
Abstract
Objective
The early detection of NSCLC is of importance because it provides chances for better outcomes. The aim of the study was to explore the clinical utility of EGFR and hTERT mRNA expression as markers for diagnosis of NSCLC.
Methods
EGFR and hTERT mRNA were quantified by quantative reverse transcription real time polymerase chain reaction in plasma of 45 non-small cell lung cancer (NSCLC) and 40 chronic obstructive pulmonary disease (COPD) patients, selected by certain spirometric characteristics that made them at high risk of developing lung cancer in future.
Results
The gene expression level of each gene was calculated and given as a relative quantity–-RQ. EGFR gene expression was found in all lung cancer patients. The mean level of expression was RQ = 29.39. hTERT mRNA could be detected in 88% of patients. The mean expression ratio in them was RQ = 17.31. Only 50% of the high risk patients turned to be positive for EGFR. The level of their expression was RQ = 2.09. The plasma levels of hTERT could be detected in 17 (42.5%) patients of the high risk COPD group. Their mean level of expression was RQ = 1.02. A statistically significant difference in EGFR and hTERT mRNA expression could be observed between the two groups of patients–-p = 0.0001.
Conclusion
EGFR and hTERT mRNA are potential markers for lung cancer diagnosis, whose clinical importance should be replicated in a larger cohort of patients.
Introduction
Non small-cell lung cancer is the leading cause of cancer related deaths. Despite the significant advances in both diagnostic and therapeutical approaches, the survival rates of this malignant disease have only slightly improved. The reason for this is that the successful treatment is dependent on the early diagnosis when curative surgical resection could be applied. However current approaches are either too invasive (e.g. bronchoscopy), or there is a lack of sensitivity, (e.g. sputum cytology, chest X-ray) and specificity (e.g. low-dose computer tomography). The routine tumor markers that are used in clinical practice cannot yield satisfactory results as early diagnostic or screening markers. The inadequacy of the standard diagnostic procedures to improve survival rate and the low cost-effectiveness are the reasons for the lack of screening in this type of malignancy.
Advances in gene expression analyses have given the opportunity of using blood-based tests for early identification of non-small cell lung cancer. There are a lot of studies, proving the ability of detecting circulating DNA with tumor related alterations–-oncogene mutations,1,2 microsatellite aberrations,3,4 and aberrant promoter hypermethylation.5,6 However the ability of employing circulating DNA as a diagnostic target needs further elucidation, because of the paucity of gene mutations and the similarity of the genetic aberrations among the different types of cancer.
Another cancer diagnostic approach that has encountered interest is the detection of circulating mRNA.7,8 Using reverse transcriptase polymerase chain reaction techniques, several studies have successfully found mRNA in peripheral blood of lung cancer patients.9–11 The low sensitivity of the method and the use of a single marker for cancer detection, however were not sufficient for clinical applications. To resolve this limitation a highly sensitive approach was introduced into clinical practice that ensures great sensitivity in the quantitative evaluation of gene expression–-real-time polymerase chain reaction.12,13 The analysis of a panel of markers has also gained prerogative in comparison to a single gene expression analysis.14,15
Carcinoembryonic antigen and cytokeratin–-19 are by far the most studied and well known mRNA markers in blood of NSCLC.16–18 Circulating c-met and hnRNP mRNA have also been reported as new biomarkers in non-small cell lung cancer.19,20 Their utility is also investigated in a multimarker diagnostic panel. Mitas et al, 21 also used a three marker panel for the molecular diagnosis of cancer. Though reaching high sensitivity and specificity the utility of these assays for the early lung cancer diagnostics remains elusive. To characterize a marker as a marker for screening of early lung cancer detection, its expression in patients with early stage lung cancer–-I and II and in high risk groups must be evaluated. The selection of markers is also of importance. They should be non-invasively detected in blood, proofs for their expression in early lung cancer should also exist.
Based on these considerations the aim of our study was to describe the expression of EGFR and hTERTin patients with non-small cell lung cancer and in COPD patients with high risk of developing lung cancer.
Material and Methods
Patients and samples
The study was approved by the institutional ethics committee and all patients had signed informed consent. A total of 45 patients diagnosed with non-small cell lung cancer at the Department of Thoracic Surgery during November 2007–-July 2008 participated in the study. Complete staging procedures including chest radiography, bronchoscopy, computed tomography, were carried out to determine precisely the primary tumor–-T, nodal involvement–-N, distant metastases–-M according to the sixth TNM International Staging system for lung cancer. 22 The histology was determined according to WHO classification 2004. 23 Before any tumor manipulations (biopsy, resection etc.) 3 ml peripheral blood were drawn from each patient. None of the patients had received any prior radio- or chemotherapy. Blood samples were taken in tubes containing K3EDTA as anticoagulant. Blood sampling was also done in a consecutive of 40 high risk COPD patients with FEO/FVC < 70%, FEO1 < 75%.
Plasma collection
Peripheral venous blood samples were collected from cancer patients before surgery and from COPD patients into 9 ml K3EDTA blood collection tubes and processed within 20 min to avoid RNA degradation. Plasma was separated by centrifugation at 12 000 g for 15 min at 4 °C to eliminate blood cells and fragments. Aliquots of plasma were stored at -80 °C and thawed once before use.
Total RNA isolation and first complementary DNA synthesis
Total RNA from plasma of NSCLC patients, and COPD patients was extracted by the acid guanidinum thiocyanate-phenol/chloroform method. 24 RNA isolates were then analyzed by using Nanodrop1000. Absorption ratio was detrmined at wavelength 260/280 nm. Only samples pure enough (absorption ratio > 1.8) were used as templates for complementary DNA synthesis. All samples were electrophoretically tested to exclude RNA degradation before reverse transcription was performed.
First strand complementary DNA was synthesized from total RNA (2 μg) with a commerciably available kit High Capacity Reverse Transcription Kit–-2X Reverse Transcription Master Mix (N#4368814, Applied Bisystems). A 20 μ1 reaction contained Multiscribe Reverse transcriptase–-1 μl, RNase Inhibitor-1 μl, 10 × RT hexamers -2 μl, 10 × RT Buffer–-2 μl; 25 × dNTP Mix–-0.8 μl, RNA dissolved in RNase free water-13.2 μl. RNA concentration per reaction -100 ng/μl. The reverse transcription reaction was performed at 37 °C for 2 h.
Reaction preamplification
To concentrate the cDNA it was preamplified by TaqMan PreAmp Master Mix (2X) –25 μl; TaqMan Gene Expression Assay (0.2 × for each of the studied genes); 2.5 μl–-250 ng/μl cDNA diluted to a final volume of 12.5 μl with distilled water. The reaction was initially activated by heating to 95 °C for 10 min. Forty cycles of amplification followed.
Use of Q-PCR
Q-PCR was performed in ABI PRISM 7500 Sequence Detection System (Taqman); Perkin-Elmer Applied Biosystems, Foster City, CA. A single reaction mixture contained 5 μl cDNA, 4 μl H2O, 10 μl TaqMan Universal MasterMix (2X), 1 μl TaqMan Gene Expression (20X). It was carried out in replicates for each patient. TaqMan MGB probes with FAM were used. ROX served as a passive fluorescence control. The analysis was carried out in 96 well plate according to manufacturer's instructions. In each plate No Template Control (NTC) reactions were carried out to confirm the specificity of Q-PCR. TaqMan Universal MasterMix (2x) was used–-N#4369016 for the assay. Commercially available kits with gene specific primers and probes for EGFR, hTERT and beta-actin were applied–-TaqMan Gene Expression (20X)–-Hs 00193306_m1 EGFR (the amplified target corresponds to a tyrosine kinase phoshorylatio site of EGFR and primers are designed in the sequences without mutations), Hs 99999903_m1 ACTB, Hs 00972650_m1 hTERT.
Then PCR amplification was carried out with the following conditions: Initial step for enzyme activation–-2 min/50 °C, 40 cycles of denaturation–-15 s/95 °C, annealing and extension–-60 s/60 °C. PCR products were quantified by measuring the intensity of fluorescence at the end of the amplification cycle. The fluorescence intensity of each mRNA was normalized to β-actin.
Data analysis
The results of the quantitative PCR were generated using the software version 1.3. The threshold cycle in each subject was received on the basis of two independent experiments. Relative gene expression analysis was applied. The expression ratio (relative quantity–-RQ) was calculated by means of the Livak's formula for delta delta Ct. 25
Statistical analysis
All data were analysed with the Statistical Package for the Social Sciences version 13.0. The comparison between EGFR and hTERT gene expression in NSCLC patients and COPD patients was done with Mann-Whitney. A p-value <0.05 was considered of statistical significance.
Results
Clinicopathological features of NSCLC patients
Of the 45 NSCLC patients thirty-seven (82%) were males and eight (18%) were females, with a mean age of 59.8 years (range 43–75). All were active smokers with a mean number of packyears–-28.1. Regarding the histological types fourteen (31%) had adenocarcinomas and thirty-one (69%) had squamous cell carcinoma. Five (11%) were subsequently diagnosed with T1 disease, twenty (44%) with T2, fourteen (31%) with T3 and six (14%) with T4. Regarding the nodal status–-twenty-three (51%) were diagnosed with N0 disease, six (13%) with N1, fourteen (31%) with N2 and two (5%) with N3. None of the patients had distant metastases upon diagnosis. Regarding the overall stage–-sitxteen (35%) had stage I, thirteen (29%) were at stage II, sixteen (36%) at stage III.
The COPD group of patients consisted of thirty-seven men and three women with a mean age–-61.4 (range 56–74). All were smokers with a mean number of packyears–-27.3. The diagnosis of COPD was verified spirometrically and the forced expiratory outflow–-FEO1/forced vital capacity (FVC) ratio of less than 70% was used as a criteria for participation. According to the grade of obstruction (FEO1), the group of COPD patients consisted of–-17 patients with FEO1 < 80%, 12 patients with FEO1 between 80%-50%, 11 patients with FEO1 < 50%.
Correlations between expression of EGFR and hTERT mRNA markers in plasma and patients’ clinicopathological characteristics
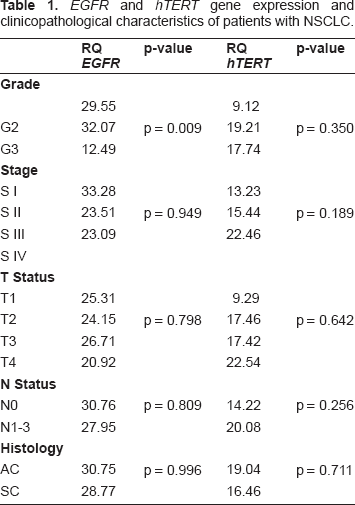
Regarding the whole group of patients, no significant correlation could be found between expression of mRNA markers in plasma and patients’ demographic and clinicopathological features such as gender and histological type of cancer. The expression of EGFR however seemed to correlate with the grade of differentiation–-p = 0.009. In addition, expression of both EGFR and hTERT in plasma was not significantly associated with the T, N, M, factor and the overall stage of the disease–-Table 1.
EGFR and hTERT gene expression and clinicopathological characteristics of patients with NSCLC.
Plasma expression of EGFR and hTERT mRNA in NSCLC and high risk group
EGFR mRNA could be detected in all patients with NSCLC. The mean level of expression was RQ = 29.39; RQmin = 0.95; RQmax = 50.03. Only 50% of the high risk patients turned to be positive for EGFR. The level of their expression was RQ = 2.09; RQmin = 0; RQmax = 21.07. hTERT mRNA could be detected in 88% of the patients with lung cancer–-40/45. The mean expression ratio in them was RQ = 17.31; RQmin = 5.12; RQmax = 27.45. The plasma levels of hTERT could be detected in 17 (42.5%) patients of the high risk COPD group. Their mean level of expression was RQ = 1.02; RQmin = 0; RQmax = 12.84–-Figure 1.
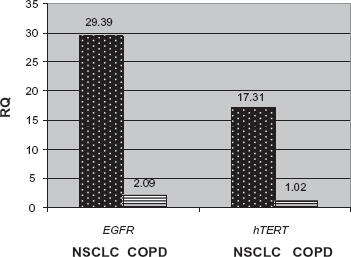
Mean expression levels of EGFR and hTERT in NSCLC and COPD patients presents the mean levels of expression of each gene in the two groups of patients–-NSCLC and COPD. RQ-relative quantity is the level of expression of the genes calculated by the already mentioned method of delta-delta Ct. It is a numerical equilavent of the level of gene expression.
Discussion
The use of circulating nucleic acid in the peripheral blood is increasingly regarded as a relatively noninvasive simple and reliable method for cancer diagnosis and follow up.26–28 Despite the great number of reports exploiting qPCR based techniques to find cancer-specific DNA aberrations in plasma or serum, their clinical applicaton is still obscure. Although results were promising it is becoming clearer that DNA based methods have some limitations such as low sensitivity, because of the paucity of the mutation, low specificity due to the common characteristics shared among malignancies and complexity of the technical detection of the genetic aberrations. 27
RNA based approaches in contrast are more sensitive as the detection rate of mRNA in blood ranges between 30%–60%. Despite of the advances in molecular diagnostics of cancer, none of the current mRNA based assays have yet achieved acceptable sensitivity for clinical cancer diagnosis.9–11
For the first time a combined detection assay in NSCLC patients was performed by Fleischhacker et al. 29 He detected hnRNPB1 mRNA and HER2 mRNA in blood in all of the eighteen patients, he investigated. Miura et al, 30 applied a multimarker panel in a large cohort of patients–-112. They found that hTERT is a useful marker for lung cancer diagnosis and staging. Sher et al, 31 carried out a combined assay of four marker genes to detect circulating cancer cells in NSCLC. An overall positive detection in 72% of patients was detected Sheu et al, 32 studied the expression of CEA, CK-19 and c-met in peripheral blood of 69 NSCLC patients. This multimarker panel gave a sensitivity of 85.5% and specificity of 85% respectively. Although providing a high detection rate in early stage cancer–-80% of T1, the study was unable in characterizing the early diagnostic potential of the markers, because the percentage of patients with early stage lung cancer–-I and II was 34.7% of the whole cohort. In addition there was not a high risk population to provide evidence for the evaluation of the effectiveness in detecting undiagnosed NSCLC undiscovered in individuals.
To the best of our knowledge this is the first study, whose design provides the opportunity to evaluate the diagnostic potential of biomarkers as well as their usefulness as screening markers in high risk group patients. The choice of the two markers was done regarding to their role in the initial steps in lung cancerogenesis. 33 The screening characteristics of the panel were performed in a COPD group of patients with certain spirometric characteristics. According to Purdue et al, 34 COPD patients with FEO/FVC < 70%, FEO1 < 75%, had a higher relative risk for lung cancer development in comparison to the general population.
Applying a preamplification assay we generated expression of both of the genes in almost all patients’ plasma. The preamplification was performed with cDNA and gene specific primers. It allowed concentration of the genes of interest and augmented the sensitivity of the real-time assay. The plasma expression of EGFR was detected in all patients. hTERT mRNA was observed in 88% of the investigated subjects. The mean level of expression of EGFR in the NSCLC group was RQ = 29.39. In comparison in the COPD patients only 50% showed expression for EGFR RQ = 2.09. hTERT mRNA gene expression level was–-RQ = 17.31 in NSCLC patients; in COPD patients hTERT mRNA expression was detected in 42.5% of the patients. Their mean RQ = 1.02. Comparing the mean values of the gene expression of EGFR and hTERT in the two groups, a statistically significant difference could be observed–-p < 0.0001. Despite of the fact that patients with advanced stage of the disease participated in the study (sixteen–-36% at stage III)–-all patients with early stage lung cancer showed expression of both of the genes in plasma.
These findings are consistent with the results of Miura et al, 30 who ran a real-time PCR with EGFR and hTERT using absolute quantative analysis. In contrast to our design their group of cancer patients included SCLC. The control group was entirely of healthy volunteers. They were able to define a cut-off copy number of EGFR and hTERT mRNA performing ROC analysis. The sensitivity and specificity in lung cancer diagnosis were 89.0% and 72.7% for hTERT mRNA, and 71.3% and 80.0% for EGFR mRNA, respectively.
Although we were unable to perform an absolute gene expression analysis, the preliminary data of our study implies the diagnostic potential of EGFR and hTERT as candidate markers for lung cancer detection among high risk smokers. A larger cohort of early lung cancer and high risk patients should be investigated for the validation of our findings. An absolute gene expression analysis is required to find the threshold value of gene copy mRNA and estimate the sensitivity and specificity of the panel of markers.
Conclusion
The expression of EGFR mRNA and hTERT mRNA in plasma of non-small cell lung cancer patients provides a potential tool for molecular diagnosis of NSCLC among high risk groups of patients.
Disclosures
The authors report no conflicts of interest.