
Abstract
The treatment gap between conservative management and total knee arthroplasty may leave patients with moderate cases of knee osteoarthritis (OA) without an ideal treatment option. The KineSpring® Knee Implant System may be a viable treatment option to fill the treatment gap for patients with knee OA who are not willing or inappropriate candidates for total knee arthroplasty, yet do not demonstrate relief with conservative treatments. This current paper reports a series of patients who received the KineSpring System and were followed for five years. Twelve patients were included in the case series. All 12 patients were diagnosed with symptomatic OA of the medial compartment of the knee. Pain and functional problems associated with OA improved with treatment using the KineSpring System. Furthermore, these improvements were seen over the course of five years. The findings of this study show the KineSpring System as a promising intervention for early-onset OA and warrant further investigation regarding its effectiveness.
Introduction
Osteoarthritis (OA) is a disease characterized by the painful deterioration of the joint structures, primarily the cartilage and subchondral bone. 1 Knee OA is prevalent worldwide,2–4 and it limits mobility and quality of life because of increased chronic stiffness and pain. 1 Mild cases of the disease can initially be treated conservatively, with braces 5 and exercise, 6 but, as cases become more severe, surgery is often required. In the most severe cases, total knee arthroplasty (TKA) is often performed. 7 This involves the complete replacement of the knee joint, is a highly invasive procedure, which is associated with continued long-term pain, and is substantially less successful in younger patients.7–9 The surgery is also expensive.10–12 Consequently, TKA should be used as a last resort for the most severe cases of knee OA, 7 and the development of new interventions, especially for younger patients, is encouraged. 13
The differences between conservative management and TKA may leave patients with moderate cases of knee OA without an ideal treatment option. 14 This belief is reflected by health care professionals, with the majority of those surveyed agreeing that a treatment gap exists for early-onset knee OA. 15 The need for alternative treatment may be a sentiment shared by patients, as many with severe OA of both the knee and hip are unwilling to undergo a total joint replacement. 16 Research has indicated that patients would rather wait until their symptoms worsen before undergoing the procedure. 17 A less-invasive method may solve both the perceived treatment gap reported by physicians14,15 and the concerns of patients. 16
One possible alternative is the KineSpring® Knee Implant System. In brief, the device consists of two base plates: one fixed to the femur and the other to the tibia, with an absorber piece connecting the two sites. This reduces the load on the knee up to 30 lbs during full extension and is designed primarily for individuals with mild-to-moderate knee OA. 18 Initial research has demonstrated that potential patients are willing to try the KineSpring System before other surgical options, primarily because of its low complication rate and complete preservation of native anatomy. 19
The KineSpring System has a growing body of literature to support its use, stemming from initial testing in an ovine model. Experimentation demonstrated no complications that could be attributed to the device specifically and that it replicated healthy joint behavior. 20 Successful implantation of the KineSpring System in human patients was reported by Hayes et al. 21 , in a 51-year-old female patient followed for three years and a 53-year-old obese male patient followed for one year. Significant improvements in pain and knee joint function occurred for both patients. Furthermore, these individuals chose to undergo surgical installment of the KineSpring System over a high tibial osteotomy (HTO) procedure. Both patients had previously undergone a HTO in their opposite leg and were not satisfied enough with the results to experience the procedure a second time. 21
While several studies have examined the effectiveness of the KineSpring System, the majority of these examine the effectiveness of this device only up to two years.22,23 This current paper reports a series of patients with moderate knee OA who received the KineSpring System and were followed for five years.
Methods
Patients
This case series included 12 patients who were followed for five years. The patients were enrolled at four clinical sites in Australia (two hospitals in Sydney and two hospitals in Brisbane). Inclusion criteria and exclusion criteria are listed in Table 1. Kellgren–Lawrence grading of the knee was determined by MRI and standing radiographs. Employment history, including the amount of physical labor, was acquired through a questionnaire.
Inclusion and exclusion criteria.

Ethics
The current report analyzes a series of patients who were enrolled in the Safety and Feasibility of a Load Bypass Knee Support System for the Treatment of Osteoarthritis (OASYS Trial). The OASYS Trial was registered at the Australian New Zealand Clinical Trials Register (ANZCTR) as ACTRN12608000451303. Human Research Ethics Committee approval from each site (St Vincent's and Holy Spirit Health Limited, Mater Health Services, and the Northern Hospital Network) was obtained prior to initiation of the investigation. Written informed consent was obtained from participants, and the study complied with the principles of the Declaration of Helsinki.
Device Details
Each of the 12 patients received the KineSpring System (Moximed Inc.), which is a load-bypassing knee support system. Two contoured base plates are fixed using bone screws: one plate on the femur and one on the tibia. A link absorber piece connects the two pieces over the knee joint. 18 The KineSpring System does not alter the joint directly, but rather, functions extracapsularly by partially absorbing the load across the joint. Consequently, the implant preserves natural kinematics (Fig. 1).
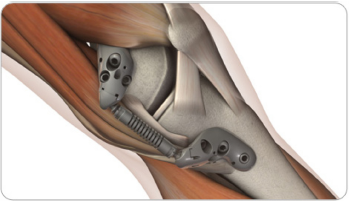
KineSpring System Implant.
Operative Details
Standard preoperative procedures were performed on each patient. The patient was placed under general anesthesia, with their knee accessible while in full extension and in a true lateral position. The medial epicondyle was used as a reference point for a K-wire that was used to position the femoral base of the device. A mean incision of 7–8 cm was made, and the Musculus vastus medialus was elevated, and then retracted anteriorly and laterally. This provided the bone exposure needed to remove unnecessary periosteum and properly attach the base component. The plate was placed onto the bone and fixed using compression and locking screws. A mean incision of 7–8 cm was made 60 mm from the K-wire along the tibial shaft. An extracapsular tunnel was created, wherein the absorber unit would reside beneath the soft tissue of the medial knee. The absorber unit was pulled into the tunnel, and then attached to the femoral base unit. The tibial base piece was then fixed to the bone in much the same way as described for the femoral piece. The knee was then rotated through deep flexion and full extension, and the wounds were closed in a standard fashion.
Patient Follow-Up
Patients were medically assessed at two and six weeks, three and six months, and then annually for five years. All assessments were performed at the orthopedic clinic where the surgery had initially taken place. At baseline, and starting on the appointment at six weeks postsurgery, additional measurements were collected for analysis: Western Ontario and McMaster Universities Arthritis Index (WOMAC) pain and functions scores, 24 Knee Society Scores (KSSs) 25 for knee and function, and the degrees of knee flexion represented as the range of motion (ROM). Baseline measurements were completed within 90 days of the procedure. All WOMAC scores were standardized according to previously outlined methods. 26
The WOMAC is a multidimensional health status instrument for patients with OA of the hip and knee, comprising pain, stiffness, and physical function subscales. 24 The current study used the normalized 100 mm VAS version of the WOMAC, where a higher score represents increased pain or decreased function, depending on the subscale. 24 The KSS is subdivided into two components: a knee score that rates only the knee joint itself and a functional score that rates the patient's ability to walk and climb stairs, with a higher score representing a better outcome for the knee or increased functionality, depending on the component. 25
Data Analysis
Descriptive statistics, including means and standard deviations for continuous variables and frequencies for categorical data, were calculated and displayed visually. Paired t-tests were performed comparing each follow-up to baseline.
Results
Demographics
Twelve patients were included in the case series. All 12 patients were diagnosed with symptomatic OA of the medial compartment of the knee. Patients age ranged from 35 to 61 years (ẋ = 48.76, SD = 8.15). Body mass index ranged from 22.2 to 44.6 (ẋ = 31.24, SD = 6.63), and seven of the participants had a BMI >30, categorizing them as “obese” (Table 2). Eight patients were male (66.7%), and four were female (33.3%). Eight patients (66.7%) had preexisting medical conditions, not otherwise specified, but were not deemed to interfere with the procedures of the study. The patients’ degree of OA, as measured by Kellgren–Lawrence grading, 27 ranging from 1 to 3, was assessed, and the majority of patients scored 3 (n = 9, 75%). Reporting of employment-related physical labor history varied largely between patients: two patients (16.7%) had a history of heavy physical labor, four patients (33.3%) with moderate physical labor, two patients (16.7%) with minimal physical labor, three patients (25.0%) with no history of physical labor, and one patient (8.3%) was unemployed. All the 12 patients were followed for five years. More detailed demographic information is listed in Table 2.
Demographic characteristics.

Outcome Scores
A summary of all outcome scores is available in Table 3, with ranges, means, and standard deviations.
Outcomes over time.

The mean baseline WOMAC pain score was 37.9 ± 13.4 (Fig. 2). The mean score significantly decreased at six weeks after the procedure, and this reduction was maintained through 60 months (P < 0.05). At the final follow-up, mean normalized WOMAC pain was 15.2 ± 15.2 (in the WOMAC scoring system, a lower score is desirable). Mean normalized WOMAC function scores demonstrated a similar pattern (Fig. 3). Decreased function was evident at baseline, with a mean score of 36.5 ± 16.5. WOMAC function scores significantly improved at all follow-up points, with a mean score of 10.9 ± 14.7 at the final follow-up (P < 0.05).

Normalized mean WOMAC pain score with standard error.

Normalized mean WOMAC function score with standard error.
The mean baseline KSS total score was 63.6 ± 12.2 (Fig. 4). KSS significantly improved from baseline over the entire course of the study, as the final mean KSS score at 60 months follow-up was 91.6 ± 12.9 (higher score indicates better result) (P < 0.05). Improvement from baseline after the KineSpring was also seen in the KSS function subscale (Fig. 5). At baseline, the mean KSS function score was 72.6 ± 22.0. These scores improved throughout the study to a mean of 98.4 ± 3.6 at the final follow-up point. Significant improvement from baseline in the KSS function score was seen at all time points (P < 0.05), except for the six-week follow-up (P = 0.105).

Mean KSS knee score with standard error.

Mean KSS function score with standard error.
Mean ROM scores over the course of the study is shown in Figure 6. ROM had a mean baseline score of 118.0 ± 13.6 and worsened immediately after surgery, indicating initial postoperative stiffness. However, scores improved at the six- and 12-month follow-up periods, with mean scores of 124.0 ± 11.5 and 127.1 ± 13.2, respectively. Significant improvement in knee ROM from baseline was seen at 12 and 48 months (P < 0.05).
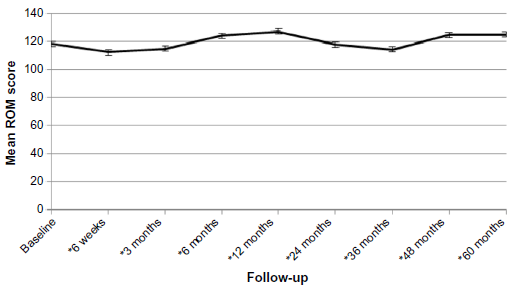
Mean ROM score with standard error.
Adverse Events
Six serious adverse events were reported within this study (Table 4). Three of these events occurred in the contralateral (nonstudy) leg, and one case of breast cancer was reported. Two of the events were related to treatment limb: one patient reported knee stiffness 1.5 years after surgery that ultimately resolved, and one patient had a deep infection that was resolved with antibiotics and no further sequelae.
Serious adverse events data.

Discussion
We report on a series of 12 patients who received the KineSpring System with five years of follow-up. It is the first study to report on the five-year outcomes of this device. The patients included in this series were relatively young, as compared to most individuals who undergo surgical treatment for knee OA. 13 More males than females were included in the study, and a wide variety of labor histories were reported. The Kellgren–Lawrence scores showed that the majority of patients had moderate OA. Symptoms of pain and poor functioning were evident at baseline. Improvement was seen as early as six weeks following surgery, and these improvements were maintained over the course of five years. ROM scores demonstrated initial postoperative stiffness, followed by improvements at six- and 12-month follow-up. Joint stiffness following TKA is relatively common,28,29 and the results of the current study demonstrate similar postoperative stiffness results. This type of initial stiffness is an expected occurrence in joint surgeries and is not necessarily indicative of lack of efficacy for this implant system.
When revision surgery is required, the KineSpring System has distinct advantages over other systems. First, it does not leave the same permanent damage to the joint, allowing for alternative methods to be pursued if desired by the patient or medically recommended. Furthermore, the KineSpring System can easily be reinstalled, with new replacement pieces. This was demonstrated clinically in the case of a 46-year-old male where a postoperative infection was given the opportunity to heal, and then the affected components of the device were reinstalled successfully. 30 Pain and functionality of the joint improved immediately following installation of the KineSpring System. Upon removal of the active components of the device, after the onset of infection, the symptoms of OA returned. After three months of infection treatment procedures, the KineSpring System was elected to be reinstalled, and again, the symptoms of OA were gone, even after an additional three months of reported follow-up. 30
Individual experimental cases have expanded into clinical trials, the midpoint results of which were very promising. The results of 99 patients from three clinical trials were positive, with follow-up times ranging from 1.5 to 48 months (mean 17 months). Pain, function, and stiffness measurements significantly improved from baseline to the last recorded follow-up point. 22 These trials also demonstrated significant cost-effectiveness when compared to standard surgical treatments and conservative methods. 31 The emergence of bicompartmental OA in the contralateral knee of one patient at three-year follow-up is a possible reason for that patient's higher WOMAC pain scores at 24 and 36 months. This potentially skewed this patient's results, as an adverse event not likely attributable to the implant may have caused worse pain scores at follow-up.
Our results, coupled with previous research supporting the KineSpring System's ability to preserve the knee joint 18 and reversible nature, 28 support the hypothesis that the implant system may fill an important gap in the treatment of moderate or early-onset knee OA.14–16 It has been previously shown that the KineSpring System can modify the progression of knee OA by increasing the joint space width and improving subchondral bone trabecular integrity. 23 Also, previous research has suggested that with a five-year lifespan of the implant, the KineSpring System demonstrates significant economic advantages over other surgeries and conservative methods. 31 Continued research should be conducted to corroborate the benefits of the KineSpring System in treating early knee OA, as well as the long-term benefits beyond five years.
Our study is strengthened by the use of previously validated instruments to assess knee pain and function,24,25 addressing a potential weakness of the case series design. 32 The current investigation has some limitations, which are commonly associated with case series. 32 First, the lack of a comparison group makes definitively concluding that the KineSpring System is advantageous over other treatments inappropriate. However, the extensive longitudinal design, with comparisons made to a baseline reference point, at the very least, provides a rationale justifying further investigation of the product as a standard treatment for knee OA. Second, the current study is limited by incomplete data collection, particularly in the measurement of ROM. Incomplete data and a small sample size only underline the need for continued investigation into the KineSpring System's treatment effect. Third, the current investigation may be at risk of selection bias, as patients chose to undergo the KineSpring treatment. The wide variety of labor histories and predominately severe ratings of OA suggest that the patients included in this series are an informative group. Fourth, only patients who were followed for five years were included, which may also contribute to a selection bias, as patients who did not feel sufficient efficacy from the treatment may have discontinued the study or undergone additional treatment.
Conclusion
The current case series demonstrated the longitudinal positive outcomes of the KineSpring System. Most notably, pain and functional problems associated with OA improved with treatment using the KineSpring System. Furthermore, these improvements were seen over the course of five years. The present study demonstrates promising results for the long-term efficacy of the KineSpring System implant for patients with moderate knee OA. Future investigations should be planned to include a larger sample size and, ideally, a longer follow-up period.
Author Contributions
Conceived and designed the study: CSL, MB. Analyzed the data: CSL, CV. Wrote the first draft of the manuscript: CSL. Contributed to the writing of the manuscript: CSL, CV, DAH, CSW, SS, MB. Agreed with manuscript results and conclusions: CSL, CV, SS, MB. Jointly developed the structure and arguments for the paper: CSL, CV, DAH, CSW, SS, MB. Made critical revisions and approved the final version: CSL, CV, DAH, CSW, SS, MB. All the authors reviewed and approved the final manuscript.