
Abstract
Diffuse large B-cell lymphoma (DLBCL) accounts for 30% to 40% of the newly diagnosed adult non-Hodgkin lymphomas, but rarely presents in leukaemic phase. Here in, we report a case of DLBCL presenting in leukaemic phase and masquerading as acute leukaemia. A 28-year-old woman presented to our outpatient department with complaints of fever for 1 week. Her peripheral blood smear showed 5% to 8% blasts. Bone marrow aspirate showed an infiltration by ~30% blasts. Flow cytometry and immunohistochemistry confirmed relapse of DLBCL. Also, patient’s poor response to therapeutic regimen for DLBCL prompted to consider second differential diagnosis of acute leukaemia. This case is a learning case, as it emphasizes the combined role of diagnostic ancillary techniques along with clinical judgments for management. The case also makes us more vigilant towards the pathobiology of DLBCL and dynamics of personalized individual treatment response.
Case History
A 28-year-old woman presented to our outpatient department with complaints of fever, night sweats, lassitude, and abdominal bloating for 1 week. Her general and physical examination was normal. The ultrasonography (USG) abdomen revealed mild splenomegaly and abdominal lymphadenopathy. Her complete hemogram showed haemoglobin value of 10.5 gm/dl, total leucocyte count of 10 300 mm−3 and platelet count of 90 000 mm−3. Peripheral blood Fig1(b) smear showed 5% to 8% blasts. Bone marrow aspirate smears were cellular and showed infiltration by ~30% myeloperoxidase (Fig 1(a)) (MPO) negative blasts with scant to moderate amounts of agranular, pale basophilic cytoplasm with rare vacuolations, irregular nuclei with dispersed chromatin, and multiple prominent nucleoli. At this point, morphologic diagnosis of MPO negative acute leukaemia, possibly acute monoblastic leukaemia was considered. Flow cytometry with a limited panel of markers showed bright CD45 with absence of CD34, CD14, cMPO, cCD3 lowering the possibility of acute leukaemia. A discussion with the clinician revealed that the patient had in fact generalized lymphadenopathy 6 months back and was evaluated elsewhere. Biopsy from the lymph node then was diagnosed as diffuse large B-cell lymphoma (DLBCL). Positron emission tomography–computed tomography (PET CT) showed extensive involvement of cervical, retroperitoneal, and mediastinal lymph nodes, bone marrow, and spleen. She had received 1 cycle of RCHOP (Rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and 6 cycles of DA-EPOCH (Etoposide, Prednisone, Vincristine, Cyclophosphamide, Doxorubicin) chemotherapy followed by abdominal external beam radiotherapy. Interim PET CT after 4 cycles of chemotherapy showed partial remission and after 6 cycles showed complete response. The patient relapsed after 2½ months and the PET CT done was suggestive of recurrence. She had received a mini BEAM and later came to our institute. Positron emission tomography–computed tomography repeated in our institute was also suggestive of bone marrow relapse. In light of this valuable history, we narrowed our diagnosis and did further panel of markers which showed the side scatter (SSC)/CD45 gated cell cluster was negative for CD34, CD13, CD33, CD117, CD14, CD3, and CD7 and positive for CD10, sIgM, and CD19. Subsequently, cells gated on SSC/CD19 were positive for CD20, CD22 and negative for CD23. Considering the morphology and flow markers, differential diagnosis considered were high-grade B-cell lymphoma (HGBL) (fig 2), DLBCL in leukaemic phase was rendered. Bone marrow Fig (1c) and retroperitoneal lymph node Fig 1(d) biopsies revealed diffuse involvement by atypical lymphoid cells, positive for CD20, CD10, BCL2, and BCL6, negative for cyclin D1 and c-MYC with a high Ki-67 labelling index (85%) fluorescent in situ hybridization (FISH) done by dual colour break apart probe was negative for c-MYC rearrangements (fig e-h). High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements was excluded as c-MYC was negative by FISH and its rarity of blastoid morphology. High-grade B-cell lymphoma, not otherwise specified (NOS) has features intermediate between DLBCL and B-cell lymphoma (BL) or appear blastoid, but do not harbour a genetic double hit. The negative c-MYC also excluded the possibility of double and triple hit lymphomas. So the final diagnosis was given as DLBCL, in leukaemic phase. Review of the outside bone marrow biopsy slides showed near total replacement by atypical lymphoid cells which was CD20 positive and negative for CD3, TdT, and cyclin D1 being consistent with the present diagnosis of B-cell non-Hodgkin lymphoma (NHL) infiltration of the marrow. Although the patient was diagnosed as high-grade NHL infiltrating the bone marrow, strongly favouring DLBCL, she was started on R-BFM-90 protocol, in view of the relapse with DA-EPOCH. The patient attained complete remission of bone marrow post induction, but later, she died due to disease progression. The point of interest in our case was the morphology and importance of eliciting proper history. The blastoid appearance of the atypical lymphoid cells made acute leukaemia top the list of differential diagnoses against NHL infiltration. Also, the patient’s poor response to 6 cycles of DA-EPOCH prompted the medical oncologists to consider acute leukaemia higher in their list of differential diagnoses.

(A) Peripheral smear showing blasts. Jenner Giemsa ×400. (B) Cellular bone marrow with infiltration by large blasts scant to moderate amounts of agranular, pale basophilic cytoplasm with only rare vacuoles, and irregular nuclei with dispersed chromatin and multiple prominent nucleoli. Jenner Giemsa ×400. (C) Bone marrow biopsy showing near total replacement of the marrow by large atypical lymphoid cells. H & E stain, ×200. (D) Retroperitoneal LN biopsy, shows diffuse effacement by large atypical lymphoid cells with hyperchromatic nuclei, frequent mitosis. H & E stain, ×400. (E) CD20 diffuse membranous positivity, ×400. (F) Bcl-2 IHC, diffuse membranous positivity, ×400. (G) Bcl-6 IHC, diffuse nuclear, ×400. (H) Ki-67 labelling index is ~80% to 90%, ×400. H & E indicates haematoxylin and eosin; LN, lymph node; IHC, immunohistochemistry.
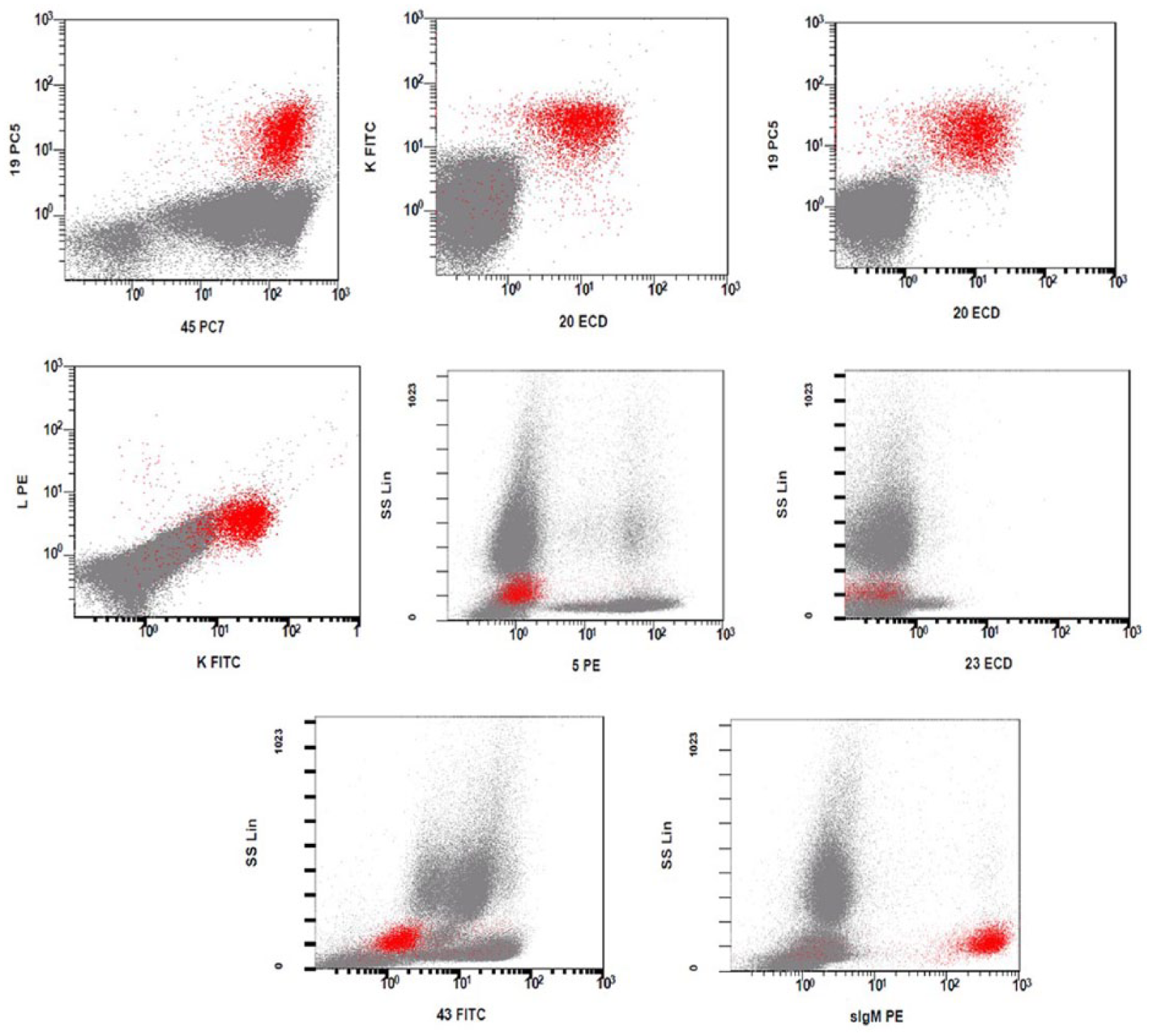
Side scatter (SSC)/CD45 gated cell cluster was positive for CD19, CD10, CD20, CD22, kappa, sIgM, and negative for CD34, CD13, CD33, CD117, CD14, CD3, CD7, and CD23. FITC indicates fluorescein isothiocyanate;
Discussion
Bone marrow infiltration by neoplastic circulating cells may occur in lymphomas, giving rise to a leukaemic phase, which may be noted during lymphoma progression or rarely at diagnosis. The flowcytometric immunophenotyping done on bone marrow or peripheral blood can help early diagnosis. 1 DLBCL rarely presents a leukaemic phase unlike other lymphomas such as mantle cell lymphoma, follicular lymphoma, anaplastic large cell lymphoma, and in terminal phases of all refractory lymphomas. 2 Although the morphology was consistent with acute leukaemia in our case, the immunophenotypic profile favoured a mature/non-blastic B-cell neoplasm, as evidenced by the expression of B-cell antigens, bright CD45, and absence of CD34. With blastoid morphology, light chain surface immunoglobulins should be included in the panel to arrive at correct diagnosis.3-5 The pathogenesis of migration of lymphoma cells into the bloodstream in various lymphomas is unclear. A differential expression of adhesion molecules has been proposed as a possible mechanism for the migration of lymphocytes from the lymph nodes, but there are no conclusive studies.6,7 Patients with DLBCL, in the leukaemic phase are prone to have extranodal involvement besides the bone marrow, bearing a high tumour burden. Data from 1 cohort of 29 patients showed the involvement of the spleen in 62%, pleura/lung in 41%, liver in 21%, bone in 17%, bowels in 7%, and cerebrospinal fluid in 14% of cases. Of these patients, 90% received anthracycline-based regimens with rituximab, which was associated with early mortality (14% vs 6% in patients with DLBCL treated with RCHOP), but yields approximately 50% at the 4-year survival analysis, which is comparable to the overall survival in patients with DLBCL and a high International Prognostic Index Score and no leukaemic presentation. 6 Our patient had bone marrow involvement and splenomegaly.
This case presented here is interesting as it provides many learning points. First, the clinical presentation and morphology can be rather deceptive without adequate history. Second, it highlights the application of flowcytometric immunophenotyping to distinguish acute leukaemia from NHL in blastic phase. Third, DLBCL in leukaemic phase could respond better to BFM-90 rather than DA-EPOCH protocol.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PB,PR,SM,PT: manuscript writing, diagnostic Workup. LK: Primary Medical Oncologist.