
Abstract
In young patients with medial knee osteoarthritis (OA), surgical intervention may not be desirable due to preferences to avoid bone cutting procedures, return to high activity levels, and prolong implant survival. The Atlas Knee System was designed to fill the gap between ineffective conservative treatments and invasive surgery. This single-arm study included 26 patients, aged 25 to 65 years, who completed 12 months of follow-up. All dimensions of the Knee injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Knee Society Score significantly improved from baseline to 12 months. About 96.2% and 92.3% of patients experienced a ⩾20% improvement in their KOOS pain and WOMAC pain scores, respectively, at 12 months. This study highlights the potential benefit of a joint unloading device in the management of young patients with medial knee OA. The trial is still ongoing and another analysis is planned at 24 months.
Background
Osteoarthritis (OA) of the knee is a leading cause of disability in the adult population globally. In the United States, 1 in 4 adults (54 million) have arthritis, and more than half of them are younger than 65 years old. Patients aged 35 to 65 years represent the fastest growing segment of the OA population.1–7 Many of these younger patients have unicompartmental knee OA, which most frequently occurs in the medial compartment, as it takes on significantly more load during weight bearing than the lateral compartment.8–11
Treatment for medial compartment knee OA typically begins with nonsurgical therapies, such as weight loss, orthotics, analgesics, anti-inflammatory drugs, and joint injections, although they may eventually fail as they do not correct the underlying pathology.2,4 Patients may then progress to surgical intervention, namely, arthroplasty or high tibial osteotomy (HTO). In younger patients, this decision may be influenced by their desire to avoid procedures that require bone cutting or bone removal and restrict their return to high activity levels.2–4,11
Just as the number of younger arthritics is increasing rapidly, the incidence of arthroplasty procedures is increasing disproportionately quickly in this younger patient population with knee OA. Unicompartmental knee arthroplasty (UKA) is an option and, if it fails, total knee arthroplasty (TKA) is typically the next step. Total knee arthroplasty following a primary UKA can be more technically demanding if bone grafts, wedges, or stems are required, and any revision arthroplasty carries an increased risk of a complication.12–17 Younger patients are more likely to experience failure of the prosthesis and, subsequently, require a revision surgery.4,9,13,18–21 In a study of 88 000 patients in California, Meehan et al 22 found that patients with TKA < 50 years old experienced a 2-year revision rate of 9% due to infection and aseptic loosening, a rate nearly 4 times that of patients >65 years old. Furthermore, multiple recent studies have reported dissatisfaction rates near 30% in arthroplasty patients <55 years old, with the authors recommending that patients younger than 55 years be informed about the increased risk of dissatisfaction.20,23 Meanwhile, HTO, despite some clinical success, has been less popular with patients and surgeons in certain cultures because it involves invasive bone alterations, a potentially prolonged recovery, and may actually accelerate OA in the lateral compartment as a result of the load shifting to this compartment.3,8,9 With higher revision and dissatisfaction rates after arthroplasty and an aversion to HTO, there is a clear clinical need to be addressed for the younger patient with knee OA.
Unicompartmental load-absorbing implants were developed to fill the gap between ineffective conservative treatments and invasive surgical options.4,9,10 Once such device is the Atlas System (Moximed, Inc, Hayward, CA, USA), a second-generation load absorber whose implantation is minimally invasive, extra-articular, and does not require bone resection. 3 The implant unloads the diseased medial compartment of the knee by means of an absorbing element, which is compressed during weight bearing, without transferring the excess load to the unaffected lateral compartment and maintaining the natural kinematics of the joint. Early research on the implant is promising, demonstrating excellent safety, effectiveness, and durability outcomes, and successful implantation rates.3,9,10,24–27
The Atlas System was first evaluated in a single-arm, multicenter study. The purpose of this study (the PHANTOM High Flex Trial) was to assess the clinical efficacy and safety of the Atlas System after 24 months of follow-up in patients needing unloading of the medial compartment of the knee. The trial is still ongoing and the current report is an interim analysis after all patients returned for their 12-month follow-up visit.
Methods
Objectives
The primary objectives of this study are to evaluate changes in pain and function at 24 months compared with baseline, using patients as their own controls, and safety outcomes. Safety will be determined using the incidence of treatment-emergent adverse events (AEs). Secondary objectives are procedural success, both patient-reported and physician-reported changes in outcomes scores, and radiographic assessments of the knee and implant.
Design
The study was designed, conducted, recorded, and reported in compliance with the principles of Good Clinical Practice guidelines and the International Organization for Standardization (ISO) 14155, 28 as well as in accordance with all national, state, and local laws of the appropriate regulatory authorities and the Declaration of Helsinki. The trial was registered with clinicaltrials.gov (NCT02711254).
The study is being conducted across 3 sites in Poland and 1 site in South Africa. Patient enrollment was completed between August and September 2015, and final 24-month data collection is expected to be completed by October 2017. All eligible patients who received the implant will be followed for 24 months following the procedure, with study visits at baseline, immediately postprocedure, 6 weeks, and 3, 6, 12, and 24 months.
Eligibility criteria
Eligible patients were men or women, between the ages of 25 and 65 years, and had a documented pathology of the medial compartment of the knee that required unloading. The pathology qualified with either an International Cartilage Repair Society (ICRS) score >0 as assessed by magnetic resonance imaging or arthroscopy older than 3 months or a Kellgren-Lawrence (KL) grade ⩽3 as assessed by X-ray. They also had continued target knee pain despite 6 months of conservative treatment prior to surgery, pain in the target knee as demonstrated by a minimum score of 40 (scale 0-100) on the Knee injury and Osteoarthritis Outcome Score (KOOS) pain domain questions, knee flexion ⩾90° to ⩽140°, a body mass index (BMI) between 24 and 35 kg/m2, and weight ⩽110 kg. Patients with an active infection, sepsis, osteomyelitis or history of septic arthritis in any joint, rheumatoid arthritis or other forms of inflammatory joint disease, significant OA in the lateral compartment of the study knee (defined as a KL grade ⩾2), significant OA in the patellofemoral compartment of the study knee (defined as a KL grade ⩾3), radiographic evidence of OA (KL grade >2) in the contralateral knee and clinical findings of OA symptoms that interfered with activities of daily living (ADL) or required the use of an assist device, previous joint modifying surgery in the target knee within 12 months prior to the planned surgery date, disorders which may impair bone formation, another significant medical condition or other factor that the investigator felt would have interfered with study participation, taking concomitant immunosuppressive therapy, or who smoked or quit smoking less than 1 year prior to enrollment were excluded. A more detailed description of the inclusion and exclusion criteria is available in the supplementary data.
Device description
The Atlas System (Figure 1) consists of titanium alloy femoral and tibial bases and a polycarbonate urethane absorber that reduces the load transferred through the affected medial compartment of the knee joint. The absorber is made of a central body that provides compressive load absorption and an articulating ball and socket joint at each end that allows the device to accommodate the natural motions of the knee (Figure 2). The absorber is implanted in the subcutaneous tissue of the medial extracapsular space and remains extra-articular. The compressible load absorber spans the joint, is positioned superficial to the medial collateral ligament, and isolated from the articular surfaces of the knee. The device is designed to be implanted through a single, relatively small incision without resection of bone, muscle, or ligaments, and without violation of the joint capsule. The device can be removed without disruption to the joint and surrounding tissues, and primary joint replacement surgery can be performed in the future, if necessary.
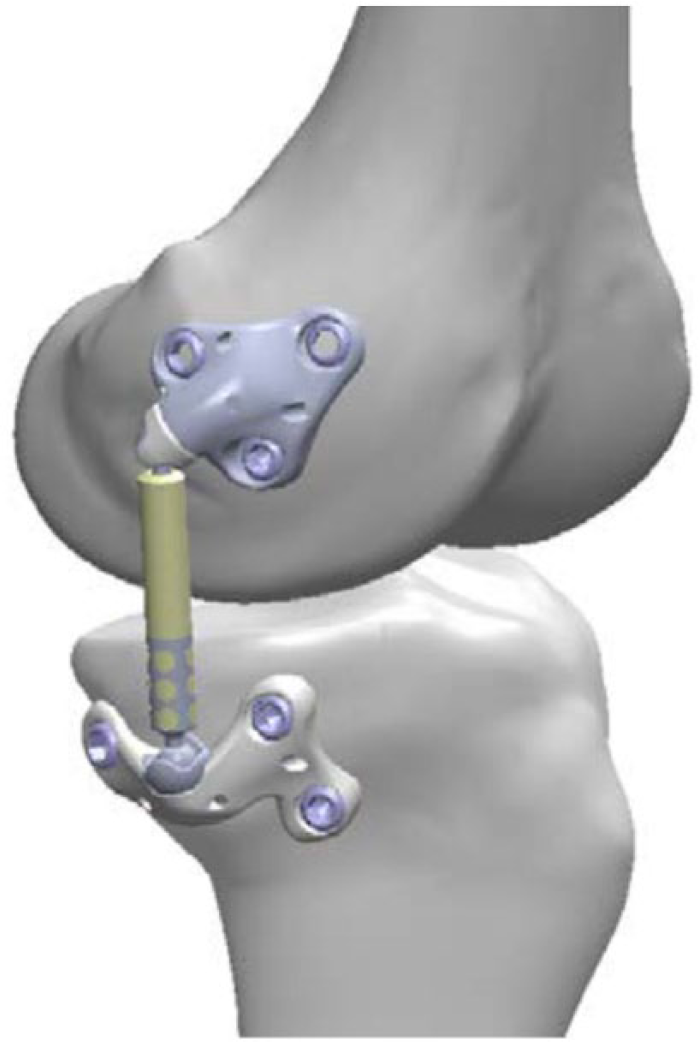
ATLAS Knee System.

ATLAS Knee System components.
The implant allows the surfaces of the joint to continue to articulate and bear weight postimplantation. By providing a supplemental load path to the side of the affected portion of the joint, the Atlas System reduces the amount of load carried by the degenerated surfaces. It provides up to 13 kg of knee unloading, without compromising range of motion (ROM).
On the day of surgery, standard preoperative preparations are taken for the patient, similar to those used in mini-open ligament repair procedures. The patient is sedated under general or spinal anesthesia. The device is implanted using direct visualization. Surgical implantation is completed using standard operative orthopedic tools and techniques in conjunction with instruments unique to the Atlas System. No concomitant procedures, including arthroscopy, were permitted in this study.
Outcomes
The KOOS is a disease-specific measure comprising 5 dimensions: pain, other symptoms, function in ADL, function in sport and recreation, and knee-related quality of life (QoL). 29 The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), also a disease-specific measure, was calculated based on 24 questions within the KOOS questionnaires and is used to evaluate the areas of pain, stiffness, and physical function. 30 The Knee Society Score (KSS) is a clinical evaluation system for reporting results for patients undergoing knee implant surgery. 31 The KSS consists of 2 parts, the Knee Score, which assesses pain, ROM, and stability, and the Function Score, which evaluates a patient’s ability to walk on level surfaces, ascend and descend stairs, and the use of external supporting devices.
All operative and postoperative complications, whether device-related or not, were recorded and reported.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 20.0, IBM Corp., Armonk, NY, USA). Categorical variables were presented as counts and proportions. Continuous data were presented as means with their standard errors. Clinical outcome scores were compared using a 1-way repeated-measures analysis of variance and displayed as both absolute and change from baseline scores. A P value less than .05 was considered statistically significant.
Adverse events were summarized and categorized by severity and relation to the study procedures. An AE that was considered recurrent was updated at the subsequent visit. Such cases were counted as one event and the highest severity was assigned. Serious adverse events (SAEs) and AEs leading to discontinuation of the study were also recorded.
Study safety success was defined as an absence of unanticipated serious adverse device effects. We also determined the proportion of patients who experienced a clinically meaningful ⩾20% improvement in their KOOS pain and WOMAC pain scores at 12 months.32–34
Results
Demographics
Twenty-six patients were enrolled and treated in the study. Baseline characteristics are shown in Table 1. The mean age of the patients at the time of surgery was 51 ± 1.7 years. The study cohort included 16 men (61.5%) and 10 women (38.5%). Their average weight and BMI were 84.7 ± 1.8 kg and 28.4 ± 0.6 kg/m2, respectively. Twenty-three patients (88.5%) were employed or self-employed at the time of enrollment. The procedure was completed in the right knee for 14 (53.8%) patients, and the average operation time was 56.8 ± 2.8 minutes. Half of the patients had prior surgery in the study knee. All devices were successfully implanted, and no concomitant procedures, including arthroscopy, were performed.
Baseline characteristics (n = 26).

Clinical outcomes
Average KOOS pain scores significantly improved from 44.2 ± 2.1 at baseline to 78.9 ± 3.7 points at 12 months (Table 2; Figure 3). Bonferroni-adjusted pairwise comparisons demonstrated statistically significant changes at each study visit relative to baseline. At 12 months, 25 (96.2%) patients experienced a clinically meaningful ⩾20% improvement in their KOOS pain score. Knee injury and Osteoarthritis Outcome Score symptoms, ADL, sports and recreation, and QoL scores also all significantly improved over 12 months (Table 2; Figure 3). For each of these dimensions, Bonferroni-adjusted pairwise comparisons demonstrated statistically significant improvements at each study visit relative to baseline, except for the KOOS symptoms and KOOS sports and recreation scores at 6 weeks.
Results of 1-way repeated-measures ANOVA (n = 26).

Abbreviations: ADL, activities of daily living; ANOVA, analysis of variance; KOOS, Knee injury and Osteoarthritis Outcome Score; KSS, Knee Society Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Values are expressed as mean ± SE. Values in bold are statistically significant compared with baseline, according to Bonferroni-adjusted pairwise comparison.
Higher score indicates improvement.
Lower score indicates improvement.
n = 25, 1 patient missing data point at 12 months.

Mean KOOS scores from baseline to 12 months. ADL indicates activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, quality of life.
Western Ontario and McMaster Universities Osteoarthritis Index pain, stiffness, and function subscales all significantly improved over 12 months (Table 2; Figure 4). For both pain and function, Bonferroni-adjusted pairwise comparisons demonstrated statistically significant improvements at each study visit relative to baseline. Pain scores improved from 53.5 ± 1.7 at baseline to 16.3 ± 3.5 at 12 months, and function scores improved from 48.4 ± 3.4 at baseline to 18.2 ± 3.7 at 12 months. At 12 months, 24 of 26 (92.3%) had a clinically meaningful ⩾20% improvement in their WOMAC pain score. The average change in the WOMAC stiffness score from baseline was significant at 6 and 12 months only.

Mean WOMAC scores from baseline to 12 months. WOMAC indicates Western Ontario and McMaster Universities Osteoarthritis Index.
Average scores for both KSS knee and KSS function significantly improved over 12 months (Table 2; Figure 5). The KSS knee scores improved from 61.9 ± 3.0 at baseline to 94.6 ± 1.6 at 12 months, and KSS function scores improved from 73.4 ± 2.8 at baseline to 98.1 ± 1.1 at 12 months. Bonferroni-adjusted pairwise comparisons demonstrated statistically significant improvements at each study visit relative to baseline except for KSS function at 6 weeks.
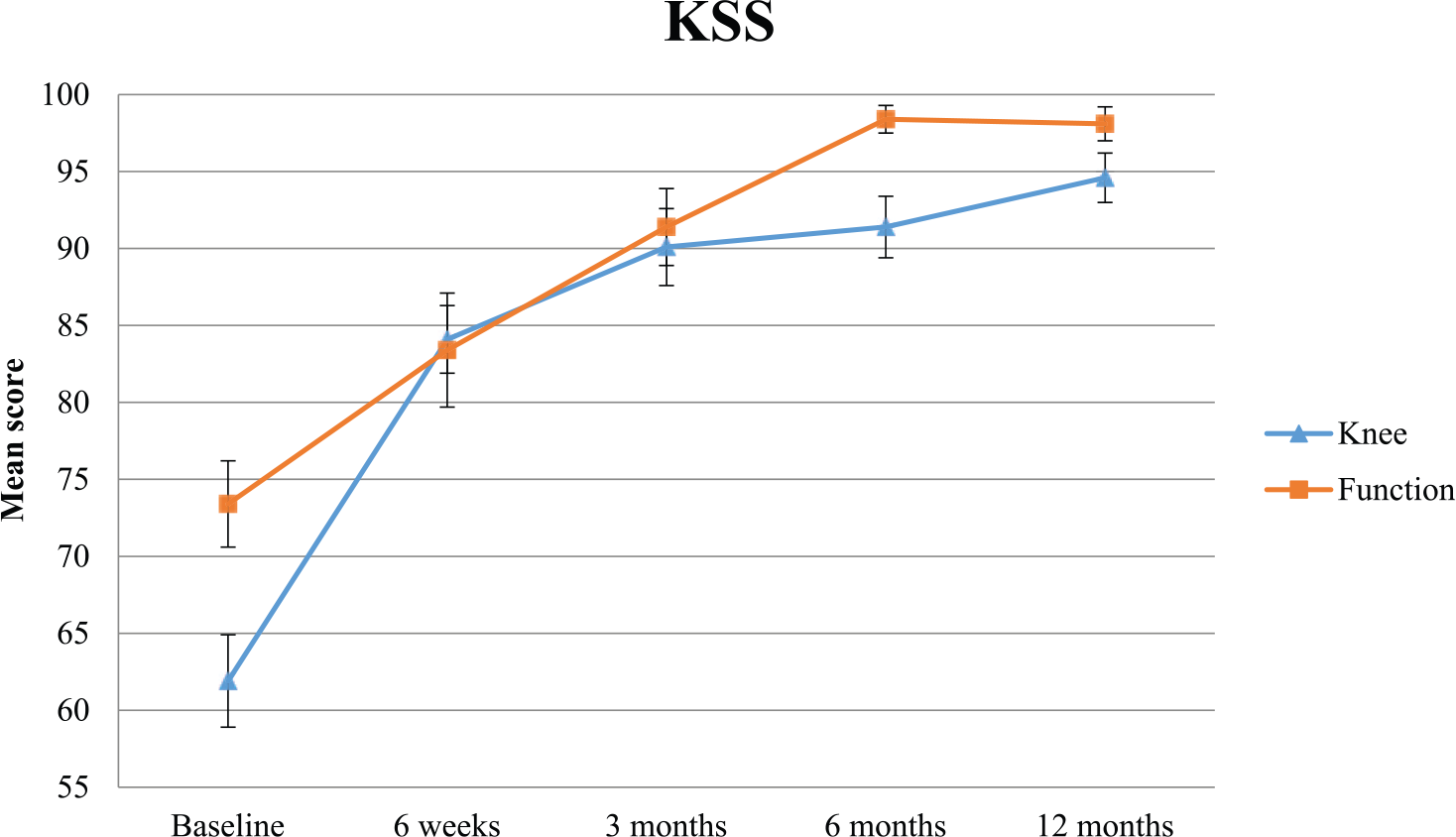
Mean KSS scores from baseline to 12 months. KSS indicates Knee Society Score.
Safety
Nine patients (34.6%) experienced at least 1 AE during the 12-month follow-up period (Table 3). A total of 14 events were reported, and none of them resulted in study discontinuation. Of the 14 events, 3 were classified as serious AEs and occurred in 3 patients (11.5%) (Table 4). One patient (3.8%) had his implant removed due to ongoing knee pain and decreased ROM at 12 months.
Adverse events.

Abbreviation: ROM, range of motion.
A patient can report multiple events.
Serious adverse events (SAEs).

Abbreviation: ROM, range of motion.
A patient can report multiple events.
Discussion
A recent article by the Centers for Disease Control and Prevention (CDC) stated that more than half of adults with arthritis in the United States, an estimated 32 million, are of working age (ie, <65 years old). Osteoarthritis has a substantial impact on everyday activities and reduces activity levels, which may then influence the development and progression of other chronic diseases, such as heart disease and obesity. 6 Young arthritics require a treatment option that will allow them to remain physically active, maintain employment, and manage or prevent other comorbidities. Because OA is affecting a greater proportion of younger individuals, this patient cohort is also experiencing a greater rate of surgical interventions. However, typical surgical options, such as HTO and arthroplasty, require substantial bone cutting and removal, which can complicate subsequent surgery and may offer limited or prolonged return to activity. As these patients are receiving surgery at such an early age, the prosthesis has a greater likelihood of failing over time. Recent studies also point to higher dissatisfaction rates in younger arthroplasty patients. Clearly, there is a clinical need for alternative treatment options for young patients with knee OA who hope to delay or avoid arthroplasty.
This study evaluated the efficacy and safety of the Atlas System for individuals with medial compartment knee OA. Importantly, the inclusion criteria targeted a younger patient population for whom arthroplasty is not the ideal treatment. This patient cohort demonstrated statistically significant improvements across a number of disease-specific outcome measures over 12 months. Impressive responder rates of 96.2% and 92.3% of patients demonstrating a clinically significant ⩾20% improvement in KOOS pain and WOMAC pain scores, respectively, at 12 months indicate that the treatment is well targeted toward the difficult-to-treat young arthritic population.
All concomitant procedures, including arthroscopy, were prohibited in this study of the Atlas System, so the outcomes can be attributed to the joint unloading provided by the implant. Furthermore, the durability of treatment effect out to 12 months suggests that the outcomes are not the result of any placebo effect, particularly because no intra-articular procedures were performed. The clinical trial is still ongoing, and a final evaluation confirming these outcomes at 24 months is expected.
It is important to remember that unloading therapy is not intended to cure the underlying OA disease, and pain with activity is possible. Of the 3 SAEs reported, only 1 involved the medial compartment that this device is intended to treat. This patient was a cycling enthusiast; unfortunately, his treatment expectations were not met and he had elective device removal at 12 months. Importantly, the explant procedure consisted of implant removal and cartilage debridement only, without conversion to any subsequent implant. During removal surgery, the proper function of the device was confirmed. The other SAEs involved uterine bleeding and trochlear microfracture for anterior knee pain, the latter of which indicates preexisting OA in the patellofemoral compartment whose pain may have been unmasked by relief of the medial compartment pain.
The results of this study are consistent with prior investigations on the implant’s predecessor, the KineSpring System, which also unloaded the medial compartment by up to 13 kg. A total of 99 patients treated with the KineSpring System, observed over an average of 17 months, all demonstrated statistically significant improvements in all WOMAC subscales relative to baseline. About 80% of these patients required implant removal and 1 person subsequently converted to a TKA.10,26 In these data on the KineSpring System, the average scores for the WOMAC pain, stiffness, and function subscales at final follow-up were 20, 32, and 22, respectively, compared with 16.3, 28.6, and 18.2 at 12 months in this study. Also, 77.8% of the patients in the KineSpring System group experienced a clinically meaningful ⩾20% improvement in their WOMAC pain score at final follow-up, whereas 92.3% achieved such an outcome in this study at 12 months. In a 5-year case series of 12 KineSpring System patients, Hayes et al 25 also found statistically significant improvements from baseline in WOMAC pain, WOMAC function, and the KSS as early as 6 weeks postsurgery, which all remained significant throughout the study. In this same trial, mean KSS function scores were 83.2, 84.2, 97.3, and 98.2 at 6 weeks, 3, 6, and 12 months, respectively, compared with similar values in this study. Madonna et al 27 reported significant improvements in WOMAC pain and function and in all KOOS subscales 12 months after treatment with the KineSpring System in a group of 53 patients. In this same patient group, 3 individuals (5.7%) had their device removed, 27 whereas 1 patient (3.8%) had an implant removal in this study. Another investigation of 9 patients treated with the KineSpring System also demonstrated significant improvements in all WOMAC subscales over a 2-year period. 35 The results of this study of the Atlas System, combined with the body of evidence from the KineSpring System, support the clinical utility of unicompartmental joint unloading implants.
A strength of this study was that it had a strict eligibility criteria and a rigorous protocol, which ensured that the sample included the targeted patient population and accurate data collection at predefined study time points. The instruments included in this investigation (ie, the KOOS, WOMAC, and KSS) are validated, disease-specific measures that assess numerous dimensions that are considered important to this patient population. A limitation of this study was that it might be considered short-term relative to previous studies examining this patient population.36–38 The planned analysis of the 24-month data will provide further knowledge regarding the safety and efficacy of this implant. Future studies will also require greater sample sizes to obtain more accurate and precise estimates of the intervention’s effect. Because this trial used an experimental, single-arm design, it is difficult to evaluate, directly, how the Atlas Knee System compares with other knee OA interventions. Randomized trials are considered the gold standard study design when estimating comparative effects between treatments; however, studies involving surgical interventions may have additional concerns to address regarding ethics and feasibility.39–41 In this particular case, we must also consider patient preferences to avoid potential randomization to a more invasive procedure, the different indications and contraindications of these various therapies, and surgeon experience. For example, arthroplasty tends to be recommended for patients who have more advanced disease, are older, and less active than those who may be offered a joint unloading device. Finally, this investigation took place at clinical sites in Poland and South Africa only, so it is unclear whether the results would also be generalizable to patients with knee OA in other geographical locations. Although these results are not conclusive, they are promising and provide rationale to continue research on the device.
Conclusions
This study highlights the potential benefit of a joint unloading device in the management of younger patients with mild to moderate medial knee OA. In this single-arm, multicenter trial of 26 patients, the Atlas System demonstrated statistically significant and clinically meaningful improvements in clinical outcomes over 12 months. This interim analysis established the short-term efficacy of the Atlas System; however, a greater follow-up period, spanning many years, is required to assess the long-term durability and safety of the implant. The trial is still ongoing and another evaluation is planned once all the patients complete their 24-month visits.
Footnotes
Acknowledgements
The authors thank Christopher Vannabouathong for his assistance in preparing the manuscript.
Peer review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1439 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Moximed, Inc.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Konrad Slynarski, Dr Jacek Walawski, Dr Robert Smigielski, and Dr Willem van der Merwe were clinical investigators in the PHANTOM High Flex Trial.
Author Contributions
KS, JW, RS, and WvdM conceived and designed the experiments; analyzed the data; wrote the first draft of the manuscript; contributed to the writing of the manuscript; agree with manuscript results and conclusions; jointly developed the structure and arguments for the paper; made critical revisions and approved final version; and reviewed and approved the final manuscript.