
Abstract
Surgical interventions for knee osteoarthritis (OA) have markedly different procedure attributes and may have dramatic differences in patient desirability. A total of 323 patients with knee OA were included in a dual response, choice-based conjoint analysis to identify the relative preference of 9 different procedure attributes. A model was also developed to simulate how patients might respond if presented with the real-world knee OA procedures, based on conservative assumptions regarding their attributes. The “amount of cutting and removal of the existing bone” required for a procedure had the highest preference score, indicating that these patients considered it the most important attribute. More specifically, a procedure that requires the least amount of bone cutting or removal would be expected to be the most preferred surgical alternative. The model also suggested that patients who are younger and report the highest pain levels and greatest functional limitations would be more likely to opt for surgical intervention.
Introduction
Globally, knee osteoarthritis (OA) is a leading cause of pain and disability in the adult population, having a considerable impact on both the health care system and a patient’s long-term quality of life.1–5 The spectrum of surgical options for knee OA is broad, offering a range of potential risks and benefits to patients. Across this spectrum, very little scientific study has considered the desires and preferences of patients, the persons undergoing the surgery. The ideal operative treatment would delay or prevent the progression of the disease, provide symptomatic relief, and preserve the anatomy and biomechanics of the joint.3,6–8 Surgical interventions for the treatment of knee OA include unicompartmental knee arthroplasty (UKA), high tibial osteotomy (HTO), total knee arthroplasty (TKA), and, recently in Europe, unicompartmental joint unloading with the KineSpring System (Moximed, Inc., Hayward, CA, USA).8–10 These procedures have markedly different perioperative and postoperative profiles and may, therefore, have dramatic differences in patient desirability.
Recently, the US Food and Drug Administration (FDA) has taken important steps to highlight the role of patients and their input in medical decision-making, including regulatory pathways to product approvals. Their goal is to bridge the gap between patients, their health care providers, and regulatory agencies.11–13 One approach to this is referred to as “patient-preference information,” which is defined as “qualitative or quantitative assessments of the relative desirability or acceptability to patients of specified alternatives or choices among outcomes or other attributes that differ among alternative health interventions.” 11 The submission of patient-preference information to the FDA is not mandatory, but it might be useful for the following: (1) devices intended to yield significant health and appearance benefits, (2) devices intended to directly affect health-related quality of life, (3) devices that are life-saving, but high-risk, (4) devices developed to fill an unmet medical need or treat a rare disease/condition, (5) devices that offer alternative benefits to those already marketed, or (6) devices with novel technology. 11
Patient perspectives regarding the benefit-risk trade-offs of therapies and their defining attributes are valuable because only patients live with their conditions and the consequences of their choices.11,13 Such information is useful when multiple treatment options exist for a given condition, when comparative effects between treatments are uncertain, or when patients’ views about benefits and risks vary within the patient population or differ from those of their health care providers. 11 It would also be influential in the research and development of future therapies.11,13
The purpose of this study was to obtain patient-preference evidence to inform regulatory approval decisions by the FDA Center for Devices and Radiological Health during the benefit-risk assessment of surgical interventions for knee OA. This approach will provide quantitative estimates on the value of the individual attributes defining these procedures, from the patient’s perspective, allowing for a comparison between surgical treatments based on each of their unique characteristics.
Methods
Design
One quantitative method recommended by FDA for conducting a patient-preference study is conjoint analysis, which is a stated preference research tool that involves asking patients a series of questions and analyzing their response patterns to determine the underlying value of an intervention’s attributes and potential outcomes.12,14,15
A dual response, choice-based conjoint approach was used, 14 asking respondents to select their most preferred treatment alternative from a set of 3 hypothetical surgical options for knee OA. This is a type of “stated-preference” study, as opposed to a “revealed-preference” test, where patient preferences are elicited by offering study participants choices or asking them to answer valuation questions in the form of an experimental design. Revealed-preference methods obtain patient preferences from the actual observed choices made by patients, which can avoid the hypothetical bias associated with stated-preference models. However, such methods are difficult to apply when a device profile of interest is not yet available for patients to choose from because the device is still under regulatory review. Therefore, revealed-preference methods are limited when the benefit-risk profile of a device is not comparable with any other on the market. These methods are also subject to potential biases, such as financial considerations of individual patients. 11 The KineSpring System is not yet approved by the US FDA, and data regarding actual patient choices involving this device do not exist; therefore, a stated-preference approach was deemed more suitable for this study.
An analysis of the pattern of their choices revealed the implicit relative importance of the procedure attributes. Based on these results, the perceived value of an intervention was estimated as a weighted sum of the attributes, where the weights represented the average relative importance of each feature. For the purposes of this study, these weights are referred to as “preference scores.” 13 The resulting preference scores are displayed on the same scale to allow for direct comparisons between the procedure attributes. 11
Setting and participants
An email invitation to the survey was sent in June 2016 to a group of Internet panelists in the United States. They were recruited from Research Now, an online sampling and data collection company that provides a nationally representative panel of consumers. These panelists receive “panel points,” which accumulate as they complete surveys and can be exchanged for gifts. The message did not specify the topic of the research, why they were sent the invitation letter, or who developed the survey. The panelists were simply told that the survey was about health care products and treatments for ailments. Respondents had to complete a set of screening questions to ensure that they met the following criteria, which was selected to ensure a study sample representative of US patients with knee OA who may realistically be offered surgery to treat their condition16,17:
Men and women aged 25 to 80 years;
Diagnosed with OA in the knee;
Experience pain in the knee of ⩾4 on a 0 to 10 scale, where 0 means not at all painful and 10 means extremely painful;
Experience knee pain at least once a week;
Previously failed nonsurgical treatments for knee OA pain;
Pass a security screen;
No previous surgical implant involving the knee (ie, TKA, UKA).
Only qualified respondents proceeded to the online survey. The link to the Web site included an embedded password that could only be used once. Respondents did not have the ability to go back to previous questions. We targeted a minimum sample of 300 patients based on the recommendation from Bridges et al 14 on Good Research Practices for Conjoint Analysis Task Force. All patients who completed the survey were included in the analysis.
This study received exemption from the Western Institutional Review Board prior to conduct and is registered on clinicaltrials.gov (NCT02934672).
Survey instrument
The first section of the questionnaire captured demographic details on the patient (Supplement 1). The second section presented a series of trade-off exercises, during which a patient was presented with 3 hypothetical surgical alternatives, each described by 9 distinct treatment attributes. Each attribute was constructed of 2, 3, or 4 levels (see Table 1 for a complete listing of the procedure attributes and their corresponding levels, which was developed and finalized in collaboration with an orthopedic surgeon). Although some of the attribute levels displayed in this table may very rarely been seen in actual clinical practice, they were intentionally presented as maximum levels to patients to establish a relative scale across the range of levels (eg, complete pain relief, zero chance of additional future surgery).
Procedure attributes for knee osteoarthritis.

“Minor pain” defined as a score of ⩽3 on a 0 to 10 scale.
In the trade-off exercise, the level for each of the attributes of a given procedure was randomly generated, reducing the likelihood that the hypothetical alternatives would match existing, real-world procedures. The 3 surgical alternatives were presented as “Treatment A,” “Treatment B,” and “Treatment C” in the survey (Figure 1), and the names of real treatments were never presented to survey respondents. Respondents completed the choice exercise 12 times, representing a balance between guidelines for a robust survey and survey fatigue. 13 When presented with the 3 hypothetical surgical options, respondents were instructed to assume that all of the treatments were considered clinically acceptable by their doctor. Patients then chose which 1 of the 3 alternatives they would be most likely to have and which one they would be least likely to have (Figure 1). Subsequently, respondents were then asked, with reference to their selected preferred treatment in the trade-off exercise, “How likely would you be to actually have that treatment?” with the following possible answers: (1) definitely would, (2) probably would, (3) might or might not, (4) probably would not, and (5) definitely would not (Figure 2).

Trade-off exercise step 1, “For the 3 treatments below, which one would you be most likely to have and which one would you be least likely to have?”

Trade-off exercise step 2, “This is the treatment you preferred. How likely would you be to actually have that treatment?”
The final survey instrument was piloted in a group of naïve respondents prior to study conduct. This was done to ensure that the questions were clear and comprehensible, and that the online survey was functioning as desired. The group of naïve respondents did not find the tasks unreasonable to complete. The survey was then launched to a preliminary sample of the target audience, and their responses were monitored for any issues. There was no indication that this preliminary sample found the survey to be too difficult or cumbersome, as there was no evidence of them simply stopping in the middle of the survey, patterned responses, or respondents speeding through the survey (based on the mean length of time to complete the survey and the normal distribution around this mean).
Data analysis
Patient preference scores for the procedure attributes were calculated based on the response patterns of the included sample. A hierarchical Bayesian multinomial logit model was used to generate utilities that accounted for individual preferences. These utilities were then used to run simulations and calculate preference scores with the choice-based conjoint analysis software by Sawtooth Software, Inc. (Orem, UT, USA).18–22 The ensuing model predicted how patients might respond if they were presented with the real-world surgical options for knee OA using conservative baseline assumptions for their attribute levels (Table 2). These assumptions were based on outcomes reported in the previous literature.23–33 The model predicted the probability that a patient would choose a given treatment relative to the other treatments, or a no-procedure alternative, included in the model. It was also able to simulate responses by sex, age group, patients’ pain level, and the impact of their knee problems on their daily function.
Procedure profiles for knee osteoarthritis.

Abbreviations: HTO, high tibial osteotomy; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
“Minor pain” defined as a score of ⩽3 on a 0 to 10 scale.
The model was also programmed to simulate how patients with knee OA might respond if they were presented with up to 3 treatment options. We compared the KineSpring System attributes to those of each of the other 3 real-world surgical procedures (ie, HTO, UKA, and TKA) and also simulated how patients might respond if they were given the option to choose between 3 of these interventions. We also performed a sensitivity analysis to determine whether, and to what extent, patient responses might change if presented with the “worst-case” scenario for the KineSpring System when compared with less conservative assumptions for both arthroplasty procedures (ie, UKA and TKA). In this simulation, alternate assumptions were used for the attribute levels of “maintains natural knee motion,” “amount of pain relief,” and “postrecovery activity restrictions” for both UKA and TKA; we retained the conservative assumptions of the KineSpring System as presented in Table 2.
Results
Data quality and demographics
We screened 978 Internet panelists. In all, 583 did not qualify for the following reasons: did not have knee OA, accessed the survey via a mobile device, did not have the minimum level or frequency of pain required, did not pass questions B or E of the security screening questions (Supplement 1), had previously undergone knee replacement surgery, or were younger than 25 years old. Of the remaining 395, 72 did not complete the survey; therefore, 323 were included in the final analysis (a completion rate of 81.8%).
The demographic characteristics of the 323 respondents are available in Table 3. More than 65% of the sample was women, 47% were less than 60 years old, and 94% were white. Approximately 97% of respondents had some form of medical insurance. Almost 54% of patients stated that they have knee pain every day, and 21% of them rated their pain as high (defined as ⩾8 on a 1-10 scale). Roughly 71% indicated the presence of pain in both knees, and 57% experienced symptoms for greater than 5 years. Of the 299 respondents who spoke with a doctor about their knee pain, 79% consulted with their primary care physician and 59% saw an orthopedic surgeon. The most common previously attempted treatments for symptomatic relief were simple pain medications (69%), physical therapy (55%), knee bracing (48%), weight loss (46%), and nonsteroidal anti-inflammatory drugs (44%).
Demographic characteristics of the 323 survey respondents.

Abbreviation: NSAIDs, nonsteroidal anti-inflammatory drugs.
Respondents could select more than 1 option.
Preference score estimates
Figure 3 shows the preference score estimates for all attributes on the same 100% scale (individual scores add up to 100%). These scores represent quantitative estimates of how much respondents weighed (or valued) a given procedure attribute, relative to all other attributes, based on the choices they made in the trade-off exercise. The mean preference score value was 11.1%. The “amount of cutting and removal of the existing bone required” for the procedure had the highest preference score of 18.7% (ie, it was the most important of the 9 procedure attributes to patients), followed by the “chance of additional surgery” (14.1%) and “amount of pain relief” (12.7%); the attributes with the lowest preference scores (least important to patients) were “limits or complicates any future treatment needs on the knee” (7.3%) and “length of hospital stay required” (7.3%). Estimates by sex, age, baseline level of pain, and level of impact on daily function showed similar results (Supplement 2).

Preference score estimates for attributes of knee osteoarthritis surgical procedures (100% scale). Attributes are sorted from highest to lowest relative importance.
Table 4 shows the preference scores of the levels within each procedure attribute. This scale ranges from −100 to +100, where the numerical estimate of the score is a measure of how much respondents valued a particular attribute level and the direction is an indication of whether it was more (positive score) or less (negative score) preferable to patients. It was determined that a procedure that does not require any bone cutting or removal was the most preferred attribute level (preference score: +72.5), whereas one that requires the cutting of 2 leg bones with extensive bone removal was the least preferred attribute level (preference score: −56.3).
Estimates of preference scores for all levels within individual attributes (−100 to +100 scale).
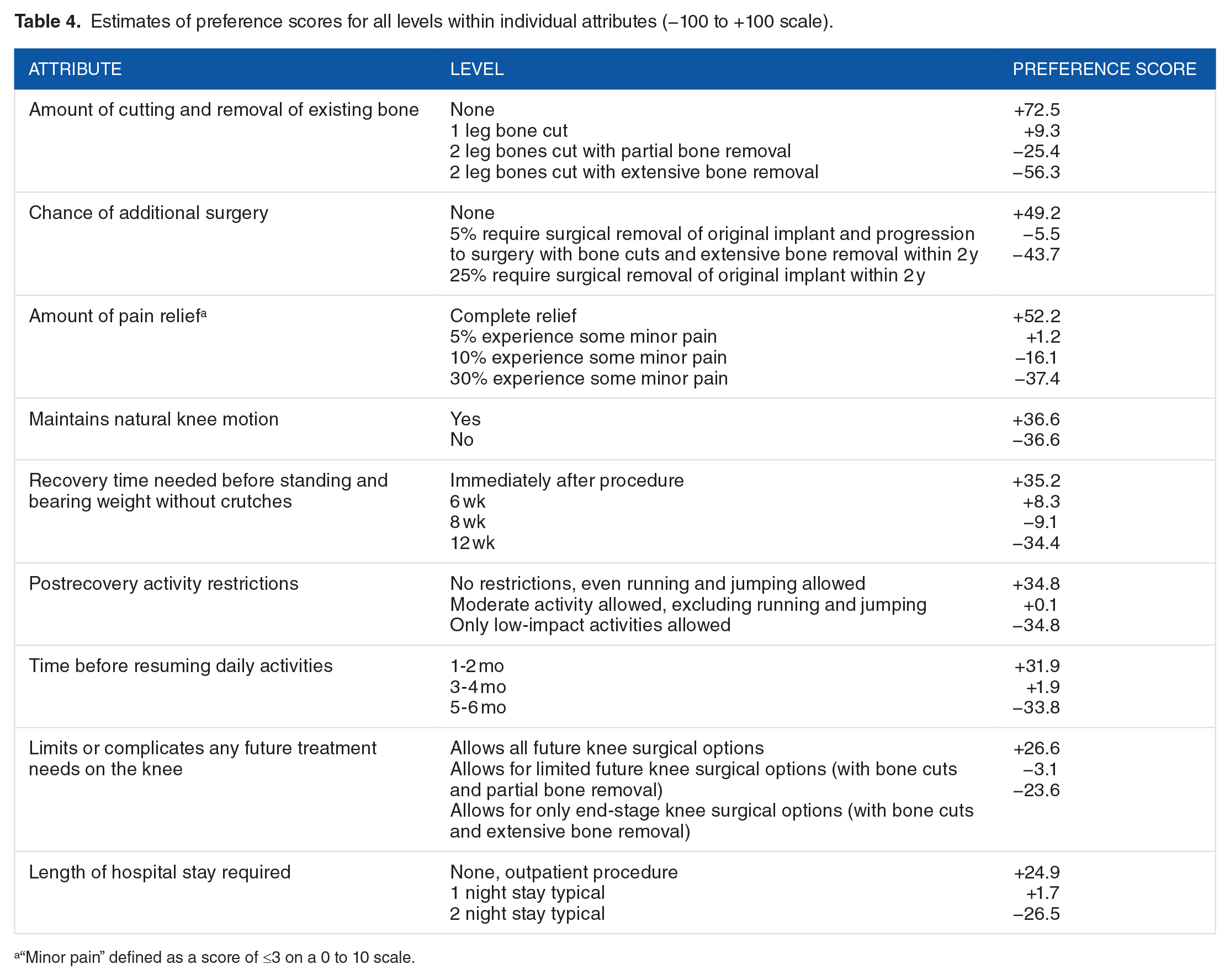
“Minor pain” defined as a score of ⩽3 on a 0 to 10 scale.
Table 5 presents the estimated percentage of respondents who would choose a surgical option over a no-procedure alternative, for each of the 4 real-world knee OA surgical interventions. These estimates were based on the procedure profiles in Table 2. The predicted proportions of respondents who would prefer the surgery over no surgery were 32.5% for the KineSpring System, 7.1% for UKA, 5.9% for HTO, and 5.3% for TKA. This trend was consistent across sexes, age groups, pain levels, and impact levels on daily function. The results in Table 5 also demonstrated limited differences in the predicted responses between men and women; however, they also revealed that younger patients, those with a greater pain level, and those with higher restrictions on daily function would be most likely to opt for surgery. This observation was consistent across all procedures.
Simulated responses for preference of a surgical option over a no-procedure alternative (% of respondents).
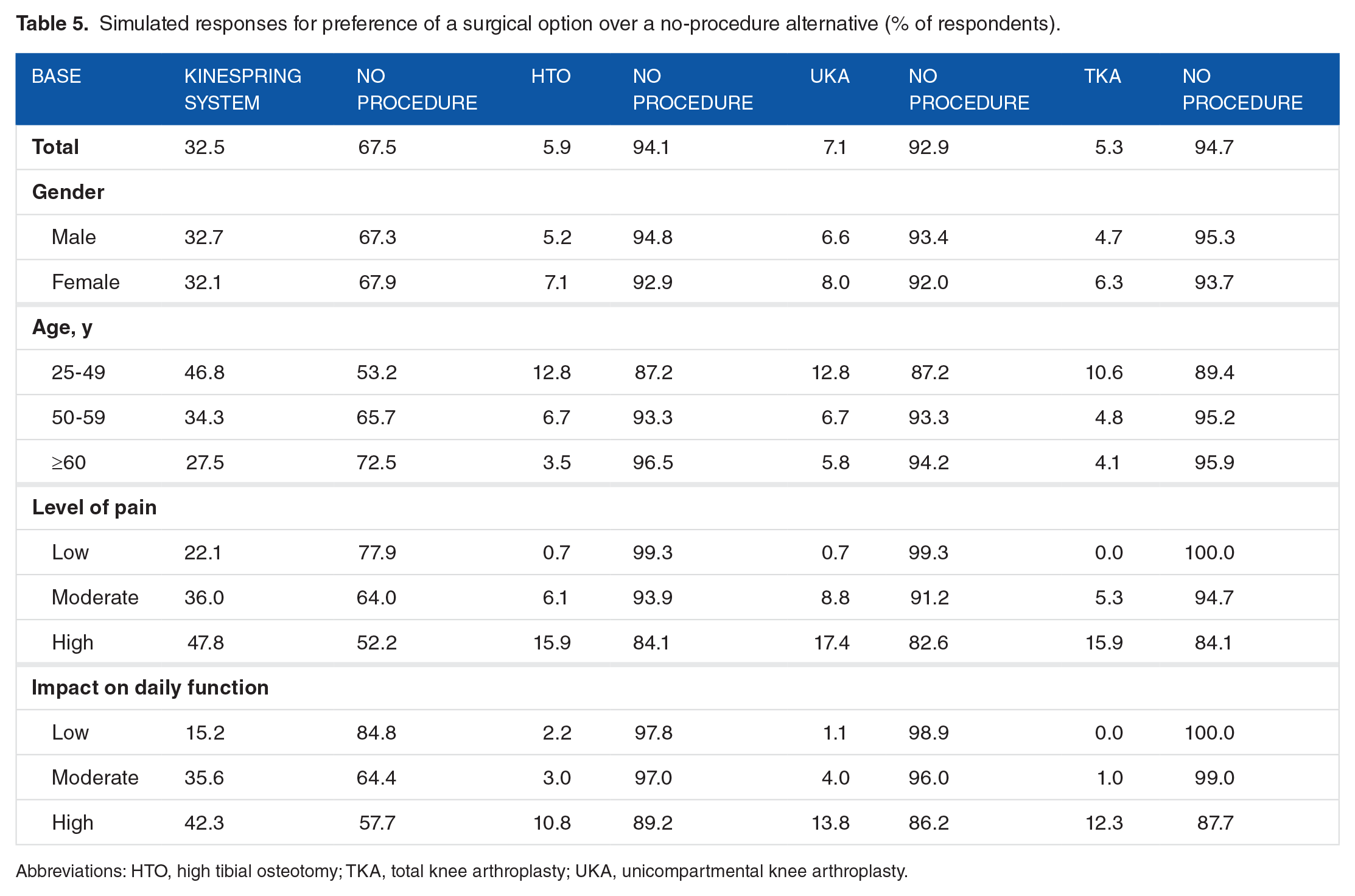
Abbreviations: HTO, high tibial osteotomy; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
In the models that simulated patient responses if they were offered the KineSpring System versus the other surgical options, the results consistently demonstrated a greater preference for a treatment with the attributes of the KineSpring System (Supplement 3). The results of the sensitivity analysis are shown in Table 6, which, again, demonstrated a greater expected preference for a treatment with characteristics similar to those of the KineSpring System.
Sensitivity analysis.

Abbreviations: TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty.
“Minor pain” defined as a score of ⩽3 on a 0 to 10 scale.
Alternate assumption used in sensitivity analysis.
Discussion
The model, which was developed based on stated preferences of patients with actual knee OA, concluded that the surgical feature that contributed the most to a patient’s decision (ie, the attribute with the highest patient preference score) was the “amount of cutting and removal of the existing bone required” for the procedure. The results also suggested that patients would be more likely to select a procedure with the attributes of the KineSpring System if they were younger, had a greater level of pain, or if their knee problems had a greater impact on their daily function. Importantly, men and women would be equally as likely to have a procedure with such characteristics. These findings are consistent with previous publications that have emphasized the desire to offer patients a procedure that preserves the bone for future surgeries, while also relieving symptoms and improving function, among younger and more active individuals.34,35 Bozic et al 34 evaluated patient preferences in a sample of individuals with hip OA and found that the most important factor in the group of patients who chose hip resurfacing arthroplasty was the procedure’s impact on femoral bone preservation. This study provides quantitative evidence that this particular treatment attribute is also important to patients with knee OA.
Similar studies have been previously conducted, but they focused on nonsurgical therapies for knee OA and considered different attributes.19,21,36 This sample was drawn from a cross section of the US knee OA population who may realistically be offered surgery for their condition.16,17 Survey respondents were predominantly white (93.5%) and patients with medical insurance (96.9%). There were also nearly twice as many women as men (65.3% versus 34.7%) included in the study. The treatment attributes included in this study were patient-centered and clinically important.
Several recent studies have highlighted higher complication rates and an increased likelihood of revision surgery of up to 9% at 2 years in younger patients with TKA.28,35,37 A recent report also suggested that approximately one-third of younger patients receiving TKA have residual pain and symptoms. 31 There are also concerns about a patient’s ability to function after TKA, as only low-impact activities are recommended postsurgery, and activities such as jogging, racquetball, and skiing should be avoided.24,35 Thus, it would not be surprising if potential knee surgery patients might prefer a treatment with distinctly different attributes than an arthroplasty procedure.
This study had some limitations. The sample was predominantly white (93.5%), and previous literature demonstrates that decisions regarding willingness to undergo surgery may differ between races.38–41 Vina et al 41 found that the decline in the willingness to operate, relative to baseline, was less in those who consulted with an orthopedic surgeon. In this study, just 58.9% of the sample spoke with an orthopedic surgeon about their knee, and our analysis does not reveal how this may have influenced patient responses. Although most of the participants (96.9%) had some form of medical insurance, we did not factor in any items related to the cost of these procedures and it is unclear how important price differences between these treatments would be among this population. The survey was Internet based, which can create a bias against computer-illiterate participants 21 and may exclude a subset of relevant patients from the study. There was an unequal distribution of men and women in the sample, but this potential bias is mitigated because the responses of both sexes resulted in similar preferences in surgical treatment characteristics and in overall treatment preference (Supplements 2 and 3). Also, hypothetical choices among different devices do not have the same clinical and emotional consequences as actual choices.11,13 To reduce the potential for this hypothetical bias, we first obtained judgments from patients about which combination of possible attributes was more preferable, which were then used to elicit stated choices between procedure and no-procedure alternatives. Another limitation is that the results of such a study are dependent on the type of questions included in the survey, which may introduce a form of response bias; however, in this study, the questions were selected based on the input and review of a practicing orthopedic surgeon, although the lack of patient involvement may be considered another weakness of this study. Using a survey design meant that respondents had to self-report that they were diagnosed with knee OA, although there is evidence that suggests that self-reporting is comparable with what is reported in patient medical records. 21 Finally, this type of experiment only reveals how respondents weigh the importance of a given characteristic relative to the other characteristics included in the survey instrument; therefore, these results can only be generalized to the attributes and levels that were included in this study. 19 In terms of study strengths, we surveyed a large sample of patients with the condition of interest. We also included individuals across a wide age range to help ensure that we captured the responses of patients with knee OA of all age groups and allow us to compare results between these age groups. Finally, we required that respondents met minimum levels and frequencies of knee pain, increasing the likelihood that the patient would realistically consider a surgical procedure.
As the condition is progressive, patients with knee OA are aware that arthroplasty is an inevitable long-term outcome35,39,41,42; therefore, as the severity of their symptoms worsens, they may alter their opinions of or reassess the benefits and risks of undergoing surgery. Another important consideration when evaluating patients for treatment is that the level of pain does not always correlate with the structural severity of OA. In other words, patients with early structural changes can have symptoms just as bad as those with end-stage OA and may elect to undergo arthroplasty for symptomatic relief. 43 This highlights the importance of discovering novel technologies that result in more optimal outcomes for this subset of patients with knee OA.
Conclusions
Stated patient preferences suggested that patients with knee OA, particularly younger patients with higher levels of pain and functional restrictions, would prefer a surgery that does not require bone cutting or removal. Not surprisingly, a model incorporating patient-preference data predicted a greater desirability for a treatment option (KineSpring System) that does not require bone cutting or removal.
Footnotes
Peer review:
Two peer reviewers contributed to the peer review report. Reviewers’ reports totaled 408 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Moximed, Inc.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Claude T Moorman III was a clinical investigator in the SOAR clinical study of the KineSpring System; his institution received research support to conduct the SOAR study, but Dr Moorman has no financial interests in Moximed. Tom Kirwan, Jennifer Share, and Christopher Vannabouathong have no interest, financial or otherwise, in the results of the study.
Author Contributions
CTM, TK, and JS conceived and designed the experiments. TK and JS analyzed the data. CV wrote the first draft of the manuscript. CTM, TK, JS, and CV contributed to the writing of the manuscript, agree with manuscript results and conclusions, jointly developed the structure and arguments for the paper, made critical revisions and approved final version, reviewed, and approved the final manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.