
Abstract
Treprostinil is a potent prostacyclin vasodilator indicated for the treatment of pulmonary arterial hypertension (PAH, World Health Organization Group I). Previously, treprostinil was available only in subcutaneous (SC) or intravenous (IV) formulations. Availability of an inhaled formulation of treprostinil has provided clinicians with an alternative to continuous SC or IV treprostinil in appropriate patients. Stable PAH patients whose quality of life has been dramatically impacted by side effects of parenteral therapy or those who have had recurrent, life-threatening bloodstream infections but are otherwise responding well to treatment may be the candidates for continuing prostacyclin therapy with inhaled treprostinil. However, there is little clinical experience with transitioning patients from parenteral to inhaled treprostinil. We present the results of two cases that highlight important considerations in transitioning patients from parenteral to inhaled therapy, including the pharmacologic and clinical equivalence of formulations, dose titration of formulations and suggested criteria for patient selection.
Pulmonary arterial hypertension (PAH) is a chronic, progressive disorder of the pulmonary microvasculature characterized by vasoconstriction, proliferation of pulmonary vascular cells and in situ thrombosis, ultimately leading to right heart failure and death.[1] Prostanoids have remained the gold standard for the treatment of PAH since the introduction of intravenous (IV) epoprostenol and clinicians currently have additional prostanoids and routes of administration at their disposal.[2]
Treprostinil (Remodulin; United Therapeutics Corporation, Research Triangle Park, N.C.) is a prostacyclin analogue that was approved for subcutaneous (SC) administration by the US Food and Drug Administration in 2002 and IV administration in 2004. In clinical studies, SC and IV treprostinil have demonstrated improvements in exercise capacity, functional class, hemodynamics and survival (compared with historic National Institutes of Health registry data).[3–6] Treprostinil has demonstrated efficacy in the treatment of PAH when administered by either parenteral route. However, infusion site pain, a common side effect associated with SC treprostinil[7] and risk of bloodstream infection with IV treprostinil[8] have limited the appeal of parenteral treprostinil for some patients.
In 2009, an inhaled formulation of treprostinil was approved for the treatment of PAH. In a randomized clinical trial of inhaled treprostinil (Tyvaso, United Therapeutics Corporation), 12 weeks of inhaled treprostinil administered four times daily (q.i.d.) to patients on background bosentan or sildenafil improved 6-Minute Walk Distance (6 MWD), quality of life and N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels.[9] Although bioequivalence between the SC and IV routes has been established for treprostinil,[10] it is unclear whether the inhaled formulation given q.i.d., with associated peaks and troughs of treprostinil concentrations in the blood, will be adequate to maintain patients at an equivalent level of disease status as compared with parenteral therapy. Furthermore, it is not clear whether it is serum concentrations or pulmonary tissue concentrations of treprostinil that are more important for clinical efficacy. As treprostinil administered by inhalation is delivered directly to the site of disease, it may be that lower serum concentrations of treprostinil are sufficient to sustain treatment efficacy. Notably, there is little clinical experience transitioning patients from parenteral treprostinil to inhaled treprostinil. We report our experience transitioning from parenteral to inhaled treprostinil in two carefully selected PAH patients.
CASE REPORTS
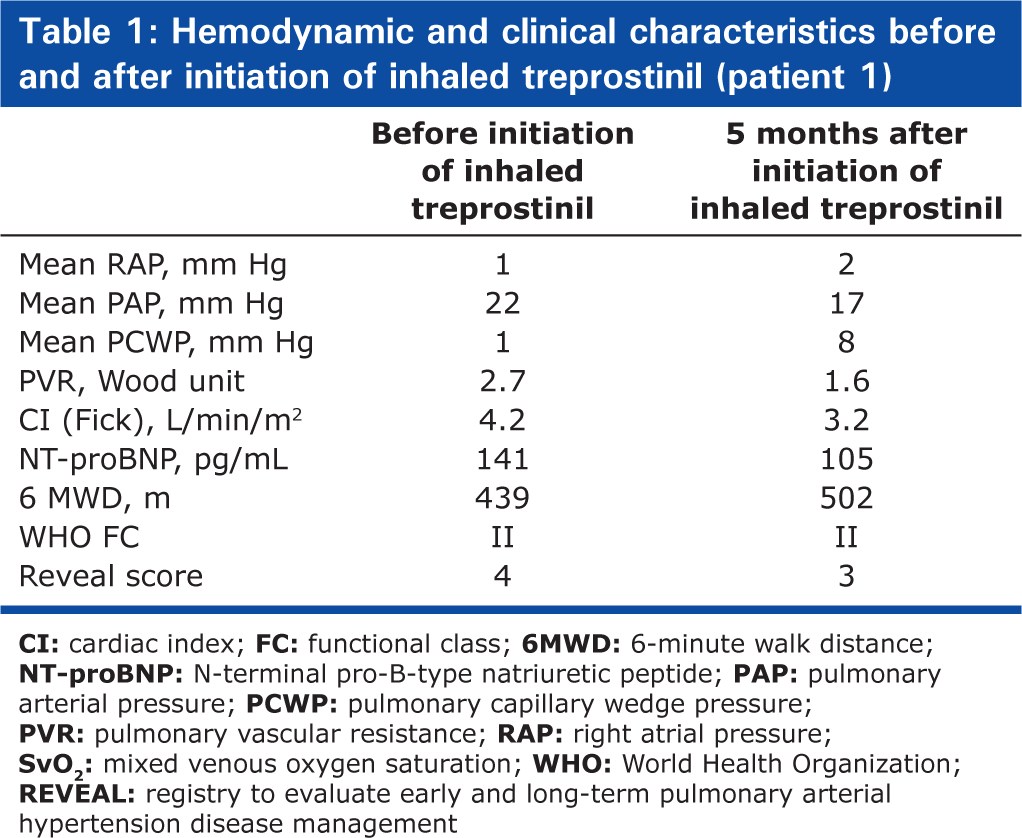
Patient 1 was a 69-year-old Caucasian woman with a 6-year history of idiopathic PAH. She was initiated on PAH therapy with bosentan 125 mg twice daily (b.i.d.) in October 2005 and sildenafil 20 mg three times daily (t.i.d.) in January 2007. She remained symptomatic, however, with worsening hemodynamics. As a result, IV treprostinil was initiated in April 2008, which was associated with significant improvement in her symptoms and hemodynamics. Unfortunately, she developed recurrent life-threatening central line infections while on IV treprostinil in 2009 and was ultimately transitioned to SC treprostinil (maximum dose 38 ng/kg/min) in January 2010. She experienced intractable infusion site pain on SC treprostinil despite topical anesthesia and analgesics, which markedly impacted her quality of life. After extensive discussion, rather than discontinue prostacyclin therapy, she was electively admitted for transition from SC to inhaled treprostinil in April 2010. A right-heart catheterization was performed pre-and post-transition to assess changes in hemodynamics. Inhaled treprostinil was initiated at three breaths every six hours and increased by three breaths daily to a maximum of nine breaths every 6 hours over three days. Simultaneously, the SC treprostinil infusion dose was decreased by 5 ng/kg/min every six hours until cessation of SC treprostinil, with minimal side effects. The total time for SC to inhaled transition was approximately 72 hours. Clinical parameters before and after the transition to inhaled treprostinil are noted in Table 1.
Hemodynamic and clinical characteristics before and after initiation of inhaled treprostinil (patient 1)
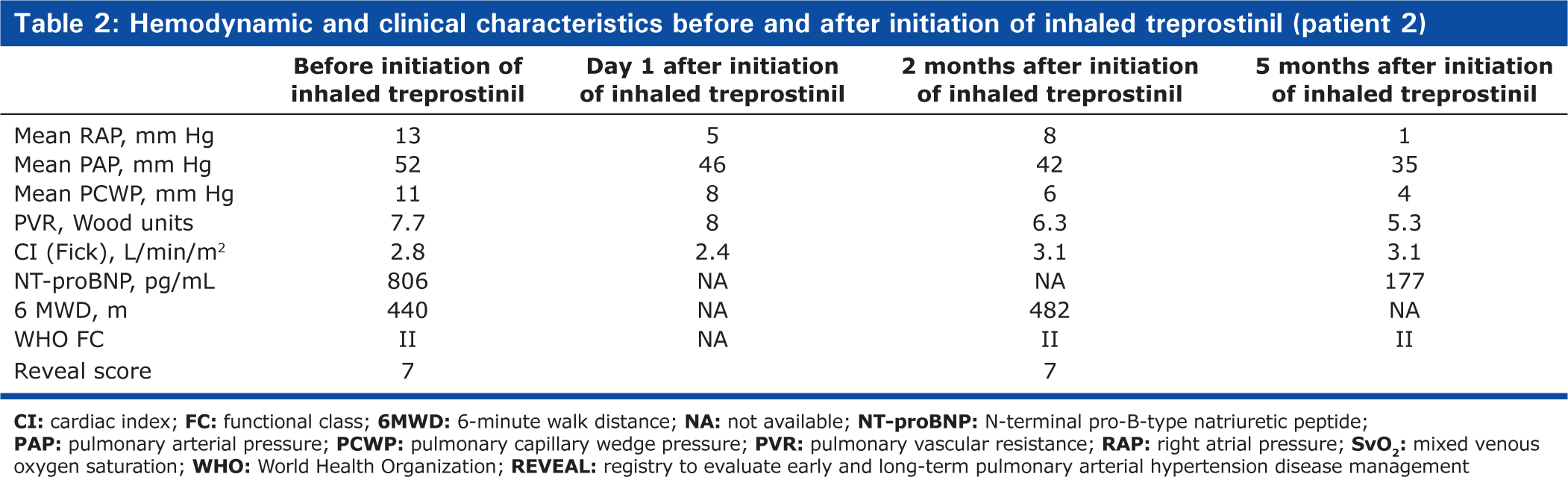
Patient 2 was a 46-year-old Caucasian man with an 8-year history of PAH secondary to β-thalassemia and cirrhosis with splenectomy. He was initiated on PAH therapy with SC treprostinil and up-titrated to 61 ng/kg/min in April 2003. Sildenafil 20 mg t.i.d. was added in July 2006 and bosentan 125 mg b.i.d was added in January 2008. His hemodynamics remained stable on this regimen. However, he developed progressive infusion site pain and serial SC abscesses with life-threatening bacteremia in late 2009 and early 2010. He was offered conversion to IV prostanoid therapy, but he refused given concern over continued infectious risk. Again, rather than discontinuing prostacyclin therapy, the patient was offered transition to inhaled treprostinil in the knowledge that this might not be feasible given his relatively high dose of SC treprostinil. He was admitted in April 2010 for transition from SC to inhaled treprostinil with continuous hemodynamic monitoring in light of the higher dose of SC treprostinil. Inhaled treprostinil was initiated at three breaths every six hours and increased by three breaths daily to a maximum of nine breaths every 6 h over a period of three days. Simultaneously, the SC treprostinil infusion dose was decreased by 5 ng/kg/min every six hours until cessation of SC treprostinil by Day 4, with minimal side effects. Clinical parameters, measured before and after the transition to inhaled treprostinil, are noted in Table 2.
Hemodynamic and clinical characteristics before and after initiation of inhaled treprostinil (patient 2)
DISCUSSION
Of the three drug classes represented in the treatment of PAH, the prostacyclin class is the best characterized, with therapy-induced improvements in patient functional capacity[3–6] and survival.[11] However, IV prostanoids require placement of a central venous catheter, placing the patient at a risk of rare, but potentially fatal, line infections. Although SC treprostinil does not require an indwelling catheter, a majority of patients experience significant pain at the infusion site,[7] as noted in the preceding cases, thereby limiting its use. Inhaled treprostinil presents a potential option in patients who are unable to tolerate the parenteral forms of treprostinil, but in whom continuation of prostanoid therapy is medically indicated.
Recently, Perez et al. reported their experience of transitioning 18 patients with WHO Group I PAH from parenteral prostacyclins to inhaled treprostinil at six tertiary PAH referral centers.[12] Patients were mainly WHO Functional Class II or III and had been stable on prostacyclin therapy for a mean of 110 months prior to transition. The mean dose of IV/SC treprostinil was 73 ng/kg/min and epoprostenol was 10 ng/kg/min. However, at seven months of clinical follow-up, 21% of patients had worsening PAH and clinical symptoms requiring reinitiation of parenteral therapy, indicating that transition should be approached with caution even at experienced centers.
Insights into the challenges associated with transitions from parenteral to inhaled treprostinil are based upon pharmacokinetic (PK) differences between continuous and intermittent delivery of treprostinil. Treprostinil exhibits a terminal elimination half-life of approximately four hours h[13] and is associated with peak and trough concentrations when administered q.i.d. by inhalation. Clinical differences between peak and trough 6-MWD in the TRIUMPH study provide rationale for suspecting variable concentrations of treprostinil in the blood and the pulmonary tissue and may have clinical implications for patients considering transitioning from continuous to intermittent therapy.[9] In that study, the 6 MWD at 12 weeks was improved by 20 m with peak exposure (measured 10–60 min post dosing) compared with 14 m at trough exposure (measured ≥4 h post dosing).[9,12]
Insight into appropriate transition from parenteral to inhaled treprostinil may be extrapolated from a randomized, single-blind, dose-escalation study evaluating the PK profile of inhaled treprostinil.[14] Sixteen of the first 31 patients in this trial were randomized to receive doses of either 30 μg of inhaled treprostinil or placebo, whereas subsequent patients received inhaled treprostinil doses of 60 μg (
In the current series, we have described a relatively simple but rational approach, based on PK data, in which the dose of parenteral treprostinil was decreased in increments of 5 ng/kg/min every six hours with simultaneous rapid up-titration of inhaled treprostinil. Inhaled treprostinil was initiated at a dose of three breaths (18 μg) q.i.d. on Day 1 and up-titrated to six breaths (36 μg) q.i.d. on Day 2 and nine breaths (54 μg) q.i.d. on Day 3. Our up-titration protocol called for a more rapid up-titration than that seen in TRIUMPH, in which the target dose was achieved typically in the second week.[9] We were wary, but we did not observe any significant prostacyclin-related (headache, nausea, flushing, diarrhea, dizziness) or administration-related (particularly coughing) side effectsdue to the rapid up-titration of inhaled treprostinil.
SC treprostinil was being delivered at doses of 38 and 61 ng/kg/min in Patients 1 and 2, respectively. Down-titration of SC treprostinil and up-titration of inhaled treprostinil began concurrently with a reduction in the SC dose of 5 ng/kg/min every six hours until its discontinuation. Since parenteral administration of treprostinilat 15 ng/kg/min would provide a concentration profile likely to exceed the target dose (nine breaths) of inhaled therapy, our transition was based upon this reduction each day in the SC dose. For practical purposes, however, we elected to conduct a daily down-titration of 20 ng/kg/min (5 ng/kg/min every six hours). The first two titrations of inhaled treprostinil (three and six breaths) would be expected to provide concentrations less than a parenteral dose of 20 ng/kg/min; however, both patients were already receiving SC treprostinil as the doses were being down-titrated. Ultimately, both transitions occurred safely over an accelerated period of time (three to four days). Although in-transition hemodynamic parameters for the first patient were not available, in-transition hemodynamic data for Patient 2 suggested that the transition was successful because no deterioration in hemodynamic parameters was evident. Interestingly, longer-term post-inhaled treprostinil hemodynamic data at five months continued to show benefits of inhaled therapy. These hemodynamic findings were validated with observations of 6-MWD, functional class and NT-proBNP concentration.
In terms of identifying patients who may be appropriate candidates for transition to inhaled from parenteral treprostinil, we emphasize that this approach should not be employed routinely in stable patients who are tolerating parenteral prostacyclin therapy given the proven benefits of IV and SC treprostinil. In addition, we risk stratified the patients transitioned to inhaled treprostinil using the multivariable risk prediction algorithm derived from the REVEAL PAH registry.[18] Based on this multivariable risk scoring system, both patients would have a predicted one-year survival < 95% prior to the transition and we noted that REVEAL scores did not change appreciably at follow-up after the transition.
We recommend that offering transition to inhaled treprostinil should be restricted to carefully selected patients who have preserved functional capacity (WHO Functional Class II), stable clinical course prior to the transition with low risk of one-year mortality based on contemporary risk prediction algorithms such as REVEAL and ideally who are on relatively lower doses of treprostinil (>40 ng/kg/min).
We base the latter recommendation on the PKs of inhaled treprostinil and the effective Cmax achieved with the maximal dose of inhaled therapy as well as prior clinical studies in transitioning from IV prostacyclin to oral bosentan, in which the likelihood of successful transition was higher than in those on lower doses of prostacylcin.[19]
Patients being considered for transition should also have experienced major complications of parenteral prostacyclin therapy such as sepsis, recurrent abscesses, intractable infusion site pain, or inability to appropriately manage the infusion system. Transition, if contemplated, should be made in the hospital setting at an experienced PAH center and preferably with continuous hemodynamic monitoring if the patient is on higher doses of parenteral treprostinil. In addition, close clinical follow-up as an outpatient with biomarker assessment, 6-MWT and WHO functional class is mandatory to ensure stability post-transition.
Because of limitations in how high the dose of inhaled treprostinil can be escalated (there are no data for doses < 54 μg q.i.d.), particular caution is recommended for physicians with patients who are transitioning from high doses of parenteral treprostinil. For this patient group, unless there is an emergent contraindication to parenteral therapy, the best course of action may be to continue parenteral therapy. These case evaluations are limited by the lack of PK data from our patients prior to their transition to inhaled treprostinil. Indeed, the patient receiving the higher dose (61 ng/kg/min) may have had lower plasma concentrations than expected because of altered site integrity and related absorption due to SC abscesses.
In summary, transitioning from SC to inhaled treprostinil can be achieved successfully in carefully selected patients with preservation of functional capacity, hemodynamics and quality of life. The transition protocol employed was relatively simple and was based on established PK characteristics of treprostinil administered by continuous infusion and by intermittent inhalation. In this clinical setting of drug transition (parenteral to inhaled), we defined success as “maintenance of disease status without clinical deterioration.” Based on this definition, the cases presented here were considered to be successful. These cases provide guidance to physicians who are experienced in managing patients with PAH on prostanoid therapy and are considering transitioning selected patients from parenteral therapy to inhaled therapy.