
Abstract
Hepatocellular carcinoma (HCC), one of the leading causes of cancer deaths in the world, is offering a challenge to human beings, with the current modes of treatment being a palliative approach. Lack of proper curative or preventive treatment methods encouraged extensive research around the world with an aim to detect a vaccine or therapeutic target biomolecule that could lead to development of a drug or vaccine against HCC. Biomarkers or biological disease markers have emerged as a potential tool as drug/vaccine targets, as they can accurately diagnose, predict, and even prevent the diseases. Biomarker expression in tissue, serum, plasma, or urine can detect tumor in very early stages of its development and monitor the cancer progression and also the effect of therapeutic interventions. Biomarker discoveries are driven by advanced techniques, such as proteomics, transcriptomics, whole genome sequencing, micro- and micro-RNA arrays, and translational clinics. In this review, an overview of the potential of tissue- and serum-associated HCC biomarkers as diagnostic, prognostic, and therapeutic targets for drug development is presented. In addition, we highlight recently developed micro-RNA, long noncoding RNA biomarkers, and single-nucleotide changes, which may be used independently or as complementary biomarkers. These active investigations going on around the world aimed at conquering HCC might show a bright light in the near future.
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide and the third leading cause of cancer mortality. HCC is defined as a primary tumorigenesis in the liver, mainly in patients suffering from chronic liver cirrhosis or hepatitis B or C. The tumor gradually spreads to hepatocytes and in advanced stages metastasizes to other organs, such as lungs and brain. HCC has become one of the very common cancers causing death, affecting more than 500,000 people in the world. 1 The other main risk factors for HCC are alcohol and aflatoxin.2,3
The Development of HCC
HCC is one of the major liver-related mortalities in cirrhosis. As shown in Figure 1, when the healthy liver is affected by hepatitis B virus (HBV) or hepatitis C virus (HCV), a gradual chronic infection leads to liver cirrhosis. Cirrhosis is characterized by a decrease in the growth of healthy hepatocytes and is due to degeneration and regeneration of cells. 3 Regeneration leads to increase in fibrous scar tissue following the destruction of the healthy liver cells, which provides the environment for forming cancerous tumors. 4 Telomerase, which plays an important role in maintaining telomere length and chromosomal stability in hepatocytes 5 and their shortening, limits the regenerative capacity of organs during chronic disease. 6 In a cirrhotic liver, the telomeres of the hepatocytes are significantly shorter than in noncirrhotic tissue. 6 Telomere dysfunctions, along with p53 mutation, are associated with the onset of early-stage hepatic neoplasms. 7
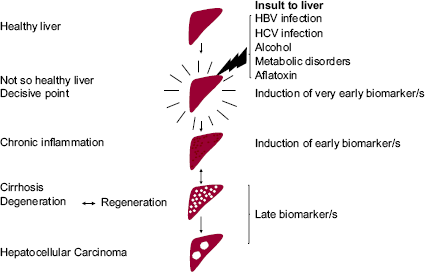
Stages of Hepatocellular carcinoma development and induction of biomarkers. Highlighted liver indicates decisive stage during which liver is either dysregulated by insult or it tolerates such insult till certain limits.
Another characteristic of cirrhosis is the activation of stellate cells. This leads to an increase in the production of cytokines, growth factors, and products of oxidative stress, many of which have been shown to affect hepatocyte proliferation and so could play a role in tumor formation. 8
The main oncogenic pathways involved in HCC are phosphoinositol-3-kinase (PI3K)/Akt, myc, Wnt/β-catenin, c-Met, and hedgehog (Fig. 1–4).9,10 Activation of Akt signaling is thought to promote tumor formation by suppressing transforming growth factor (TGF)-β-induced apoptosis, which in turn activates Wnt/β-catenin signaling, so further driving the hepatocarcinogenic process.
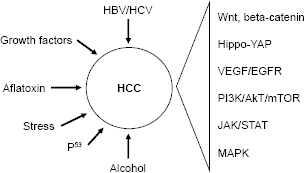
Main factors and signaling involved in hepatocarcinogenesis.
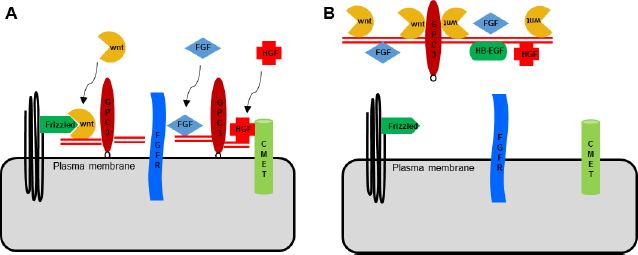
Mechanism of action of sGPC3. (
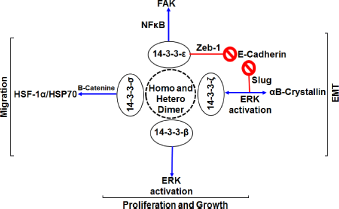
14-3-3-HSF-1/HSP70 cell signaling in HCC cells. Modified from Wu YJ, Jan YJ, Ko BS, Liang SM, Liou JY. Involvement of 14-3-3 proteins in regulating tumor progression of hepatocellular carcinoma. Cancers. 2015;7(2):1022-1036, under the Creative Commons Attribution License.
Current HCC therapeutic and management methods
HCC patients are subjected to multiple treatments, including transcatheter arterial chemoembolization, brachytherapy with radioactive yytrium,11–13 and also cytokine/hormonal therapy, such as interleukin (IL)-2. 14 A potent drug sorafenib, an oral agent with antiangiogenic, proapoptotic, and Raf-kinase inhibitory properties, has been safely evaluated in clinical phase II and phase III trials.15–17 Several drugs modulating different cell signaling mechanisms, mainly PI3K-Akt, mammalian target of rapamycin (mTOR), and RAF/MEK/ERK pathways, are being investigated for their effectiveness to control the progression of HCC. For example, KU-0060648 was found to inhibit HCC cell proliferation by both DNA-activated protein kinase-dependent and -independent mechanisms. 18 A study involving VO-OHpic, a phosphatase and tensin homolog (PTEN) inhibitor in HCC cells, demonstrated that VOOHpic inhibited HCC cell viability, cell proliferation, and colony formation in synergy with PI3K/mTOR and RAF/MEK/ERK pathway inhibitors. 19 Antroquinonol, a traditional Chinese liver treatment drug, exhibited anticancer activity by activating 5′-adenosine mono phosphate (AMP) kinase and inhibiting mTOR pathway, 20 leading to G1 cycle arrest and cellular apoptosis. In another study, it is shown that overexpression of far upstream element-binding protein in HCC and other cancers,21,22 which is directly regulated by P13K/Akt/mTOR pathway, could be substantially reduced by sorafenib.23,24
Role of biomarkers in HCC
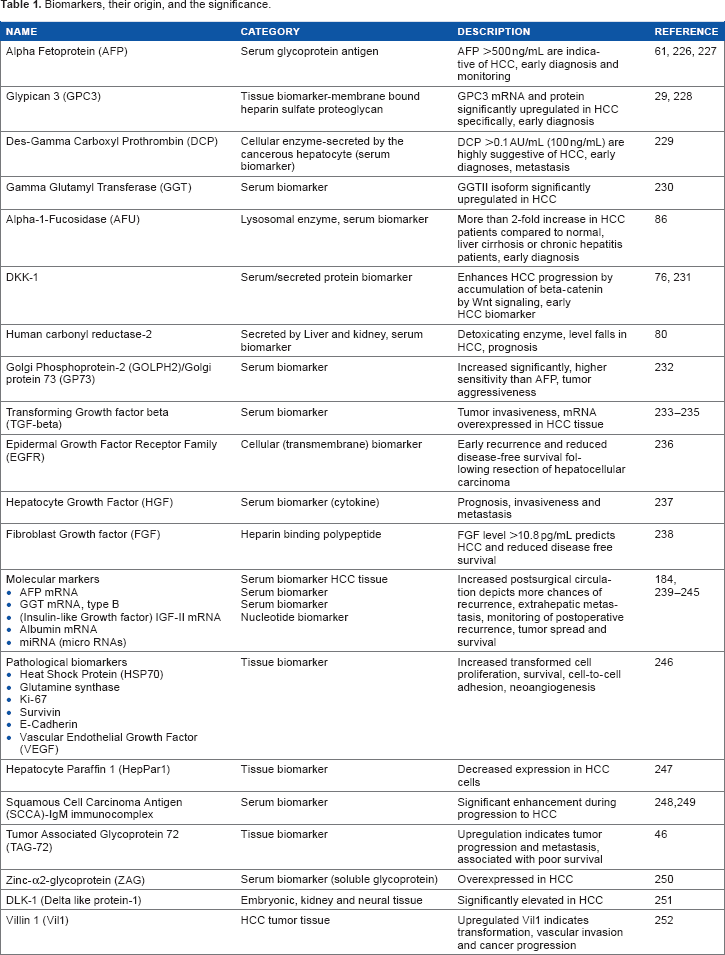
Biomarkers, their origin, and the significance.
Tumor Tissue Biomarkers of HCC
The biopsies and extensive research on tumor tissues of HCC provide a wide range of information about the abnormal constituents of tumor cells and what constituent is upregulated in transformed or neoplastic conditions. This information has provided researchers with therapeutic targets for vaccine, drug development, and screening for surveillance or device prognostic measures to prevent HCC in the past couple of decades.25–28 Here, we focus on some of the potential tissue biomarkers of HCC that function as appropriate targets for early diagnosis and development of antimetastatic vaccines/drugs.
Glypican-3
Glypican-3 (GPC3), a potent tissue biomarker of HCC, links to the cell membrane by a glycosylphosphatidylinositol anchor. It is a heparan sulfate proteoglycan that is involved in regulating the cell growth. Besides, GPC3 can remove growth factors, such as hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF), from the cell surface and inhibit the growth of HCC.29,30 GPC3 is particularly expressed in HCC, but it is not produced by normal or cirrhotic hepatic cells.29,31 Genetic studies in many mammals exhibited that glypicans can regulate the signaling of Wnt, hedgehog, and FGF.32–35
The glypicans interact with Wnts and their signaling receptors, the frizzleds. 36 The GPC3 stimulates Wnt signaling activity by stabilizing the interaction with of Wnt with frizzled, resulting in the proliferation of the HCC cells. The GPC3-induced stimulatory activity requires the attachment of GPC3 to the cell membrane. 36 In a study by Zittermann et al, 30 it was demonstrated that a mutant GPC3 could not attach to the cell membrane (sGP3) and is secreted extracellularly (in the serum) and, thus, could remove the autocrine/paracrine Wnt from the cell surface of the HCC. The removal of Wnt could inhibit the proliferation of HCC and block the activity of FGF, VEGF, epidermal growth factor, and HGF.37–39 Hence, sGPC3 (mutant GPC3) is a potent tissue biomarker that can be targeted for HCC management.
Heat shock protein 70
Heat shock protein 70 (HSP70) is an essential molecular chaperon upregulated in response to heat, stress, or cell survival protection, tightly controlled by heat shock factor-1 (HSF-1). Studies have demonstrated that HSF-1 and HSP70 are involved in HCC tumor invasion and metastasis.40,41 It has been demonstrated that 14-3-3σ protein induces HSP70 via a β-catenin/HSF-1-dependent pathway, which in its downstream modulates HCC. 42 Hence, 14-3-3σ-HSF-1 or HSF-1/HSP70 complex is another important tissue biomarker to be targeted for developing a prognostic tool for HCC.
Tumor-associated glycoprotein 72
Tumor-associated glycoprotein 72 (TAG-72) is a cell membrane mucin-like glycoprotein complex, overexpressed in many of human adenocarcinomas but not in normal tissues.43–45 In a study by Zhang et al, 46 it was demonstrated that TAG-72 is a new tissue biomarker in HCC that indicates the poor survival of patients (Fig. 5).
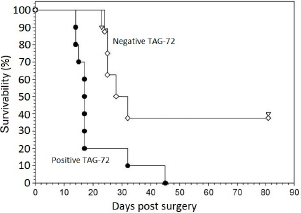
TAG-72 as a potent prognostic marker in various cancers: Curves showing an estimate of overall survivability of cancer patients with absence of TAG-72 expression and presence of TAG-72 expression in cancer tissue after days of treatment.
Ki-67 antigen
Ki-67 is a nuclear protein associated with cellular proliferation. 47 The Ki-67 levels were expressed significantly correlating with higher increases from grades I to IV HCC tumors. This proliferative marker, with increased expression, indicated increased severity or spread of HCC (ranging from a mean+/– SD of 4.1+/–4.01 in tumor grade I to 29+/–15.01 in grade IV tumors). 48
Hepatocyte paraffin 1
Hepatocyte paraffin 1 (HepPar1) is a monoclonal antibody prepared from a failed liver allograft, 49 which recognizes an epitope that is a component of hepatic mitochondria and not found in other normal tissues.49,50 Hep-Par1 is often used as a marker to distinguish between HCC and secondary or metastatic hepatic neoplasms.51,52 A strong HepPar1 expression was detected in majority of the HCC tumors (35 out of 48 HCCs), 53 whereas it was also expressed in nonhepatic tumors, such as lung, gallbladder, stomach, pancreas, colon, and malignant melanoma, but to a much lesser extent.54–58
HERC5
Homologous to the E6-AP carboxyl terminus (HECT) domain and RCC-1-like domain-containing protein 5 is E3 ligase that conjugates with ISG15 to regulate several proteins. One of the main mechanisms of action of this molecule is by induction of CCL20, which in turn increases T regulatory infiltration, and it is one of the important prognostic biomarkers for tumor recurrence in HCC patients as well as survival in liver transplant patients. 59 It is also an important biomarker in the prognosis of lung cancer, and hypermethylation of promoter of HERC5 was associated with poor survival of stage 1 adenocarcinoma.59,60
Serum Biomarkers of HCC
Alpha fetoprotein
Alpha fetoprotein (AFP) is produced by embryonic liver cells during pregnancy. It is in abundance during gestational stages, but its production is minimal after birth. 61 AFP is one of the most common serum biomarkers used for the diagnosis of HCC by clinicians; however, the specificity and reliability of AFP biomarker is questioned, and it is of less value in the early stages of HCC when the tumor size is <3 cm. 62
AFP-L3
It is a different form of AFP that differs in binding affinity with a lectin Lens culinaris agglutinin. This form of AFP-L is used as an early biomarker of HCC when the size of tumor is <2 cm. As the size of tumor increases, the sensitivity of this marker is increased. 63 AFP-L is connected with Ki-67; as a marker of increased nuclear expression of Ki-67, there is a decrease in the expression of β-catenin, which is associated with distant metastasis. 64 In case of the AFP-negative HCC, β-catenin positivity is more common. 65
Glycoprotein 73
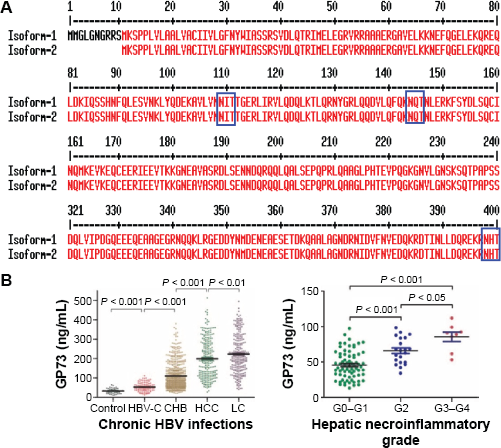
Glycoprotein 73 (GP73) is a type II Golgi-localized phosphoprotein, encoded by Golgi transmembrane type II (GOLPH2) gene located on chromosome 9q21. It is expressed in epithelial cells in several human tissues and was first identified by serum glycoproteomics. 66 GP73 is highly expressed in the tumor part of the liver; however, its expression is comparatively very less in normal part of the same liver.67,68 Similar observations were noted in woodchuck animal model of HCC. 67 Interestingly, it can differentiate patients developing cirrhosis with that of high-grade HCC and is also an early biomarker of HCC. During insult to the liver, ie, acute hepatitis and autoimmune hepatitis, GP73 is highly expressed. Viral infections are also found to increase the GP73 secretion. 69 Oncostatin M, produced in the adipose tissues and a proinflammatory cytokine IL-6, increases the mRNA levels of GP73 as detected in HepG2 cell lines. 70 In addition to HCC, it has been found in other cancers, such as lung adenocarcinoma, testicular seminomas, renal cell carcinoma, and prostate cancer; however, in prostate cancer, it is detected only in urine and not in serum and, therefore, not a specific liver cancer biomarker. 71 As given in Figure 6A, there are two major isoforms of GP73: one is complete and another is incomplete. In the incomplete form, first 10 amino acids at the N-terminal region are lacking and may have functional implications.
(
APO-J
APO-J is a glycoprotein with seven glycosylated sites and is also known as clusterin. 72 It is more sensitive and specific than AFP. 73 APO-J is significantly decreased in HCC patients compared to healthy controls and can be used as an independent marker of HCC. 72 One of the recent studies also showed that it can be used as a prognostic marker and can also monitor HCC progression and metastasis.74,75
DKK-1 Dickkopf-p1
DKK biomarker is of high importance in cases where AFP biomarker misses HCC diagnosis. Importantly, it can diagnose HCC in very early stages of cancer.76,77 One of the studies by Zhu et al reported that DKK-1 can be used as a biomarker for HCC patients undergoing liver transplantation (LT) and can predict the prognosis of such patients. 78 Studies on this biomarker are ongoing, and more robust studies are required to consider it as a biomarker.
Human carbonyl reductase-2
It is expressed in human liver as well as kidneys. During oxidative stress, the released reactive oxygen species and alpha dicarbonyl are detoxified by this enzyme. 79 The expression of human carbonyl reductase-2 (HCR2) is significantly decreased in the tumor part of the liver compared to the normal cells. 80 The decreased expression of carbonyl reductase-2 leads to cancer growth as it triggers the cell damage through reactive oxygen species and other carcinogens.
Midkine
Midkine is expressed at the time of early embryogenesis and is a heparin-binding growth factor. It is expressed during wound healing, tumorogenesis, and inflammation. 81 Compared to AFP, which is significantly raised during advanced stages of HCC, midkine is marginally raised and cannot be used as the biomarker in advanced stages of HCC. However, midkine expression markedly rises during early development of HCC. 82
Des-γ-carboxy prothrombin
It is an important biomarker in large size HCC, and in cases where AFP misses HCC diagnosis, des-γ-carboxy prothrombin is able to detect HCC. 83 It is an abnormal prothrombin protein of VEGF family expressed during vitamin K deficiency/antagonist-II (PIVKA-II). During insult to the liver cells, when normal cells convert to fibroid cells or epithelial-to-mesenchymal transition, hypoxic shock leads to the induction of DES. 84
α-1-Fucosidase
α-1-Fucosidase is a lysosomal enzyme that hydrolyzes fucose glucosidic bonds of glycolipids and glycoprotein. Its expression increases with liver insult similar to chronic hepatitis, cirrhosis, and HCC patients. 85 It is one of the early HCC biomarkers and has a cut-off value of 870 nm/mL/h. Interestingly, it is raised preceding six months of development of HCC, and its value is over 700 nm/mL/h in 85% of HCC patients. 86
Hepatocyte growth factor
HGF is a cytokine produced by nonparenchymal Ito cells in the liver. 87 It stimulates the expression of immediate early genes in primary cultures of hepatocytes. 88 In hepatic regeneration, chronic hepatitis, cirrhosis, and HCC, HGF levels increase, and a level of 1.0 ng/mL indicates poor survival. 89 It acts as a prognostic biomarker and can predict the early tumor recurrence and metastasis. 90
Nerve growth factor
Nerve growth factor (NGF) is a member of neurotrophin family and is important for differentiation, survival, and preservation of peripheral and central nervous systems. 91 NGF levels are associated with tumor growth, invasion, and metastasis. There are two receptors of NGF: high-affinity trkANGF and low-affinity p75NTR. Expression of NGF and trkANGF increases significantly during HCC. It can differentiate between cirrhosis that develops to HCC and cirrhosis that does not lead to HCC. 92
Vascular endothelial growth factor
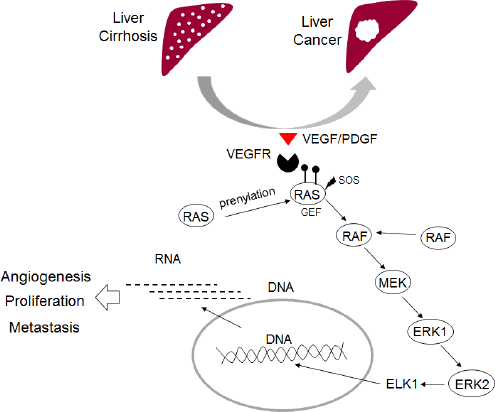
VEGF is a glycosylated cytokine that acts as a mitogen and mediates vascular permeability, angiogenesis, vasculogenesis, and endothelial cell growth-reduced survival. 93 Tumor characteristic and environment promotes VEGF expression and initiates VEGF signaling and thus triggers downstream MAPK cascade (Ras/RAF/MEK/ERK) which is involved in angiogenesis, proliferation and metastasis and is shown in Figure 7. VEGF levels envisage HCC recurrence, and it is a substantial biomarker for the survival of HCC patients.94,95 A phase III clinical study conducted on 602 HCC patients receiving sorafenib showed that VEGF was one of the molecules that predicted patients' survival suggesting its role as a biomarker in the prognosis of HCC. 96
Interaction between VEGF, VEGFR-2, and sVEGFR-2 via MAPK pathway. Modified from Ratnasari N, Yano Y. Do soluble vascular endothelial growth factor and its receptors predict the progression of chronic hepatitis to hepatocellular carcinoma? Hepatitis. 2015;1(1):4, under the Creative Commons Attribution License.
Transforming growth factor-β
TGF-β plays an important role in the control of cellular proliferation and differentiation in HCC cells. Serum TGF-β levels are raised in HCC patients and is a long sought biomarker of HCC. 97 One of the recent reports documented the role of the TGF-β-interacting factor as one of the prognostic biomarkers of HCC. 98 Moreover, its partner mucin1 mediates TGF-β signaling by activating JNK/AP1 pathway and can also be used as a therapeutic target for the treatment of HCC. 99
Epidermal growth factor
Epidermal growth factor receptor (EGFR) signaling is one of the important players in all the phases of hepatic injury from very early stages of inflammation to HCC development, including fibrogenesis and neoplastic transformation. 100 One of the forms of EGFR, ErbB3, was detected in the serum of HCC patients during the early stages of HCC development and was associated with portal vein invasion and metasatsis. 101 One of the recent studies reported that HBV HBx protein downregulates the EGFR expression by inducing miRNA-7 in HCC cells. 102 In addition, it is an important player and has tumor promoting role in non-HCC cells via live resident macrophages. 103 Using an in vivo model, a recent study determined the potential role of soluble EGFR in HCC metastasis. 104
Wnt
Wnt-1 protein has been described as a prognostic biomarker of HBV-related and HCV-related HCC after surgery. 105 GPC3 molecule, which is described in the “Glypican-3” section, promotes the growth of HCC by stimulating Wnt signaling. 106
Angiopointin-1/2
Angiopointin-2 levels are raised in HCC and cirrhosis, and it has been documented by several studies that elevated levels of Ang2 could be used as a marker of advanced pathological invasiveness and overall survival of HCC patients.96,107,108 It is also shown that Ang2 contributes to multiple organ failure and sepsis. 109
NOTCH
Activation of NOTCH plays a prominent role in HBV-mediated HCC by proliferating hepatic cells and further supporting the growth of HCC, and this is also proved in in vivo mouse models.110,111 NOTCH1 is one of the possible therapeutic targets for the treatment of HBx-associated HCC. 112 Recent studies showed that NOTCH1 and NOTCH4 are important biomarkers revealing the poor prognosis of HCC.113,114
Oncostatin M
OSM is a member of cytokine family, which is very early secreted from the hematopoietic cells, and induces the differentiation of hepatocytes by regulating HNF4 alpha. 115 It regulates cytokine production, such as IL-6, GM-CSF, and G-CSF. It is also shown to be elevated in HCC and acts in synergy with IL-6. 116
Alpha-1 antitrypsin
Alpha-1 antitrypsin is a member of the SERPINA1 family of proteins, which is controlled by IL-6, TNα, and IL-1.117,118 Increased levels of A1AT have been associated with HCC. A recent study revealed changes in the status of A1AT glycosylation during HCC and also documented that the core fucosyalation of HCC is one of the main reasons behind such changes. 119 Compared to cirrhosis, it is significantly elevated in HCC and could also be used as a differentiation marker. 120
WFA+ M2BP
Kuno et al 121 first reported an assay that uses Wisteria floribunda agglutinin-positive human mac2-binding protein in assessing liver fibrosis. A recent study by Yamasaki et al 122 showed high value of measuring WFA+ M2BP and highlighted that it can be used as an independent risk factor biomarker for HCC development. Interestingly, WFA+ M2BP can predict HCC in HCV patients who respond well to the treatment and achieve the sustained virological response. 123
Lymphotoxin beta receptor
Lymphotoxin beta receptor is a cytokine and a member of tumor necrosis factor family, which is well known for controlling the development of lymphoid organs. 124 In HCC as well as in cholangiocarcinoma cells, lymphotoxin beta receptor is vastly expressed and sustains the oncogene activity. 125 It correlates with the upregulated Akt/NOTCH1 signaling and is a marker of poor survival in cholangiocarcinoma patients. 126
Long Noncoding RNA as Biomarkers of HCC
MALAT1
Long noncoding RNA (lncRNA) is an RNA molecule with a length of 200 bp to 100 kbp and lacks protein-coding capacity. Metastasis-associated lung adenocarcinoma transcript 1 is the lncRNA of >8 kbp transcribed from chromosome 11q13. Recently, Lai et al 127 reported that an overexpressed MALAT1 transcript could predict HCC recurrence after LT and importantly in those patients whose survival rate was also reduced. There are five SP-binding motifs upstream of the MALAT1, which lead to its overexpression, 128 In addition, an in vitro study suggested an interaction of hn-RNP-C with MALAT1 regulating cell cycle as recently studied in HepG2 cells. 129
HOTAIR
Hox antisense intergenic RNA plays a role in chromatin dynamics, cell differentiation, and cancer metastasis, which is encoded by HOXC gene cluster. 130 Once transcribed, it acts in trans to control the HOXD genes by recruiting the polycomb repressive complex 2 and silencing the transcriptional machinery. 131 Patients with elevated expression of HOTAIR shows poor prognosis compared to those with reduced HOTAIR expression. Yang et al 132 documented that HOTAIR can act as an independent prognostic biomarker in predicting the HCC recurrence in patients undergoing LT.
H19
Oncofetal H19 mRNA is abundantly expressed in the fetus. 133 It is paternally imprinted, which resides at chromosome 11p15.5 and is significantly expressed during tumorogenesis. Compared to AFP, the expression of H19 mRNA is much higher in HCC cases. 134 It also inhibits metastasis by stimulating miRNA-200 and inducing histone acetylation. 135
Highly upregulated in liver cancer
Highly upregulated in liver cancer is a 500 nucleotide lncRNA, which is expressed from chromosome 6p24.3 136 loci. Compared to normal liver tissue, it is highly expressed in adjacent tumor part of the liver. 137 One of the main agents responsible for HCC is HBV infection, particularly HBx. A recent study by Du et al 138 documented an important role of highly upregulated in liver cancer in HBx-mediated HCC and further implicated that it is possible due to the downregulation of p18.
Long interspersed nuclear element-1
Retrotransposons are the jumping genes, and long interspersed nuclear element-1 (LINE-1) is one of the autonomously regulated retrotransposons. A recent study by Tangkijvanich et al 139 tested the hypomethylation status of LINE-1 in 85 patients and concluded that advanced disease and tumor size are associated with levels of LINE-1 hypomethylation. Another report by Piao et al highlighted the role of LINE-1 hypomethylation in early childhood tumorogensis. 140 Gao et al 141 also precisely documented that hypomethylation at two of the sites, CpG 7 and 18, is associated with poor prognosis in HCC.
Micro-RNA biomarkers of HCC
Micro-RNA and its role as biomarkers
A micro-RNA (miRNA) is a small noncoding RNA molecule that mainly functions in RNA silencing. 142 Transcription of miRNA initiates from intronic region of a host gene leading to long pri-miRNA transcript. This is further processed to pre-miRNA, Pre-miRNA then transport to cytoplasm by Exportin, where it goes through further modification by Dicer developing into complete miRNA molecule as given in Figure 8. miRNAs exhibit their silencing activities by base pairing with complementary sequences within mRNA molecules, 143 by cleavage of the mRNA, chopping off its poly(A) tail, or less efficient translation of the mRNA into protein by ribosomes. 144 The human genome encodes for over 1000 miRNAs, 145 most of which are abundant in many mammalian cell types. 146
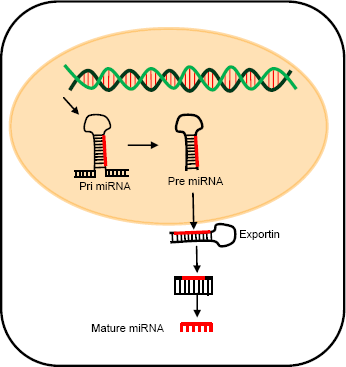
Biogenesis of miRNA. Modified from Anwar SL, Lehmann U. MicroRNAs: Emerging novel clinical biomarkers for hepatocellular carcinomas. Journal of Clinical Medicine. 2015;4(8):1631-1650, under the Creative Commons Attribution License.
Several studies indicate that miRNAs are involved in a variety of physiological processes, including cell proliferation, differentiation, metabolism, and apoptosis. As given in Figure 9, miRNAs regulate important cellular angiogenesis, apoptosis and metastasis pathways. The miRNA was recognized as a distinct class of biological regulators during early 2000s.147,148 Ongoing research has identified different miRNAs expressed in different cells and tissues.146,149 miRNAs are detectable and stable in clinical samples, such as blood, serum, plasma, urine, and feces. Besides, the abnormal expression of miRNAs has been observed under different disease conditions, especially cancers, establishing miRNA as an important biomarker. Hence, new miRNA-based therapies are now under investigation.150–153
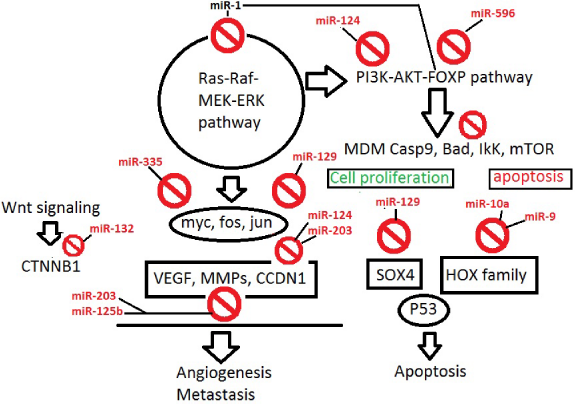
Mature miRNAs silenced by aberrant DNA methylation and their affected target genes and pathways that are important in the development and progression of HCC.
Role of miRNA biomarkers in HCC
miRNA dysregulation has been known to be associated with many cancers, the first studied being lymphocytic leukemia, 154 and hence sometimes referred to as oncomirs. miRNA levels are also used as prognostic for cancers, as low miR-324 levels could serve as indicator of poor survival in non-small-cell lung carcinoma samples. 155 High miR-185 or low miR-133b may correlate with metastasis and poor survival in colorectal cancer. 156 miR-10b is implicated in the metastasis of breast cancer cells 157 and the development of gastric cancer and pancreatic cancer.158,159
A number of studies have demonstrated extensive miRNA dysregulation in various stages of HCC. 160 Furthermore, unique patterns of miRNA expression could be utilized as potential biomarkers for diagnosis, prognosis, staging, and prediction of therapeutic responses in HCC.161–163 Expression of particular miRNAs tends to change gradually during the progression of HCC, and many tumor suppressor genes are demonstrated as the targets of the HCC oncomirs (eg, PTEN for miR-21, miR-221, and miR-222). Specific signaling pathways, such as Wnt/β-catenin, RAS, TGF-β, and JAK/STAT, are established targets for miRNA dysregulation in HCC. 163
A comprehensive demonstration of the role of miRNA dysregulation and differential miRNA expression in HCC has been done.164,165 The advantage of miRNAs is that they are stable in frozen samples, formalin fixed paraffin embedded tissues, and body fluids, including plasma/serum, urine, and saliva. This property of miRNA makes them an excellent tool for early cancer diagnosis.
Primary tissue specimens. Basal miRNA expression has been studied using deep sequencing in primary HCC specimens as well as in the healthy liver.165,166 The most abundant miRNA expressed in healthy liver is miR-122, which is commonly downregulated in HCC. miR-199a/b is also downregulated in HCC and associated with poor survival. 166
Serum. Serum levels of miR-122 are significantly upregulated in HCC patients compared to healthy individuals, and the levels are decreased after therapy. 167 A case study reported by Li et al 168 involving 500 serum samples from HCC patients showed that a combination of three miRNAs' profile change, such as miR-25, miR-375, and let-7f, could distinguish between HCC and healthy controls. Serum levels of miR-16, miR-195, and miR-199a, alone or in combination, could distinguish between HCC and chronic hepatitis. 169 Overexpression of miR-15b, miR-21, miR-130b, and miR-183 is demonstrated in 96 tumors, which indicate that these circulating miRNAs are derived from tumor cells. 168 Lin et al 170 reported very recently that the cluster of seven miRNAs (miR-29a, miR-29c, miR-133a, miR-143, miR-145, miR-192, and miR-505) can detect the HCC with better sensitivity and similar specificity than AFP. Another recent study demonstrated that low miR-150 level in HBV-related HCC patients was associated with a significantly decreased survival (P < 0.0001). 161
Zhou et al 171 reported that a particular miRNA panel was able to specifically distinguish HCC from healthy individuals and HBV and cirrhosis patients, using plasma samples from 934 HBV-associated HCC patients. For example, miR-106 could distinguish between HCC from healthy individuals and chronic hepatitis patients; 172 while four miRNA panels (miT-20a-5p, miR-320a, miR-324-3p, and miR-375) have a high sensitivity and specificity to differentiate HCC from benign liver lesions. 173 These findings clearly demonstrate that circulating miRNAs could be a potential diagnostic marker in HCC. As given in Figure 10, distinctive miRNAs are up-/down-regulated in hepatitis, fibrosis, steatosis and HCC, however miRNA-21, miRNA-122 and miRNA-223 are involved in Hepatitis as well as HCC.
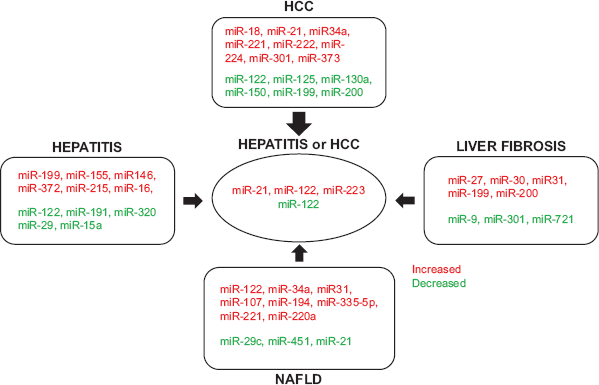
Summary of miRNAs and their targets associated with HCC, liver fibrosis, NAFLD, and hepatitis (HBV or HCV infection). miRNAs that are upregulated are indicated by red text, and miRNAs that are downregulated are indicated by green text.
miRNA as a prognostic tool in HCC
Other than their utility as a diagnostic biomarker, miRNAs are also important as prognostic tool, able to determine the tumor size, nodal, and metastasis stage of HCC, invasion, recurrence, and overall survival. miR-25 has been demonstrated to have a significant role in tumor size, nodal, and metastasis as reported by Su et al; 174 upregulation of miR-183 175 and miR-17-5p 176 in primary HCC samples after surgery has been associated with large tumors and higher risk of metastasis. High miR-221 expression, along with downregulation of miR-100 and miR-22, is demonstrated in primary HCC tissues with distant metastasis.177–179 miR-222 level is important to determine the advancement of the tumor. 180 An overall miRNA profiling study demonstrated that upregulation of miR-25, miR-372, miR-155, and miR-182174,181–183 strongly correlates with shorter survival time, whereas downregulation of miR-29a-5p, miR-100, miR-29, miR-101, and miR-148a in HCC tissues depicts the cure of the HCC and an increased survival.177,184–186
miRNA as a therapeutic target
Currently, active research is going on to utilize these potential diagnostic and prognostic biomarkers as potential therapeutic targets to manage HCC. For therapy, antagonists are being developed against oncogenic miRNAs or oncomirs, referred to as antagomirs (locked nucleic acids). A very interesting example is of miravirsen (anti-miR-122) to treat chronic HCV infection, which is currently on phase III clinical trials. 187 The success of the miRNA-based therapy would definitely lead to the better effectiveness of the current interferon therapy by the downregulation of the cell signaling pathway that generally renders the cells' inter-feron resistant. It is reported that sorafenib, the drug used to treat HCC patients, regulates miRNA expression. Fourteen miRNAs are upregulated by sorafenib treatment. miR-122 is an important liver-specific miRNA that maintains liver homeostasis, so the delivery of miR-122 in HCV-infected patients is currently on clinical trials. 188 miR-122, which is generally downregulated in HCC patients, is restored by sorafenib. 189 Restoration of miR-122 by sorafenib also leads to an increased sensitivity of the tumors to other drugs, such as doxorubicin 190 adriamycin, and vincristine. 191 miR-26b has been shown to affect NF-kB signaling molecules to mediate chemosensitivity. 192 Certain miRNAs when downregulated or upregulated induce drug resistance, hence they are targeted to develop their specific antagomirs to induce drug sensitivity for HCC treatment.
miRNA profiling and expression studies have tremendous potential for the development of new biomarkers, diagnostic and prognostic markers, as well as therapeutic molecules for the management of HCC. Hence, miRNAs are definitely the anticancer medicine for the future.
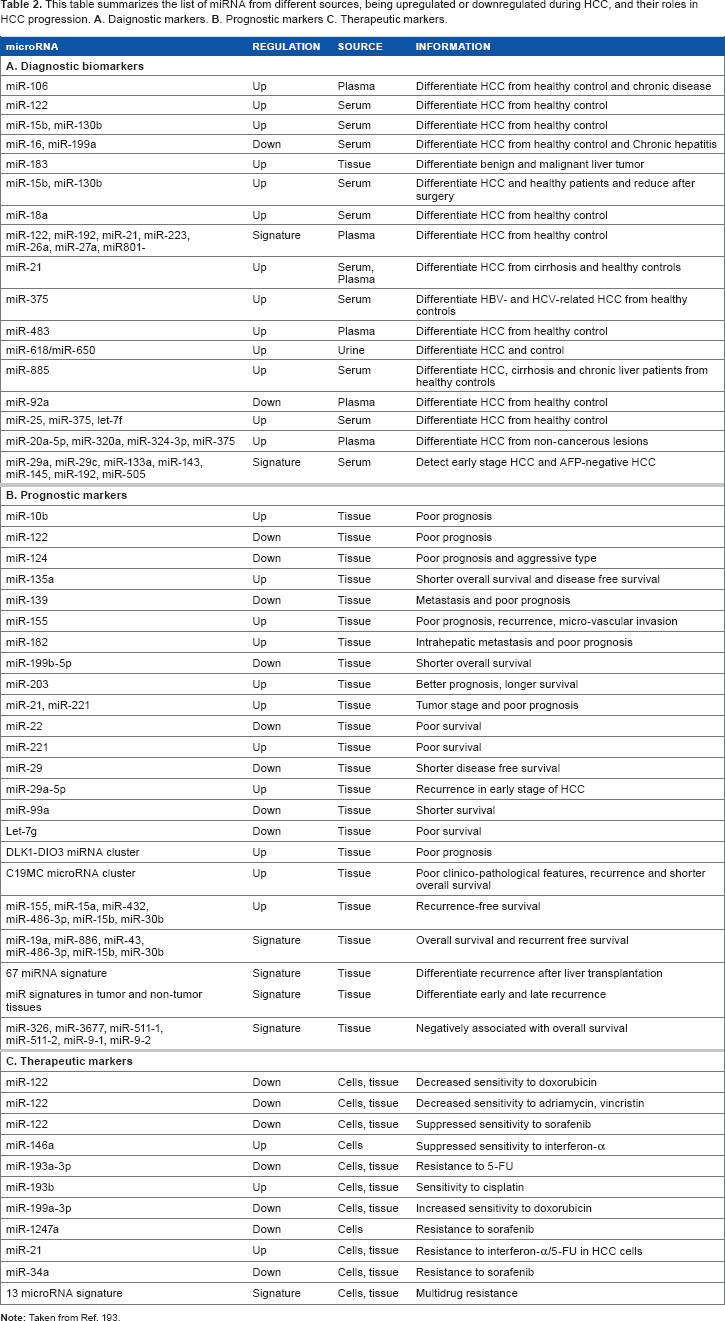
This table summarizes the list of miRNA from different sources, being upregulated or downregulated during HCC, and their roles in HCC progression. A. Daignostic markers. B. Prognostic markers C. Therapeutic markers.
Exosomal miRNA as a biomarker of HCC
One of the recent studies by Sohn et al 194 isolated exosomes from the serum of chronic hepatitis B (CHB), cirrhosis, and HCC patients and found elevated levels of miRNAs, such as miR-18a, miR-221, miR-222, and miR-224, in HCC patients compared to those with CHB or liver cirrhosis (Fig. 11), whereas serum levels of miR-101, miR-106b, miR-122, and miR-195 were lower in HCC patients compared to CHB patients.
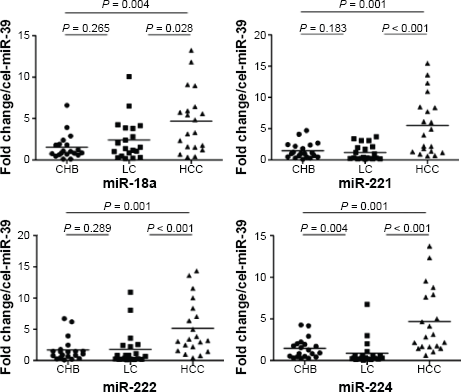
The distribution of upregulated exosomal miRNAs (miR-18a, miR-221, miR-222, and miR-224) in CHB patients, LC, and HCC. Reprinted by permission from Macmillan Publishers Ltd: Experimental & Molecular Medicine, Sohn W, Kim J, Kang SH. Serum exosomal microRNAs as novel biomarkers for hepatocellular carcinoma. Exp Mol Med. 2015;47:e184. Copyright 2015.
Genetic Variants as Biomarkers
P 53 A249S
AGG-to-AGT single-nucleotide transversion leads to change of codon from arginine to serine at position 249 of P 53 gene and one of the important hotspot genetic variations in HCC. 195 It is majorly detected in patients who are exposed to aflatoxin and HBV. 196 Some recent investigations deciphered the mechanisms by which it leads to HCC development: (1) inactivation of p16INK4 gene by overmethylation of this gene 197 and (2) regulation of genes that play a main role in controlling the cell cycle switch from G to S phases. 198
HBV core promoter mutations
HBV mutations in the basal core promoter region are important etiological risk factors for severe liver disease and HCC.199,200 BCP 1762 and 1764 mutations identified as an independent risk factor of HCC.201,202 Using the plasma samples, two studies reported that these mutations have the high predictive power to reveal the predisposition to HCC and its development.203,204
HBV PreS1 mutations/truncations
One of the largest studies, while recruiting 11,582 HBV-infected patients, reported that HBV preS mutants are associated with high risk of HCC. 205 T53C, PreS2 initiation codon mutation, PreS1 deletion, C7A, A2962G, C2964A, and C3116T were significantly associated with HCC.201,206 One of the effects of few such mutations/deletions is that it also alters the overlapping polymerase gene reading frame; for example, rtA181T mutation in polymerase gene leads to stop codon mutation sW172 stop in the surface region and is associated with high risk of HCC development in patients' refractory to the nucleoside therapy. 207 Due to PreS envelope protein mutations/deletions, high-level uneven expression of these proteins leads to endoplasmic reticulum stress, causing genomic instability resulting in HCC. 208
HBx region mutations and truncations
There are two main mechanisms by which HBV causes HCC, ie, direct and indirect. In direct mechanism, it integrates into the host liver cell genome and modulates several host genes in cis manner, 209 and the indirect way is by trans activation of several genes by HBx protein. 210 HBx protein in serum has been shown to be one of the markers of the liver cirrhosis and liver cancer in HBV-infected HCC. 211 HBx induces AFP and promotes malignant transformation of hepatocytes by activating PI3K/mTOR signaling. 212
Genetic Variations Identified by Next-generation Sequencing
Accumulation of genetic alterations is one of the most important mechanisms of causing HCC. Next-generation sequencing (NGS) through whole genome, whole exome, and whole transcriptome approaches has lead to revolutionary studies. A study by Ley et al 213 reporting NGS, first described NGS as an unbiased method discovering cancer-initiating mutations. HBV integration into the host liver genome is considered as a direct way through which HBV causes HCC. Through NGS, three recent reports described HBV integration sites in the host liver genome. Using the whole genome sequencing, Jiang et al 214 found 255 HBV integration sites in only three patients. In the second study by Sung et al, 215 399 integrations sites were identified 75 out of 81 HCC patients. In the third study, Toh et al used 48 patients and, using the deep sequencing-mediated enrichment of HBV genomes, found that HBV integrates significantly in higher frequency in the regulatory regions of the host genes. It was reported that one of the important genes having recurrent HBV integration was TERT gene. 216 A recent study also found important TERT promoter mutations in 60% of HCC patients, and other mutated genes identified were P 53 , CTNNB1, and ARID1 genes. 217 Although not by NGS, but by clonal sequencing, our recent in-vitro study demonstrated that hepatitis B virus can integrate in the host genome immediately after infection, and the same was proved in in vivo study by infecting Wood-chucks with Woodchuck hepatitis virus. 218 Such HBV-host integration junctions possibly have the potential to act as very early molecular biomarkers of HBV related hepatocellular dysregulation. However, the question of whether they can act as a serum biomarker (fused virus-host protein secretion) will need further work and validations. Moreover, it will be interesting to discover, if such virus-host fused, secreted, properly folded proteins indeed play a role in the development of hepatocarcinoma and could be used as a prognostic biomarker or a therapeutic target. Using the whole-exome sequencing, a recent study for the first time identified recurrent alterations in four genes: AR1D1A, RPS6KA3, NFE2L2 and IRF2. In addition in liver tumors G > T transversion were significantly enriched in the non-transcribed DNA strand and highlighted their role in HCC. 219 This study demonstrated alterations in genes responsible for activating the PI3K/Akt/mTOR pathway and an important mutation of mTOR at position S2215Y was reported. 220
Summary
HCC, the neoplastic transformation of the hepatocytes, is one of the leading causes of cancer deaths around the world. People at risk of developing HCC include chronic liver disease patients with hepatitis B or C, obese or diabetic people, and heavy drinkers. HCC is developed as a consequence of chronic liver cirrhosis, where there is a decrease in hepatocyte growth and proliferation, along with scar tissue formation, that provides the platform for neoplastic tumor growth. Current methods of HCC management and treatment are more tumor oriented (chemotherapy using drugs, radiotherapy, surgical methods, such as liver resection and transplantation, and ethanol injection in the tumor cells). However, these methods are more of a palliative approach to HCC, aiming to extend the life span of patients rather than devising a curative approach. Therefore, due to the lack of a proper curative treatment of HCC, it is very important to prevent the onset of HCC or make attempts to detect the disease at a very early stage. The purpose of this review is to present before the readers, scientists, and medical professionals a detailed report of the ongoing research aiming at the discovery of biological tools for the prevention and prognosis of HCC. There are some biomolecules in the tissues and body fluids of humans whose levels change with the development of many abnormal conditions, various disease states, as well as carcinogenesis. These molecules, called biomarkers, are now regarded as important prognostic tools for early diagnosis of HCC. Active research is being conducted both at the basic and clinical levels to accurately detect the molecular targets, for developing drugs and vaccines to cure or prevent HCC. Many classes of biomarkers have been studied and detected in various stages of HCC (early and late), including peptides, glycoproteins, enzymes (soluble biomarkers), and mRNAs (nucleotide biomarkers), and can be obtained from liver tissue and serum of HCC patients. These biomolecules have also shown strong promise as molecular targets for the development of anti-metastatic vaccines or drugs. For example, some biomarkers, such as TAG-72, Golgi-localized phosphoprotein 73 (GP73), enzymes, such as α-1-fucosidase, and HGF, are overexpressed in HCC tissues and indicate poor surviv-ability in patients. There are other markers, such as HCR2 enzyme, the glycoprotein APO-J/clusterin, that are reduced significantly during HCC progression and metastasis. From the start of the new millenium, miRNAs that are small non-coding RNA silencing molecules were recognized to be a new and distinct class of cancer biomarkers, especially in HCC. miRNAs that are effectively stable and easily extractable from tissues, plasma, serum, urine, and feces have shown great potential as prognostic tools and therapeutic targets in HCC.
This review has been documented to discuss the new research going on with an aim to harness the SOS signals of the human body, the biomarkers, to detect early and prevent HCC. The success of this research would bring a new era where not only HCC but also other cancers would no more be a death sentence.
Author Contributions
Wrote first draft of the manuscript: RC. Contributed to the writing of manuscript: RC, NL. Agree with manuscript results and conclusions: RC, NL. Jointly developed the structure and arguments for the paper: RC, NL. Both authors reviewed and approved of the final manuscript.
Footnotes
Abbreviations
Acknowledgments
Authors thank all biomarker investigators and scientists who are directly and indirectly associated with the present review. We have made an effort to accommodate most of the references; however, due to space constraints, all references could not be accommodated.