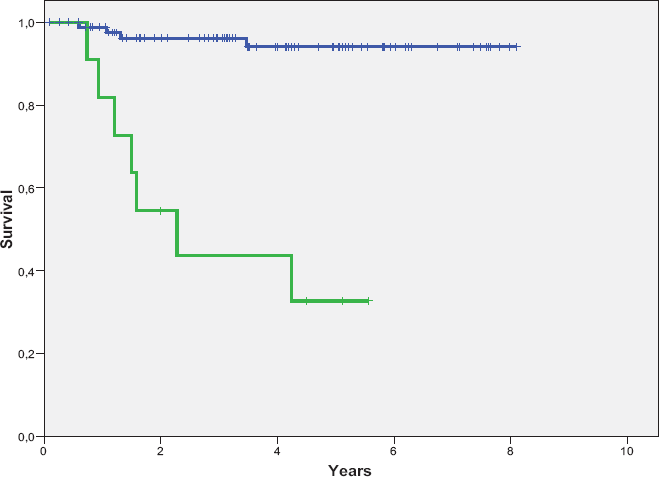
Overall survival of relapsing (green line) and no relapsing patients (blue line) (log-rank p < 0.0001).
Parameters Evaluated
The main clinicobiological variables of the patients were recorded and evaluated, including age, gender, performance status according to the Eastern Cooperative Oncology Group (ECOG) scale, presence of B-symptoms, Ann Arbor stage, nodal and extranodal involvement, bulky disease, bone marrow infiltration, serum lactate dehydrogenase (LDH), albumin and β2-microglobulin levels and International Prognostic Index (IPI), treatment given to the patients, duration of response, relapse/progression, cause of death and survival.
Informed consent was obtained from each patient according to the guidelines of the Ethics Committee of the ICO-Hospital Duran i Reynals. The procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional) and with the Helsinki Declaration of 1975, as revised in Edinburgh 2000.
Staging, Response, Evaluation and Follow-Up
Initial staging procedures included computed tomography (CT) of the thorax, abdomen and pelvis, bone marrow biopsy and positron emission tomography-computed tomography (PET-CT). These procedures were performed in 84 patients (86%). Post-therapy restaging included the repetition of the previously abnormal tests or biopsy. 11
Complete remission and unconfirmed complete response was defined according to the Cheson criteria. 12
The follow-up surveillance policy after treatment consisted of physical examination, blood counts and biochemistry, and chest roentgenogram (if initially abnormal) every 3 months during the first 2 years, every 6 months during the next 3 years and once a year thereafter. Thoracic and abdominal CT scans were performed every 6 months during the first year, every 8 months during the second year and yearly for the following 3 years.
Disease relapse or progression was defined as the appearance of new symptoms or signs of the disease as demonstrated by lymph node biopsy or other appropriate studies. At the time of relapse or progression, besides a new lymph node biopsy, CT scans of thorax, abdomen and pelvis, PET-CT scan, 11 as well as a bone marrow biopsy, were performed whenever possible. Patients relapsing within 2 years from the CR were considered as early relapsing patients and those relapsing after 2 years were considered as late relapsing patients.
Statistical Analysis
The multivariate analysis of the variables predicting a response was performed using a logistic regression. Progression-free survival (PFS) was measured from the date of first relapse until second relapse or death by any cause. Overall survival (OS) was measured from the date of first relapse until death from any cause or last follow-up evaluation. Survival data were computed according to the method described by Kaplan and Meier, and the curves were compared using the log-rank test.13,14 The multivariate analysis for survival was performed using the Cox model. Categorical data were compared using Fisher's exact test. All statistical analyses were carried out using SPSS 17.0.
Results
All Patients (N = 98).
Features
51 patients (52%) were males and 47 patients were females (48%). The median age of patients was 56 years, range (18-87). The main characteristics at initial diagnosis are presented in Table 1.
Initial Treatment and Response
All 98 patients received immunochemotherapy including rituximab at first-line treatment. Treatments including anthracyclines and all of these treatments incorporated CHOP and rituximab. Two patients received cyclophosphamide, vincristine, and prednisone (COP) and rituximab due to previous heart disease in both cases. Both cases received complementary radiotherapy.
Of the 96 patients treated with rituximab-CHOP (R-CHOP) regimens, 58 received 6 cycles and 11 received 6 cycles followed by radiation therapy. 15 27 patients received 3-4 cycles followed by radiation therapy. 16 The main reason to receive radiotherapy in large courses was bulky disease.
Outcome and Survival
Five year OS was 85%. With a median follow-up of 6.8 years, 11 patients died, 9 of them due to disease progression. 2 patients died in CR due to a sepsis and acute myeloblastic leukemia, respectively.
Relapsed Patients (N = 12).
Features
12 patients (12.2%) eventually relapsed. Late relapse occurred in 3 patients (3%) and early relapse in 9 patients (9.2%). 6 patients (50%) were males and 6 were females (50%) with a median age of 65 years, range (24-84). Median time-to-relapse was 0.61 years for patients at early relapse and 3.66 years for patients at late relapse. 8 patients were in stage II and 4 were in stage I at diagnosis. 3 of them (25%) had primary extranodal disease. The main characteristics at initial diagnosis and at relapse of relapsed patients are presented in Table 2, respectively.
Patient characteristics at relapse.

In patients with early relapse, a second biopsy was available in 8 of 9 cases and in all late relapsing patients. Histological subtype was the same at diagnosis and at relapse in all patients. At time of relapse, 6 (55%) had germinal center (GC) phenotype and 5 (45%) had non-GC phenotype. 2 of 3 late relapse were GC phenotype.
3 relapsing patients had received involved field radiotherapy at initial therapy. All relapses were outside the radiation field.
Treatment
All 12 patients received R-CHOP. Of these 12 patients, 9 received 6 cycles, 2 of them received 4 cycles followed by radiation therapy, and 1 patient received 6 cycles followed by radiation therapy.
At relapse, salvage regimens for patients were heterogeneous 17 : 6 patients received etoposide, cytarabine, cisplatin and prednisone (ESHAP) regimen plus rituximab, 3 patients received an ESHAP regimen and 1 patient received monotherapy with rituximab. 2 patients received palliative treatment.
Only 4 (30%) patients were consolidated by means of autologous transplant (ASCT), three at early relapse and one at late relapse.18,19
The reasons for not receiving ASCT included age (>65 years) in 2 cases, early progression of disease in 2 cases, death because of bleeding complication during salvage chemotherapy in 1 case and chemoresistant disease in 1 case.
Response
In terms of response rate at relapse, 5 patients (42%) achieved complete remission (CR), 2 (17%) partial remission, and 5 (41%) progression.
OS and PFS
OS at 3 years was 22% for patients at early relapse and 33% for patients at late relapse (p = 0.65).
Progression-free survival at 3 years was 22% for patients at early relapse and 33% for patients at late relapse (p = 0.23).
Univariate and Multivariate Analysis
Variables included in univariate/multivariate analysis at diagnosis were: age (< 60 vs ≥ 60 years), gender, Eastern Cooperative Oncology Group (ECOG) performance status, B symptoms, histological subtype, hemoglobin, lymphocyte count, serum lactate dehydrogenase (LDH), serum β2-microglobulin (β2M) levels, number of nodal and extranodal involved sites, Ann Arbor stage, bulky disease (defined as a tumor diameter >10 cm), bone marrow infiltration and the International Prognostic Index (IPI).
The most important variable predicting relapse at diagnosis was age, which was the only predictive variable in the multivariate analysis.
Discussion
DLBCL is an aggressive and potentially curable lymphoma that presents itself at stage I-II in 30% of all cases. In stage I-II between 15 to 20% of patients eventually relapse, mainly in the first 2 years following treatment mainly consisting of CHOP. The addition of rituximab improves the outcome of patients with the localized disease.1–3 However, little data exists regarding relapses in patients with localized DLBCL treated with R-CHOP.
In a review of the literature, Cabanillas et al 20 found an overall risk of late relapse in 503 patients with DLBCL who attained a CR of 6.8%. Lee et al 21 analyzed 127 patients with de novo advanced-stage DLBCL treated with MACOP-B. The risk of early relapse, defined like relapsing patients less than 2 years, in this series was 24.5% and 16% for late relapse.
Vose et al 22 analyzed 368 patients with DLBCL in CR after CHOP regimen. The risk of early relapse, defined as < 5 years, in this series was 36% and 8% for late relapse. They concluded that late relapsing patients had better prognostic characteristics, such as being in stage I-II, having normal LDH and having a performance score of >80% as compared to early relapsing patients.
Only 2 series analyzed risk of relapse in stage I-II. Sanz et al 23 analyzed risk of relapse in a series of 103 patients with DLBCL in CR after treatment including anthracyclines not containing rituximab. Risk of relapse of all series was 40%, 26% within 2 years (early relapse) from CR and 14% later than 2 years after CR (late relapse). In this series, in a separate analysis of I-II Ann-Arbor stage patients, risk of relapse for these patients was 16.5%, being 10.6% in patients with early relapse and 5.9% at late relapse. In a more recent paper, Larouche et al 24 analyzed a large series of 1492 patients with DLBCL relapse after 5 years following treatment based in anthracyclines like CHOP or doxorubicin, cyclophosphamide, vindesine, bleomycin, prednisone (ACVBP) mostly of them not containing rituximab. In this series risk of late relapse for localized patients, defined as more than 5 years, was 2.2%.
In our series, we examined 98 patients diagnosed with localized (stage I-II) diffuse large B-cell lymphoma in CR after receiving mainly R-CHOP. 12 patients eventually relapsed (12.2%): 9 (9.2%) before 2 years after CR (early relapse) and 3 (3%) after 2 years of CR (late relapse). It shows a lower frequency as previously published in patients treated with CHOP or CHOP like patients. 22 All patients relapsed with the same histological subtype, highlighting 2 of 3 (66%) late relapse with GC phenotype. Of the 10 patients that received salvage treatment, 5 patients (50%) achieved complete remission (CR), 2 (20%) partial remission, and 3 (30%) failed. Overall survival at 3 years was 22% for patients at early relapse and 33% for patients at late relapse (p = 0.65). In our series, only 4 patients received an autologous stem cell transplantation. This population is generally older, making it difficult to treat these patients with aggressive salvage regimens including transplant. In addition, this means that some of them receive palliative treatments.
The unique variable predicting relapse at diagnosis was age.
The main limitation of our study is the small number of relapsed patients, due to the good prognosis for these localized patients, and it does not allow us to make strong conclusions.
In conclusion, patients who are diagnosed with stage I-II DLBCL and achieve a CR/CRu to first line therapy have a good prognosis. However, a proportion of patients do relapse, and this is less frequent in patients treated during first-line therapy with immunochemotherapy. These patients have a poor prognosis.
Author Contributions
Conceived and designed the experiments: SM, EGB. Analyzed the data: SM. Wrote the first draft of the manuscript: SM, AO. Contributed to the writing of the manuscript: SM, EGB, AFS. Agree with manuscript results and conclusions: SM, AO, FC, EGB. Jointly developed the structure and arguments for the paper: SM, VR. Made critical revisions and approved final version: SM, FC, EDD, AO, VR, AFS, EGB. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.