
Abstract
Introduction
Breast cancer is the most common cancer among Egyptian women. We report the unique assessment of hope and social support outcomes of women with breast cancer after mastectomy in Egyptian community.
Patients and methods
Between July 2009 and June 2010, three hundred and one women with newly diagnosed breast cancer joined this study. Socio-demographic data including patient's age, level of education, occupation, social status, and residence were collected by means of structured interviews based on special questionnaires. These questionnaires were designed to measure hope and social support.
Results
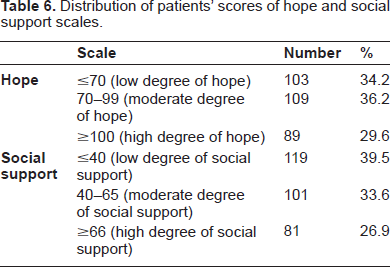
Age ranged from 21 to 88 years (median = 45.8 years and SD ± 13.3). A low degree of hope was reported in 103 patients (34.2%), a moderate degree in 109 patients (36.2%), and a high degree in 89 patients (29.6%). A low degree of social support was reported in 119 patients (39.5%), a moderate degree in 101 patients (33.6%), and a high degree in 81 patients (26.9%).
Conclusions
Social support is related to many psychological factors, which can be quantitatively analyzed and it can predict hope. However, there were no significant differences between the socio-demographic variables (age, educational levels, residence and martial status) and social support, hope, and their sub-components among Egyptian women with breast cancer.
Introduction
In Egypt, as in many other parts of the world, breast cancer is the most common type of cancer: it accounts for approximately 38% of reported malignancies among Egyptian women. 1
The social environment may represent a protective shield to patients from the harmful effects of discomfort associated with cancer. It has been found that the structural forms of the individual's social relations such as relation dimensions and the functional forms such as emotional support may be associated with rates of death and life in cancer patients. 2
Social support plays an important role in reducing the pressure and improving health. Cancer patients who lack social support may be more pessimistic and desperate as they are constantly looking for support from others. 3
Few studies have been conducted in Egypt to assess the outcomes of social support and hope among women with breast cancer after mastectomy. This study aims to investigate the relations between social support and hope among Egyptian women with breast cancer using quantitative measures, and to determine whether social support and hope vary according to socio-demographic variables or not.
Patients and Methods
This is a prospective study carried out in The Oncology Center, Mansoura University between July 2009 and June 2010. After giving their verbal and written consents, three hundred and one women with newly diagnosed breast cancer participated in this study. They were recruited postoperatively while still in the surgery department. Fifty-one women underwent sparing mastectomy with immediate autologous breast reconstruction while the others underwent modified radical mastectomy. Socio-demographic data including each patient's age, level of education, occupation, social status, and residence, were collected during structured interviews. These interviews were based on special questionnaires designed to measure social support and hope.
The hope questionnaire
The Hope Measurement Questionnaire (Table 1) is composed of 51 items describing five domains of hope: physical, emotional, spiritual, medical, and occupational. The items measuring these domains were randomly distributed throughout the questionnaire to achieve balance, social desirability, and patient satisfaction (Table 2).
Hope measurement questionnaire.

Distribution of items of Hope domains throughout The Hope Questionnaire.
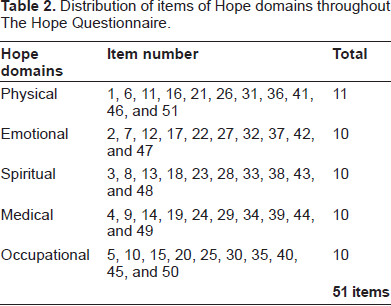
The items included were extracted from psychological frameworks and previous studies, and then modified to be logical, non-suggestive, non-duplicative in meaning, appropriate for the sample of the study, and suitable for patients’ culture and for the research's objectives.4–8
Each item was weighed on a scale of 3 points (1 = Disagree, 2 = Not sure, 3 = I agree). The total score ranges from 51 to 153. This score indicates the range of hope: ≤70 = a high degree of despair, 70–99 = moderate degree of hope, and ≥ 100 = a high degree of hope and desire in life.
The social support questionnaire
The Social Support Measurement Questionnaire (Table 3) consists of 33 items including four domains; psychological, material, medical, and social. Table 4 shows the random distribution of these items. The items included in the questionnaire were extracted from some previous studies9–14 and were amended in terms of language to be appropriate to the research sample and objectives.
The Social Support Questionnaire.

Distribution of items of Social Support domains throughout the Social Support Questionnaire.

Each item was weighed on a scale of 3 points (1 = Disagree, 2 = Not sure, 3 = I agree). The total score ranges from 33 to 99. This score indicates the range of social support: ≤40 = a low degree of social support, 40–65 = moderate degree of social support, and ≥66 = a high degree of social support dimensions.
Research hypothesis
There is a relation between social support and hope among patients with breast cancer.
Social support of patients with breast cancer is linked to several psychological factors, which can be quantitatively analyzed.
Social support can predict hope in women with breast cancer.
Both social support and hope vary in patients with breast cancer according to the socio-demographic variables.
Results and Statistical Analysis
Three hundred and one women with breast carcinoma were included in this study. They represent various socio-demographic levels of rural Egypt. Their ages ranged from 21 to 88 years (median = 45.8 years and SD ± 13.3). Table 5 shows the socio-demographic features while Table 6 shows the distribution of patients’ scores on both Hope and Social Support scales.
Socio-demographic features.
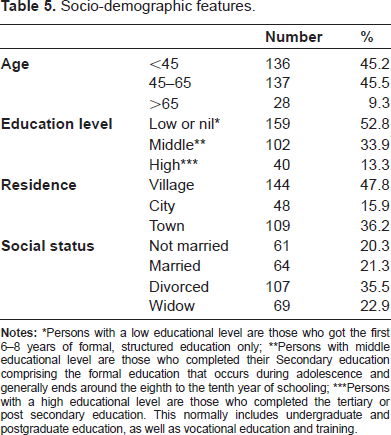
Persons with a low educational level are those who got the first 6–8 years of formal, structured education only;
Persons with middle educational level are those who completed their Secondary education comprising the formal education that occurs during adolescence and generally ends around the eighth to the tenth year of schooling;
Persons with a high educational level are those who completed the tertiary or post secondary education. This normally includes undergraduate and postgraduate education, as well as vocational education and training.
Distribution of patients’ scores of hope and social support scales.
The first assumption
There is a relation between social support and hope among patients with breast cancer.
To test the validity of this hypothesis, the data collected were analyzed in two ways:
First
The bilateral correlation coefficient of the participants’ scores on the measurements of social support and hope was (43.0), which represents a positive and statistically significant value at (0.01).
Second
After controlling the demographic variables of age, education, marital status, and residence, the partial correlation coefficient of the participants’ (N = 301) on the measurements of social support and hope was (44.0), which represents a positive and statistically significant value (0.01).
The second assumption
Social support of patients with breast cancer is linked to several psychological factors, which can be quantitatively analyzed.
To test the validity of this hypothesis, factor analysis (the principal component method) as well as varimax rotation method was applied to participants’ responses to the items of the questionnaires used in the study. Table 7 shows the data resulting from factor analysis after rotation. Saturation was calculated and found to be (3.0) indicating the presence of the three following factors:
Rotated component matrix.

The first factor (the spiritual domain of hope)
It includes a group of seven variables of a total of eleven variables representing the domains of the study. The data obtained indicate the strength of this factor which can be regarded as the most highly saturated and correlated variable. The saturation degree of this domain was (3.32) followed by that of body domain (0.883), the emotional component (0.882), the psychological domain of social support (0.875), the material domain (0.861), the total degree of social support (0.568), and then the total degree of hope (0.565).
The second factor
This factor included eight variables of the study. The saturation values of this factor ranged between (0.316) for the medical domain of social support, (7.97) for the social domain of social support. This makes it the most saturated variable. The saturation value of social support was (4.91) and that of the body domain of hope was (3.76). The occupational domain had a saturation value of (0.834) while the total degree of hope had a saturation value of (0.797), and the medical domain of hope a value of (0.778). The saturation value of the spiritual domain was comparatively low (0.608).
The third factor
This factor included five variables: the psychological domain of social support (8.379), the emotional domain of hope (5.15), followed by the social domain of social support (0.911) as well as the medical domain of social support (0.854), and finally the total degree of social support (0.795).
The third assumption
Social supports can predict hope for patients with breast cancer.
The regression coefficient was used to test the validity of this hypothesis. The results indicated that the t value mounted to (8.263) thus indicating that psychological support predicts hope. This means that social support can predict hope for patients with breast cancer. Table 8 illustrates the ability of social support to predict hope in patients with breast cancer.
Ability of Social Support to predict hope.

The fourth assumption
Both social support and hope vary in patients with breast cancer according to the socio-demographic variables.
The validity of this hypothesis was tested by applying the Anova one-way analysis of variance (contrast) test to participants’ responses to the measurements of social support, hope and their sub-components (domains). The results were as follows:
Age
Social support, hope and their sub-components do not vary among patients with cancer breast according to their age (Table 9).
Differences between Social Support, Hope and their domains according to age.

Educational level
Table 10 shows the differences between social support, hope and their domains in relation to the educational level. There are no statistically significant differences between the different educational levels and hope or social support with the exception of the social domain of psychosocial support which has a statistically significant difference at (0.01). Using Scheffe Test to identify which groups have differences, it was found that there were significant differences between women who had nil or low education and women who had a high level to the advantage of the first group who had an average grade of (15.6). The highly educated group, on the other hand, had an average grade of (13.7).
Differences between Social Support, Hope and their domains according to the Educational level.

Residence
Table 11 shows the differences between participants’ scores on The Social Support and Hope questionnaires together with their domains in relation to residence. There were no statistically significant differences between residence and the total score of hope including its emotional, medical, occupational domains. However, there were statistically significant differences between the physical and the spiritual domains of hope and residence at (0.01) level of significance. Using Scheffe Test to identify which groups had differences, it was found that differences in the physical domain of hope were between city residents who had an average grade of (13.9) and the village residents who had an average grade of (11.7). There were also differences in the average grades between town residents (13.5) and village residents (11.7). In regards to the spiritual component, there were differences between town and village as well as between city and village towards village with an average of (17.4), (14.7), and (15.4) respectively.
Differences between Social support, Hope and their domains according to Residence.

Results related to social support also indicate that there are no statistically significant differences between the different places of residence and the total score of social support together with its components with the exception of the material component as there were significant differences in this variable at (0.05) between town and village towards town where the average grades were (9.3) against (8.2) for village.
Marital status
Table 12 shows the differences between social support, hope and their domains in relation to marital status. There were no statistically significant differences between marital status and the total degree of hope with its domains or of social support and its components. However there were statistically significant differences between the components of hope criterion and marital status at (0.01) level. Using Scheffe test to identify which groups have differences, it was found that there were differences between married women, divorcees and widows: the average grades were (15), (17.3), and (17.4) respectively.
Differences between Social support, Hope and their domains according to the Martial status.

Discussion
When women are subjected to psychological stress or emotions they cannot face either because of the strength of situation or because of their personalities, they become vulnerable to many diseases including cancer. At present, women are subjected to too much pressure because of the burden of working in different fields in addition to the commitments of their roles as mothers and housewives. These pressures have naturally affected women's physical structure and exposing them to disease and reducing their sense of hope. This reduced feeling of hope in life is affected by many factors such as: family, friends (social support) and religious beliefs which all are important in giving the individual the feeling of hope.15–17
Dekeyser et al. (1998) conducted a prospective, descriptive and relational study which aimed to investigate the relationship between psychological stress and the pressures that women face as well as the effects of hope loss (despair) on the function of the immune system. The study sample included (n = 35) women, six of them were suffering from malignant tumors and 29 of them did not suffer from any organic disease. The variables of the study were psychological pressure, psychological stress symptoms, and hope. Hope was measured by a scale designed to suit the sample of the study, psychological pressure by a short list of symptoms and the function of the immune system by the level of cytokine in the blood serum. The results of the study showed that there was a strong influence of the process of cancer diagnosis on psychological stress, hopelessness, and the loss of hope: these factors had negative effects on the function of the immune system. It was also found that psychological pressure experienced by women in their lives before the diagnosis of breast cancer was of a very strong effect causing the collapse of the immune system and making women more vulnerable to breast cancer. The immune system of women, who were not subjected to any organic disease, has the ability to cope with any disease through the increase in white blood cells. They usually cope with psychological pressures because of the immune system activity and its good performance. 18
Social support may even affect the outcome of breast cancer therapy; Spiegel et al. (1989) published what would become a landmark study showing that women with metastatic breast cancer who participated in an expressive supportive group therapy intervention lived about twice as long as women who had a similar condition. 19
The comprehensive understanding of patients’ healthy psychological reactions towards breast cancer is a necessary matter to determine standards of care and treatment vectors for women with breast cancer who are psychologically healthy and others who suffer from psychological disorders which may significantly delay or complicate treatment. 20
Some studies confirmed and agreed with the results of the current study as to the presence of a strong relationship between social support together with its dimensions and hope and its domains.21–23
Many studies confirmed that hope varies according to demographic variables like education, age, and the patient's previous experience of cancer.24–33 These studies have stated that education has a role in the development of a sense of hope 34 and demonstrated that whenever the individual is educationally developed, the feeling and awareness of hope increases. 35
However, in this study, social support, hope and their sub-components do not vary among Egyptian women with breast cancer according to their educational levels. This may be attributed to many interacting factors: some of these factors are related to habits and traditions which are the main constituents of culture among Egyptians especially women regardless of their educational levels. Other factors are related to the quality of education they receive.
Some previous studies concluded that patients who have a rural cultural background; live far away from pollution, congestion; and whose lifestyle is characterized by religiosity and spirituality, will feel hope more than their peers who live in city. 36 The present study, however, showed that there were no statistically significant differences between the different places of residence and the total degree of hope, social support, and their domains. This may be attributed to the unplanned urbanization of rural areas in Egypt which resulted in the migration of large rural population to urban towns during the last decades. This has, in turn, resulted in a mix of many socio-demographic features between Egyptian villages, cities and towns.
Apparently, hope correlation with demographic variables is not absolute: variability and differences in these variables are not a certainty and the issue is still controversial. The sense of hope is not related to the educational level since it represents a response to a certain situation or to a stimulant that the individual experienced. 37
The type of treatment has no effect on the sense of hope. Patients particularly those suffering from breast cancer often feel desperate because of the extreme seriousness of this disease and the sterility of its treatment. 38 Other studies also concluded that subculture and age have no effect on the sense of hope.39,40
In regards to marital status in the present study, it was found out that there were no statistically significant differences between the marital status and the total degree of hope and its domains or between marital status and social support and its domains. This may be explained by the similarity of problems among members of all groups as reflected in the questionnaires of hope and social support, eg, delayed age of marriage together with its attendant concern for the future; family problems and the absence of husbands either due to travel or overtime work or lack of husband support; divorcing along with the Egyptian Society's melancholy view of divorced women; and the widowhood together with the concomitant burden of having additional responsibilities towards raising children in the absence of a comprehensive system of social solidarity.
The present study proved that both social support and hope do not vary in Egyptian patients with breast cancer according to any of the socio-demographic variables investigated.
Conclusions
Social support is related to many psychological factors, which can be quantitatively analyzed. These factors represent the domains or dimensions of hope; therefore, there is a strong relation between social support and hope. In addition, social support can predict hope among Egyptian women with breast cancer, but there are no significant differences between the socio-demographic variables (age, educational levels, residence and martial status) and social support, hope and their sub-components.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgment
The authors gratefully acknowledge the contribution of Dr. Osama El-Damshety.