
Abstract
Primary breast lymphoma (PBL) is a rare disease, and few clinicohistopathologic features of the disease have been discussed in previous studies. It represents 2.2% of extranodal lymphomas and constitutes 0.04% to 0.5% of malignant breast neoplasms, despite the clinical and radiographic similarities between breast lymphoma and carcinoma, the prognosis, as reported in the literature, varies. No consensus exists on the best way to treat PBL. However, radiotherapy and chemotherapy were used alone or in combination to treat various cases of PBL. We retrospectively studied 3 cases of PBL of the breast seen in patients attending a tertiary cancer center in Qatar, between 2012 and 2015, in an attempt to determine the common clinical features, therapy, and prognosis of PBL.
Introduction
Breast lymphoma is classified as primary breast lymphoma (PBL) or secondary breast lymphoma (SBL). The term PBL is used when the breast is the principal or, as in most cases, the only site of lymphoma. The term SBL is used when the breast is involved, but with other sites of lymphoma present. The distinction between PBL and SBL is sometimes difficult and in some series not clearly distinguished.1,2 Primary breast lymphoma is a rare tumor that originates from lymph tissues. The reported incidence is 0.04% to 0.5% of malignant breast tumors, 1% of all non-Hodgkin lymphoma (NHL) and 2% of extranodal lymphomas.3–7 Most of the PBLs are diffuse large B-cell lymphomas (DLBCL), but there are also other less frequent subtypes.7–11
Primary breast lymphoma is mainly found in female patients, accounting for 95% to 100% of all the patients with PBL. 12 It is very rare for men, and a limited number of cases have been reported in the literature so far. The range of the age is very broad; therefore, this kind of tumor can occur in any age group. Primary breast lymphoma is commonly found in only 1 breast, ie, the right breast, and especially in the upper quadrant of the right breast. 13
During the early 1970s, some researchers suggested collecting proper pathological samples, the close association of mammary tissue and lymphomatous infiltration and absence of disseminated lymphoma at the time of diagnosis before diagnosing any primary malignant breast lymphoma. 14 Patients with breast involvement as a result of progression or relapse of a previously diagnosed NHL are considered as SBLs. 15
Presentation and Management of Cases
Case 1
A woman in her 40s not known to have any chronic illnesses presented with history of progressively enlarging left breast mass for 6 months with no nipple discharge. She reported history of undocumented weight loss over the same period. On physical examination, the patient was found to have large firm, nontender left-sided breast mass almost occupying the entire left breast more in the upper inner quadrant measuring 8 × 10 cm with overlying erythema. She also had a palpable lymph node (LN) in the left axilla measuring 1.5 × 2 cm. The rest of her examination was unremarkable. The patient underwent breast biopsy and was found to have DLBCL (Figure 1), activated B-cell subtype, International Prognostic Index (IPI 3), with no central nervous system (CNS) involvement by cerebrospinal fluid (CSF) examination. Further workup revealed bulky disease with multiple extranodal localization (breast, muscle, and lung) stage IVB. The patient started on chemotherapy (R-CODOX-M/R-IVAC protocol) for a total of 4 cycles. She was associated with uncomplicated febrile neutropenia, otherwise had unremarkable hospital course, and achieved complete metabolic remission by positron emission tomography-computed tomography (PET-CT) (Image 1) followed by radiotherapy to the residual breast mass of 20 Gy in total. The patient lost follow-up as she traveled back to her home country after ending her treatment.

Histopathologic examination of breast mass in patient 1. (A) Diffuse proliferation of atypical large lymphoid cells in breast tissue (hematoxylin-eosin, original magnification ×40). Immunohistochemical studies demonstrate that atypical large cells are (B) positive for CD20 and (C) positive for BCL2. (D) Ki67 shows high proliferation rate of lymphoma cells.

(A) Evidence of stage IV disease on baseline 18F-FDG-PET/CT MIP image with nodal involvements on both sides of the diaphragm, splenic lesions, right adnexal mass, and right femoral solitary intramedullary focus. (D) Large FDG-avid mass demonstrated in the left breast averaging 13 cm in maximal dimension. (B) Interim evaluation after 2 cycles of chemotherapy showed a remarkable reduction in the FDG accumulation (∆SUVmax > 90%, visual score: 2) and size of the breast mass (E, arrow). Similar metabolic regression was observed at the right femoral intramedullary lesion (arrowhead). All the other lymphomatous manifestations have resolved. (C) Restaging scan did not show significant hypermetabolic activity, the mild tracer uptake detected within the morphologically further regressed left breast mass (F, arrow) and right femoral lesion (arrowhead) is compatible with complete metabolic remission. 18F-FDG-PET/CT indicates 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography; MIP, maximum intensity projection.
Case 2
A woman in her 40s known to have Hypertension (HTN) on treatment presented in with history of progressive left axillary enlarging LN associated with left breast skin changes in form of redness and swelling. The patient gave history of intentional weight loss of 3 to 5 kg over 1 month with anorexia and progressive generalized fatigability over the last 2 months before presentation. On examination, the patient was found to have generalized lymphadenopathy with erythema over left breast and diffuse left breast enlargement. Excisional biopsy from left axillary LN showed DLBCL. Staging workup by PET-CT (Image 2) revealed extensive involvement with multiple extranodal sites (breast, skin, pancreas, ovary, skeletal, gastric, and rectal) stage IVB, IPI 3 with no CNS involvement by CSF examination. The patient started on chemotherapy (R-CODOX-M/R-IVAC protocol) for a total of 4 cycles. She developed line-related sepsis that was culture negative, otherwise had unremarkable hospital course, and achieved complete metabolic remission by PET-CT followed by radiotherapy to the residual breast mass of 36 Gy in total. After 4 months of completion of therapy, she presented with right thigh pain radiating to hip with anorexia. Positron emission tomography-computed tomography was consistent with relapse mainly in infra-diaphragmatic region. The patient received salvage chemotherapy with R-DHAP 2 cycles and then went to Jordan and underwent autologous stem cell transplantation (SCT) in December 2014 in King Hussein Cancer Center in Jordan (KHCC). Positron emission tomography-computed tomography 100 days after transplant showed complete metabolic remission similar to the PET-CT done 1 year after transplant.

(A) Initial 18F-FDG-PET/CT MIP image demonstrated multiple intensely hypermetabolic extranodal masses (within superior vena cava and right atrium, bilateral breasts, left adrenal gland, bilateral adnexal region, and left lower abdominal wall) with the largest lobulated left breast lesion measuring 11 cm and presenting (D) SUVmax of 28. (B) Interim study performed after 4 cycles of chemotherapy revealed marked metabolic and morphological regression of left breast lesion (∆SUVmax > 80%) with residual moderate FDG uptake similar to the liver tracer uptake level (visual score: 3). (C) End-of-treatment 18F-FDG-PET/CT showed no metabolic evidence of lymphoma activity and no significant FDG uptake (equal to that of mediastinal blood pool activity) in left breast residual soft tissue density stranding likely to represent posttreatment fibrotic change. Regressing left breast mass is appreciated on fused 18F-FDG-PET/CT corresponding transverse sections (E, arrow), (F, arrowhead). 18F-FDG-PET/CT indicates 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography; MIP, maximum intensity projection.
Case 3
A woman in her 30s not known to have any chronic illnesses presented in with severe shortness of breath and symptoms of superior vena cava (SVC) obstruction with prominent veins, facial swelling, and fever. The patient had normal vaginal delivery 6 months before presentation when she noticed enlargement of her left breast attributed to breastfeeding and sought medical advice on several occasions. She was given oral antibiotics to treat recurrent mastitis, but her condition continued to worsen to the point of having SVC obstruction syndrome. On physical examination, the patient was febrile, found to have bilateral breast enlargements, with multiple masses more in the left breast. No palpable lymphadenopathy was noted. Breast biopsy showed DLBCL, and staging workup revealed (Image 3) extensive involvement with multiple extranodal sites (bilateral breast, cardiac, adrenal, and abdominal wall), stage IVB, IPI 3 with no CNS involvement by CSF examination. The patient started on chemotherapy (R-CODOX-M/R-IVAC protocol) for a total of 4 cycles, had unremarkable hospital course and then had favorable response with persistent fludeoxyglucose (FDG) activity in left breast. She went to UK and received 4 cycles of R-CHOP. She was advised to consolidate with radiotherapy, received total 50 Gy after finishing her treatment. Positron emission tomography showed complete metabolic remission. The patient has regular follow-up with hematology team.
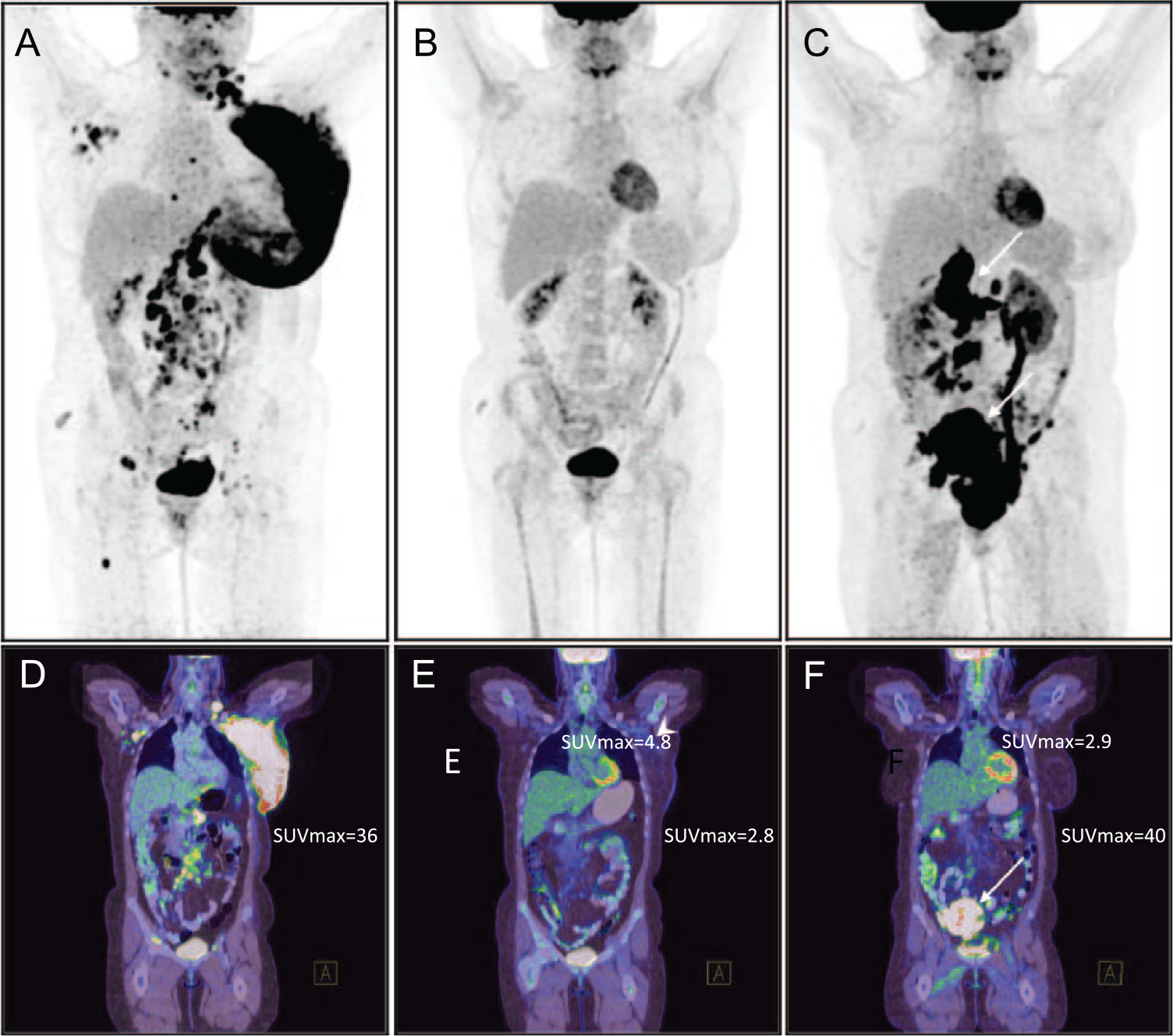
(A) Initial staging 18F-FDG-PET/CT MIP image depicted intensely hypermetabolic huge left breast axillary mass encasing the subclavian vessels inseparable from pectoralis minor muscle and (D) extensive skin infiltration. Organ involvements (pancreas, left ovary, and rectal wall), generalized lymphadenopathy, and multifocal skeletal lesions were presented. (B) After 4 cycles of interim chemotherapy study, practically complete metabolic treatment response in all initially involved sites with minimal (visual score: 2) FDG uptake correlating with left axillary ill-defined residual soft tissue stranding (E, arrowhead) and slightly thickened breast skin were observed. (C) Restaging follow-up 18F-FDG-PET/CT demonstrated intense hypermetabolic abdominal and bulky pelvic masses (F, arrows) consistent with disease relapse but no sign of lymphomatous activity above the diaphragm including the breast and axillary regions. 18F-FDG-PET/CT indicates 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography; MIP, maximum intensity projection.
All the 3 cases were treated with R-CODOX-M/R-IVAC protocol based on their high IPI score, the aggressiveness of the disease at presentation, and the poor prognosis being in unfavorable primary site with high risk of CNS relapse; taking into consideration the lack of autologous SCT in our center, and after thorough discussion in Multidisciplinary Team (MDT), it was decided to start with this aggressive protocol for the overall benefit of the patients.
Radiologic Findings
The diagnostic approach of PBL includes radiologic studies (mammography, ultrasonography [US], PET, and magnetic resonance imaging [MRI]), fine-needle aspiration cytology (FNAC), and immunohistochemical biomarkers. 16
Evidence of stage IV disease on baseline 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) maximum intensity projection (MIP) is shown in image (A) with nodal involvements on both sides of the diaphragm, splenic lesions, right adnexal mass, and right femoral solitary intramedullary focus. Large FDG-avid mass demonstrated in the left breast averaging 13 cm in maximal dimension is shown in image (D). Interim evaluation, as shown in image (B), after 2 cycles of chemotherapy showed a remarkable reduction in the FDG accumulation (∆SUVmax > 90%, visual score: 2) and size of the breast mass (E, arrow). Similar metabolic regression was observed at the right femoral intramedullary lesion (arrowhead). All the other lymphomatous manifestations have resolved. Restaging scan (C) did not show significant hypermetabolic activity, the mild tracer uptake detected within the morphologically further regressed left breast mass (F, arrow), and right femoral lesion (arrowhead) is compatible with complete metabolic remission (Image 1).
Initial 18F-FDG-PET/CT MIP image (A) demonstrated multiple intensely hypermetabolic extranodal masses (within SVC and right atrium, bilateral breasts, left adrenal gland, bilateral adnexal region, and left lower abdominal wall) with the largest lobulated left breast lesion measuring 11 cm and presenting SUVmax of 28 (D). Interim study (B) performed after 4 cycles of chemotherapy revealed marked metabolic and morphological regression of left breast lesion (∆SUVmax > 80%) with residual moderate FDG uptake similar to the liver tracer uptake level (visual score: 3). End-of-treatment 18F-FDG-PET/CT (C) showed no metabolic evidence of lymphoma activity and no significant FDG uptake (equal to that of mediastinal blood pool activity) in left breast residual soft tissue density stranding likely to represent posttreatment fibrotic change. Regressing left breast mass is appreciated on fused 18F-FDG-PET/CT corresponding transverse sections (E, arrow; F, arrowhead) (Image 2).
Initial staging 18F-FDG-PET/CT MIP image (A) depicted intensely hypermetabolic huge left breast axillary mass encasing the subclavian vessels inseparable from pectoralis minor muscle and extensive skin infiltration (D). Organ involvements (pancreas, left ovary, and rectal wall), generalized lymphadenopathy and multifocal skeletal lesions were presented. After 4 cycles of interim chemotherapy study (B), practically complete metabolic treatment response in all initially involved sites with minimal (visual score: 2) FDG uptake correlating with left axillary ill-defined residual soft tissue stranding (E, arrowhead) and slightly thickened breast skin were observed. Restaging follow-up 18F-FDG-PET/CT (C) demonstrated intense hypermetabolic abdominal and bulky pelvic masses (F, arrow) consistent with disease relapse but no sign of lymphomatous activity above the diaphragm including the breast and axillary regions (Image 3).
Histologic Diagnosis
Histopathology examination of breast mass biopsies of patients 1 and 2 showed a diffuse lymphoid proliferation. Most of the cells are large lymphoid cells with atypical irregular nuclei having a vesicular chromatin and variably prominent nucleoli with scattered mitotic figures. Immunohistochemical studies performed confirmed the diagnosis of DLBCL (CD45+, CD20+, BCL2+) with high Ki67 expression. The DLBCL in the first patient is of germinal center origin (CD10+) and in the second patient it is of activated B-cell origin (CD10−, BCL6+, MUM1+). Histopathologic examination of left axillary LN of patient 3 showed DLBCL of germinal center origin (CD10+) (Figure 1).
Discussion
Primary breast lymphoma is an unusual condition with poor clinical outcome. Breast lymphomas present less than 0.5% of malignant breast neoplasms and 2.2% of extranodal lymphomas. 17 So health care providers handling breast carcinomas should be aware and able to recognize its clinical presentation, management, and prognosis compared with usual breast carcinoma cases.
With the current advancement in diagnostic testing, reporting of PBL is increasing, which proves the significance of holistic information about this rare disease. It is predominantly (95%-100%) reported among female patients and is very less prevalent in men, 13 as all the 3 reported cases are women. Approximately, 1% to 14% of all PBL cases have bilateral breast lymphomas. 18 In all of our 3 patients, the breast lump was detected on the left side. The investigational findings of our cases showed a DLBCL of germinal center origin (cases 1 and 3), whereas case 2 showed activated B-cell origin.
Based on the histopathologic findings, breast tumors can be categorized as large cell B-cell lymphomas, monocytoid B-cell lymphomas, and undifferentiated lymphomas. 12 Most of the patients with PBL have a DLBCL and B-cell lineage, which accounts for 40% to 70% of all breast lymphomas with features of non-germinal center cells. 13 The assessment of our 3 cases revealed DLBCL of the breast (CD45+, CD20+, BCL2+) with high Ki67 expression in 2 cases, which is consistent with the existing literature.
The diagnosis of PBL includes radiologic investigations (mammography, US, MRI, and PET), immunohistochemical biomarkers, and FNAC. 19 Accurate diagnoses are crucial for staging and grading of this type of malignancy and also to help in monitoring the patient’s response to treatment.
Treatment of PBLs follows treatment guidelines for lymphomas of the same stage in other locations. The choice of chemotherapy should be based on histologic subtype, disease extent, and the individual patient. 17 Mastectomy has no benefit to the treatment of PBL. Nodal status predicts outcome and guides the optimal use of radiation and chemotherapy.16,18,20 On review of literature, most of the cases of primary DLBCL were treated by R-CHOP “the standard of care for DLBCL,” some were followed by radiotherapy with variable outcome, and none of the cases have been treated with R-CODOX-M/R-IVAC “the standard protocol for Burkitt lymphoma.”
Two of our patients treated with R-CODOX-M/R-IVAC (rituximab, cyclophosphamide, doxorubicin, vincristine, methotrexate/ifosfamide, etoposide, and high-dose cytarabine) protocol as first line of treatment were followed by radiotherapy: one patient lost to follow-up as she traveled back to her home country and the other patient relapsed shortly after radiotherapy and underwent autologous SCT and still maintaining remission till date. It is not clear whether R-CODOX-M/R-IVAC protocol is superior to R-CHOP in the treatment of primary DLBCL of the breast and needs further studies.
Review of literature on PBL-DLBCL with treatment details and the outcomes is summarized in Table 1.
Summarizing the review of literature on PBL-DLBCL with treatment details and outcome.

Abbreviations: CNS, central nervous system; CR, complete response; DLBCL, diffuse large B-cell lymphoma; NA, not applicable; PBL, primary breast lymphoma; PR, partial response; SCT, stem cell transplantation.
Conclusions
The authors report an unusual case series of 3 female patients with PBL. Early recognition of PBL based on advanced radiologic and histopathologic investigations is useful for identification of this condition. Furthermore, accurate staging and grading of PBL are crucial for selecting the appropriate treatment modalities to avoid mastectomy.
Footnotes
Peer review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 533 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AB conceived and designed the paper. AB, EK, and AN analyzed the data and wrote the first draft of the manuscript and jointly developed the structure and arguments for the paper. AN, HO, HE, MY contributed to the writing of the manuscript. EK, ZH, SA, SK, and DS agree with manuscript results and conclusions. EK, ZH, HO, HE, SA, SK, DS, and MY made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.