
Abstract
Pulmonary arterial hypertension (PAH) is a disease that leads to characteristic vascular wall remodeling and hemodynamic alterations. Consequently, this pulmonary vascular disease contributes to substantial morbidity and mortality in afflicted patients. PAH may be idiopathic in nature or associated with connective tissue disease, chronic liver disease, human immunodeficiency virus, congenital heart disease, and a growing list of other conditions. There are currently nine Food and Drug Administration-approved therapies for specific PAH treatment. Therapeutic targets include prostacyclin replacement, endothelin-1 antagonism, and phosphodiesterase-5 inhibition. This article focuses on the prostanoid treprostinil and explores its role in the management of patients with PAH.
Keywords
Introduction
Clinical classification of pulmonary hypertension (Dana Point, 2008).
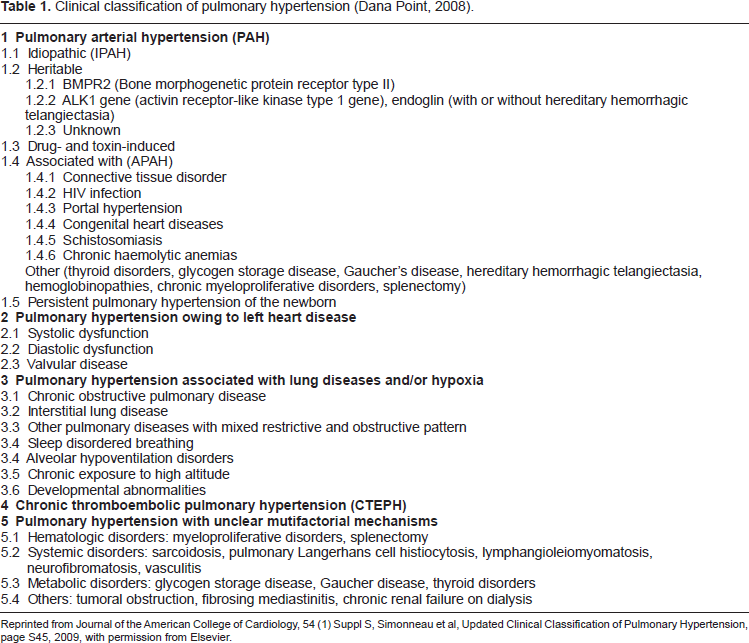
Reprinted from Journal of the American College of Cardiology, 54 (1) Suppl S, Simonneau et al, Updated Clinical Classification of Pulmonary Hypertension, page S45, 2009, with permission from Elsevier.
Though strides have been made in the field of pulmonary vascular disease, including a wider array of pharmacologic therapies to choose from, it still remains a life-threatening diagnosis. In 1995, the Food and Drug Administration (FDA) approved intravenous epoprostenol for the treatment of severe idio-pathic PAH (IPAH) and expanded approval in 2000 for scleroderma-related PAH. This was followed in 2001 by approval of bosentan—a competitive antagonist of endothelin-1—a vasoconstrictor, for WHO Group I patients with New York Heart Association (NYHA) Functional Class II-IV symptoms. In 2002, a second prostacyclin analogue—treprostinil was approved for continuous subcutaneous (SC) infusion. The first inhalable prostacyclin analogue iloprost was approved in 2004, followed by the oral phosphodiesterase inhibitor sildenafil in 2005. On the basis of the bioequivalence 2 of subcutaneous and IV treprostinil, the FDA approved IV treprostinil for continuous administration for PAH patients with NYHA class II, III, and IV signs and symptoms in 2004. Two years later, an additional indication for diminishing the rate of clinical deterioration in patients requiring transition from continuous IV epoprostenol to IV treprostinil was approved. The inhaled form of treprostinil was approved for use in July 2009, followed by another phosphodiesterase inhibitor tadalafil that year.
Epoprostenol, or prostacyclin, is the single most important advance in the treatment of idiopathic (or primary) PAH. This potent, short-acting vasodilator and inhibitor of platelet aggregation is produced by vascular endothelium. However, epoprostenol therapy is associated with problems due to its short half-life (3-5 min), necessitating continuous parenteral infusion via a central venous catheter. Treprostinil is a synthetic prostacyclin analogue that possesses similar pharmacological properties to epoprostenol and unlike epoprostenol, is stable at room temperature and has a neutral pH with an elimination half-life of 4.5 hours. These properties permit the delivery of treprostinil via intravenous (IV), subcutaneous (SC), inhaled, and oral formulations.
Mechanism of Action
The basic lesions of PAH include medial hypertrophy, fibrosis, and plexiform lesions with or without thrombo-occlusive vascular lesions. These lesions are found in varying degrees and also differ in respect to their distribution within the pulmonary vascular bed. 3 Excesses of endothelin-1 and thromboxane, and relative deficiency of endogenous prostacyclin and nitric oxide appear to be responsible at least in part for the described changes. Thromboxane and endothelin-1 contribute to vasoconstriction and smooth muscle proliferation while nitric oxide and prostacyclin oppose these effects. This pulmonary vascular dysregulation represents the rationale for the exogenous therapeutic administration of prostacyclin. Prostacyclin was originally discovered in 1976 by Nobel Laureate John Vane. 4 This compound was found to be a potent vasodilator. The mechanism of action of prostacyclin in PAH is multifactorial. Prostacyclin and its analogues (prostanoids) are potent vasodilators that also possess antithrombotic, antiproliferative and anti-inflammatory properties. As a group, prostacyclins improve exercise capacity, quality of life and hemo-dynamics in patients with symptomatic PAH.
Prostacyclins are potent inhibitors of platelet function. They inhibit platelet activation on several levels, including platelet aggregation, agonist-induced Ca2+ influx and release of α-granular content. In addition, these compounds are active vasodilators and exert cytoprotective effects that are not fully understood. Prostacyclin analogs are thought to work primarily through prostacyclin receptors linked to cyclic AMP (cAMP) generation, but also activate cell-surface and nuclear PGE receptors, and nuclear peroxisome proliferator activated receptor (PPAR) gamma which explains most of the biological effects. Stimulation of PGE2 nuclear receptors modulates nuclear calcium and gene transcription. 5
Recent studies have also shown that PPAR gamma is activated through the IP receptor via a cyclic AMP-independent mechanism and contributes to the anti-proliferative effects of prostacyclin analogues. 6
Prostacyclin analogues have also been shown to inhibit vascular remodeling in pulmonary hypertension and through proliferation inhibition of human pulmonary artery smooth muscle cells (PASMCs). 7
Metabolism and Pharmacokinetics
Treprostinil is a tricyclic benzidene analogue of prostacyclin that has similar biologic actions. This prostanoid is rapidly and completely absorbed after subcutaneous administration with an absolute bio-availability of 100 percent. Continuous subcutaneous infusion of treprostinil is associated with steady state plasma concentrations after approximately 10 hours. The pharmacokinetics of continuous subcutaneous treprostinil is linear over the dose range of 1.25 to 125 ng/kg/min (corresponding to plasma concentrations of about 15 pg/mL to 18,250 pg/mL). Dose proportionality at higher rates has not been studied. A multicenter, open-label, multiple-cohort, steady-state, pharmacokinetic study in subjects with PAH receiving treprostinil by continuous IV or SC infusion at doses between 10 and 125 ng/kg/min demonstrates linearity at treprostinil doses up to 125 ng/kg/min. 8 The volume of distribution of the drug in the central compartment is approximately 14 L/70 kg ideal body weight. Treprostinil at in vitro concentrations ranging from 330-10,000 mcg/L was 91 percent bound to human plasma protein.
The elimination of treprostinil is biphasic; it has an elimination half-life of 4.5 hours and a distribution half-life of 40 minutes. In a chronic pharmacokinetic study in normal volunteers with SC treprostinil doses ranging from 2.5 to 15 ng/kg/min steady-state plasma treprostinil concentrations achieved peak levels and trough levels twice daily. The peak concentrations were found to be approximately 20% to 30% higher than trough concentrations in this study. 9
Pharmacokinetic information for single doses of inhaled treprostinil was obtained in healthy volunteers in three separate studies. Treprostinil systemic exposure post-inhalation was shown to be proportional to the doses administered (18 mcg-90 mcg). In a three-period crossover study, the bioavailability of two single doses of inhaled treprostinil (18 mcg and 36 mcg) was compared with that of IV treprostinil in 18 healthy volunteers. Mean estimates of the absolute systemic bioavailability of treprostinil after inhalation were approximately 64% (18 mcg) and 72% (36 mcg). 10
The metabolism of treprostinil is hepatic. Approximately 79% of the administered dose is excreted in the urine either as unchanged drug or an identifiable metabolite. The clearance of treprostinil is decreased up to 80% in patients with hepatic impairment. In patients with hepatic disease, it is recommended that the initial treprostinil dose should be at least halved, and subsequent increments in treprostinil doses also should be reduced. There are no studies on the pharmacokinetics of treprostinil in patients with renal insufficiency. Information on drug interactions is limited to studies conducted with the oral and injectable formulations. 7
Treprostinil is metabolized by cytochrome P450 (CYP) 2C8; co-administration of inhibitors (eg, gemfibrozil) or inducers (eg, rifampin) of this enzyme may increase or decrease exposure to trepro-stinil, respectively. Treprostinil has not been shown to induce or inhibit other common cytochrome (CYP) P450 enzymes. 9
Anticoagulation with warfarin is recommended in PAH therapy. 11 A single-blind, controlled, crossover study was conducted by United Therapeutics Corp. to evaluate the effect of subcutaneous treprostinil infusion on the pharmacodynamics and pharmacokinetics of a single dose of warfarin. Mean time to attain peak concentration, half-life and elimination rate constant for warfarin did not differ significantly during infusion of subcutaneous treprostinil. No significant adverse events, laboratory findings or anticoagulation-related events were reported. 12
Safety/Adverse Effects
Chronic IV infusions of treprostinil are delivered using an indwelling central venous catheter. This route is associated with the risk of blood stream infections (BSI) and sepsis, which may be fatal. Therefore, continuous subcutaneous infusion is an alternative mode of administration.
The most common side effects of this compound included those related to the method of infusion. For subcutaneous infusion, infusion site pain and infusion site reaction (redness and swelling) occur in the majority of patients. These symptoms are often severe and could lead to treatment with narcotics or discontinuation of treprostinil. For intravenous infusion, line infections, sepsis, arm swelling, tingling sensations, bruising, and pain were most common. General side effects (>5% more than placebo) were diarrhea, jaw pain, vasodilatation, and edema. In an open label study of IV treprostinil (n = 47), there were 7 catheter-related line infections during approximately 35 patient years, or about 1 BSI event per 5 years of use. A Centers for Disease Control and Prevention (CDC) survey of 7 sites that used IV treprostinil for the treatment of PAH found approximately 1 BSI (defined as any positive blood culture) event per 3 years of use. 13
In a 12-week placebo-controlled study—Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension (TRIUMPH I) of 235 patients with PAH (WHO Group 1 and nearly all NYHA Functional Class III symptoms), the most commonly reported adverse reactions of inhaled treprostinil included: cough, throat irritation, headache, gastrointestinal effects, muscle, jaw or bone pain, flushing and syncope. 14
The long term safety of inhaled treprostinil was also studied in an open-label extension study in which 206 patients were dosed for a mean duration of one year. The adverse events during this chronic dosing study were qualitatively similar to those observed in the 12-week placebo controlled trial. 15
Tresprostinil is a Pregnancy Class B drug. The safety of treprostinil is favorable, with no reproductive toxicity or teratogenicity except for an increased incidence of fetal skeletal variations (bilateral full rib or right rudimentary rib on lumbar 1) associated with maternal toxicity (reduction in body weight and food consumption) at an infusion rate of 150 ng/kg/min (about 41 times the starting human rate of infusion, and 5 times the average rate used in clinical trials) in pregnant rabbits. 16
It is not known whether treprostinil is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when treprostinil is administered to nursing women.
Safety and effectiveness in pediatric patients have not been established. Clinical studies of treprostinil did not include sufficient numbers of patients aged ≤16 years to determine whether they respond differently from older patients. Clinical studies did not include patients younger than 18 years to determine whether they respond differently from older patients. In general, dose selection should be cautious. 8
Clinical Trials
The first experiences of prostanoid therapy in PAH patients were published in 1980. 17 In 1995, IV epoprostenol was approved by the FDA for the treatment of severe IPAH, and was subsequently approved in 2000 for PAH related to the scleroderma spectrum of disease. In 1996 and 1998, two important trials18,19 demonstrated that continuous IV infusion of epoprostenol (prostacyclin) improved exercise capacity, hemodynamics, and quality of life in primary pulmonary hypertension. Similar clinical trial results were also demonstrated in scleroderma-associated PAH subjects. 20 Despite these favorable outcomes, continuous parenteral infusion of epoprostenol is far from ideal as a treatment for severe PAH due to its very short half-life (three to five minutes). This delivery method may be associated with severe and potentially fatal side effects. Other prostacyclin analogues and modes of delivery have been developed to treat patients with advanced PAH. The pivotal subcutaneous treprostinil trial by Simmoneau et al in 2002 enrolled 470 patients at 24 US centers and 16 international sites with PAH, either primary pulmonary hypertension, that associated with connective tissue disease or congenital systemic-to-pulmonary shunts in a 12-week, double-blind, placebo-controlled trial. The objective of this study was to assess the effects of SC treprostinil on exercise capacity, disease symptoms, hemodynamics, and quality of life. 21
An intention-to-treat analysis found that exercise capacity improved with treprostinil and was unchanged with placebo and yielded a between-treatment group difference of 16 meters (
In another study by Barst et al, 22 patients who had participated in a previous 12-week study were eligible to enroll in an open-label extension study. In addition, de novo patients were also eligible to enroll in the open-label study. A total of 860 subjects who participated in these studies received SC trepros-tinil therapy for up to 4 yrs. The objectives of this open-label study were to retrospectively analyze the effects of SC reprostinil monotherapy (as well as SC treprostinil therapy with the addition of other PAH therapies if needed) on outcomes in PAH. In a subset of patients with IPAH in whom baseline hemodynamic measurements were available, the authors also compared observed survival with predicted survival, using the formula by D'Alonzo et al. 23
The demonstrated survival was 87%-68% over 1-4 yrs for all 860 patients and 88%-70% over 1-4 yrs with SC treprostinil monotherapy. For the IPAH subset with baseline hemodynamics (n = 332), survival was 91%-72% over 1-4 yrs. In contrast, predicted survival was 69%-38% over 1-4 yrs. The safety profile for long-term SC treprostinil was consistent with previous short-term trials with no unexpected adverse events. 20
Another long-term European retrospective observational study by Lang et al in a total of 99 PAH patients and 23 inoperable chronic thromboembolic pulmonary hypertension (CTEPH) patients showed at the end of three years, after an intention-to-treat analysis, an improvement in NYHA functional class from 3.2 to 2.1, an improvement in the 6MWD, on average by 100 meters, and 1 and 3-year survival rates of 89% and 71%, with event-free survival rates of 83% and 69%. There were 5% treatment interruptions because of local infusion site pain. 24
Treprostinil was initially studied as a continuous subcutaneous infusion. Although most often manageable, the frequency of infusion site pain led ultimately to the development and FDA approval of treprostinil as a continuous IV infusion. The efficacy of IV treprostinil was demonstrated in a 16-week open-label trial of 16 patients that showed an increase in 6MWD of 82 m, and significant improvements in the secondary end points of Naughton-Balke treadmill time (
A recent placebo-controlled trial of IV treprostinil, in treatment-naive PAH patients (42 of 44 with idiopathic/familial PAH with NYHA Class III symptoms) increased 6MWD by a placebo-corrected median of 83 meters (
In July 2009, Treprostinil inhalation solution was FDA approved—the second prostacyclin analog approved in the United States for administration via the inhalation route—with iloprost being available since 2004.
TRIUMPH 1 (Addition of Inhaled Treprostinil to Oral Therapy for Pulmonary Arterial Hypertension) was a 12-week, randomized, placebo-controlled, double-blind, multicenter study to evaluate the safety and efficacy of inhaled treprostinil versus placebo in patients who were receiving stable dose oral therapy—sildenafil or bosentan for at least 3 months prior to enrollment in the study. Patients included were NYHA functional class III or IV and had a 6MWD between 250 to 400 meters. The study demonstrated statistically significant outcomes with respect to its primary endpoint—improvement in peak 6MWD by a placebo-corrected median change of 20 meters from baseline after 12 weeks of treatment (95% confidence interval [CI] = 8-33 m;
An open-label extension of TRIUMPH 1 was undertaken to evaluate long-term effects of inhaled treprostinil (up to 72 mcg four times daily) in 206 patients from the original controlled study for a duration of 24 months. Sixty nine percent of patients appeared to maintain clinical benefit by month 24 as measured by 6MWD and quality of life measurement and survival with a more prominent effect in patients who were initially assigned to active therapy arm in the controlled TRIUMPH 1 study. Most patients (baseline NYHA class III) did not have worsening of NYHA functional class. A further open-label study that followed 27 patients demonstrated similar results with respect to maintenance of clinical benefit and survival rates of 92%, 85% and 75% at the end of 12, 24 and 36 months respectively, though the event-free survival (death, additional therapy, or transplantation) was 50% at the end of the study period of 36 months.14,15
In TRIUMPH 1, 6% of patients treated with inhaled treprostinil compared to 3% of patients on placebo discontinued therapy due to adverse events. The most frequently reported adverse events associated with inhaled treprostinil were cough, headache, dyspnea, and nausea. A surveillance of respiratory tract related adverse events in patients treated with inhaled trepros-tinil is underway due to concerns regarding the potential for oropharyngeal and/or pulmonary toxicity.
Given the availability of a longer-acting, effective inhaled prostacyclin analog, the potential of transitioning patients from the shorter acting iloprost to inhaled treprostinil was examined. A 24-month, multicenter, prospective, open-label trial was designed to evaluate the long-term safety in PAH patients (n = 73) of transitioning from a stable dose of inhaled iloprost to inhaled treprostinil. Data from an interim analysis of 55 patients provided preliminary evidence supporting the safety of rapid transition from inhaled iloprost to inhaled treprostinil while maintaining exercise capacity and improving quality of life. Overall, patients noted significantly improved The Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR) scores after inhaled treprostinil treatment compared with baseline values on iloprost treatment. In addition, the total time spent per day administering inhaled treprostinil was reduced by 66% (81 minutes) compared with that for iloprost at baseline. Significant improvement in median 6MWD was observed after 12 weeks of inhaled treprostinil therapy (426 meters vs. 388 meters at baseline on iloprost;
In 2005, an oral formulation of treprostinil was evaluated as a potential therapy for patients with PAH. Two Phase III multi-national, placebo-controlled clinical trials of oral treprostinil in combination with approved therapy and as monotherapy in patients with PAH to study both safety and efficacy were undertaken.
The FREEDOM-C trial (Oral Treprostinil in Combination with an Endothelin Receptor Antagonist (ERA) and/or a Phosphodiesterase-5 (PDE-5) Inhibitor for the Treatment of PAH) was a 16-week study of oral treprostinil on approved background therapy using a phosphodiesterase-5 inhibitor, such as sildenafil, or an endothelin receptor antagonist, such as bosentan, or a combination of both. This was a negative trial due to side-effects which caused a high patient drop-out rate. 28 Analysis suggests that the inability to dose titrate was a limiting factor that suppressed the overall treatment effect. Of the 174 patients who received oral treprostinil, 25 patients discontinued due to an adverse event and 33 patients completed the trial, but were unable to titrate their doses above 1 mg twice daily. Accordingly, 58 (33%) of the patients in the active treatment group were only able to maintain a suboptimal dose of 1 mg or less twice daily. The trial failed and the dosing and pill formulation was revised for the monotherapy trial (Freedom-M) and a new combination trial (Freedom-C).
Freedom-M (Oral Treprostinil as Monotherapy for the Treatment of PAH) reported a median 6MWD improvement of 23 meters. 29 The Freedom C2 trial failed to reach statistical significance on its 6MWD primary endpoint with a median improvement of 10 m. 30 Both studies missed on secondary endpoints which included change in Borg Dyspnea Score rating, trough walk at Week 11, change in Dyspnea Fatigue Index, change in NYHA functional class, time to clinical worsening (as defined by death, transplant, atrial septostomy, hospitalization due to PAH or at least a 20% decrease in six-minute walk and initiation of another approved PAH therapy), and PAH signs and symptoms.
Place of Treprostinil in current Therapy for PAH
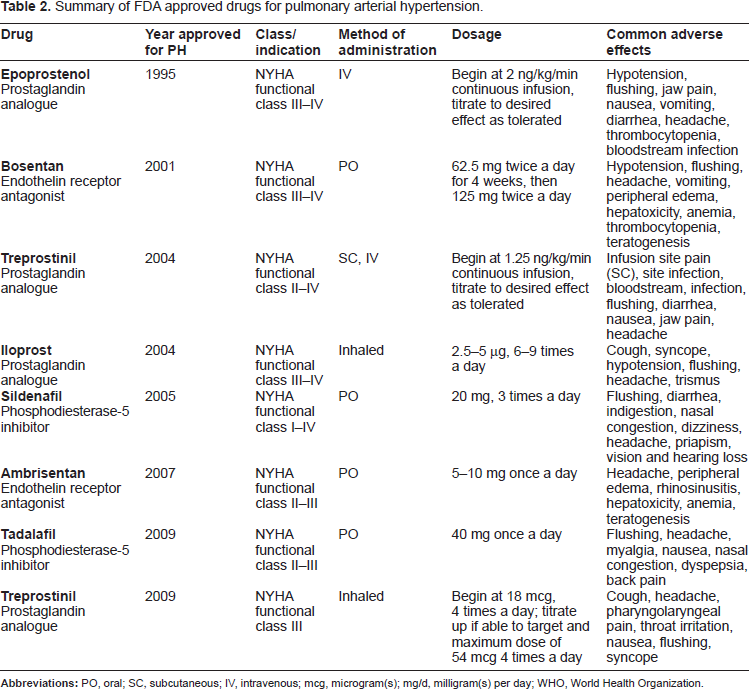
Summary of FDA approved drugs for pulmonary arterial hypertension.
Conclusion
Prostanoid therapy remains the mainstay of treatment for PAH and collective evidence demonstrates that it provides the best benefit in terms of prolonging survival and reducing morbidity in patients with advanced pulmonary vascular disease. The availability of prostacyclin analogues such as treprostinil with its various dosing routes (IV, SC, inhaled) provides flexibility and options for many patients. Nonetheless, any parenteral infusion system remains a substantial treatment impediment for many patients, especially those with more modest symptoms. An oral prostanoid formulation that offers the efficacy previously found only with cumbersome infusion systems could represent an important “next step” in PAH therapy. At this point, we have much to learn in order to fully realize the elusive goal of a highly effective oral prostacyclin agent. Inhaled treprostinil offers an advantage to patients with its dosing schedule when compared to inhaled iloprost that is dosed six to nine times a day, but long-term experience remains to be seen. With the advances in prostanoids, the future looks promising for improved treatment efficacy and better quality of life in patients afflicted with PAH.
Abbreviations
6 minute walk distance
American College of Cardiology Foundation
American Heart Association
blood stream infection
cyclic adenosine monophosphate
Cambridge Pulmonary Hypertension Outcome Review
centers for disease control and prevention
chronic thromboembolic pulmonary hypertension
cyto-chrome P450
endothelin receptor antagonist
European Society of Cardiology
Food and Drug Administration
idiopathic pulmonary arterial hypertension
intravenous
N-terminal pro brain natriuretic peptide
New York Heart Association
pulmonary arterial hypertension
pulmonary artery smooth muscle cell
phosphodiesterase-5
prostaglandin
peroxisome proliferator-activated receptor
subcutaneous
Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension
World Health Organization.
Author Contributions
Wrote the first draft of the manuscript: SM. Contributed to the writing of the manuscript: RF. Agree with manuscript results and conclusions: SM, RF. Jointly developed the structure and arguments for the paper: SM, RF. Made critical revisions and approved final version: RF. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.