
Abstract
Background
Our original paper, published in 1992, reported a median overall survival after first relapse in breast cancer of 26 months. The current retrospective review concentrates more specifically on patients with first systemic relapse, recognizing that subsets of patients with local recurrence are potentially curable.
Methods
Records of 5,168 patients from a largely breast-cancer-specific oncology practice were reviewed to identify breast cancer patients with their first relapse between 1996 and 2006 after primary treatment. There were 189 patients diagnosed with metastatic disease within 2 months of being seen by our therapeutic team and 101 patients diagnosed with metastatic disease greater than 2 months. The patients were divided in order to account for lead-time bias than could potentially confound the analysis of the latter 101 patients.
Results
Median survival for our primary study population of 189 patients was 33 months. As expected, the median survival from first systemic relapse (MSFSR) for the 101 patients excluded because of the potential for lead-time bias was better at 46 months. Factors influencing prognosis included estrogen receptor (ER) status, disease-free interval (DFI), and dominant site of metastasis. Compared with our original series, even with elimination of local-regional recurrences in our present series, the median survival from first relapse has improved by 7 months over the past two decades.
Conclusion
The new benchmark for MSFSR approaches 3 years.
Keywords
Introduction
Breast cancer is the most prevalent cancer among women in the United States, and remains the second leading cause of cancer-related mortality. In 2013, approximately 232,340 women were diagnosed, and 39,620 women died of breast cancer. 1 Although most patients with early stage disease will be cured, the 10-year risk of distant recurrence at 5 and 10 years is approximately 14% and 36%, respectively.2,3 The prognosis of patients with metastatic breast cancer (mBC) is rather heterogeneous, ranging from several months to many years, depending on numerous factors including original tumor stage (tumor size and number of metastatic lymph nodes involved), age at relapse, estrogen receptor (ER) status, human epidermal growth factor receptor 2 (HER2) receptor status, sites and number of sites of relapse, disease-free interval (DFI), and prior exposure to adjuvant or neo-adjuvant chemotherapy.4–24
Our original paper, published over 20 years ago, reported a median survival after first relapse (MSFR) of 26 months (range: 15–90 months) among a population of patients diagnosed with relapse between 1976 and 1982 treated at the University of Miami. 4 In the intervening time since the initial publication, there have been significant advances in the treatment of mBC, including new surgical and radiation techniques, and the addition of novel systemic agents, including aromatase inhibitors (AI), taxanes, and the advent of HER2 targeted agents. One of the critical elements of our original paper was accounting for lead-time bias. Lead-time bias has been discussed extensively as a potential confounding variable in the reduction of overall mortality of newly diagnosed breast cancer due to the potential impact of early detection through screening. 1 Our original publication would have overestimated median survival results if we had not adjusted for lead-time bias. 4
The purpose of this study was to define a new benchmark for survival in patients with systemic breast cancer excluding the potentially curable subset of loco-regional relapse. Most still cite a median survival for metastatic breast cancer of approximately 2 years.2,13 However, there remains significant controversy regarding this number.6,8,18,25 The current retrospective review was undertaken in an attempt to clarify the median survival for those subsets of metastatic breast cancer that are considered “incurable”.
Patients and Methods
The records of 5,168 patients with breast cancer from a large breast cancer oncology practice from 1986 to 2011 were retrospectively reviewed to identify patients with known, accurate dates of first distant relapse after primary therapy with curative intent. Because of the retrospective nature of the study and the use of deidentified data, the requirement for ethics committee approval was waived by the University of Miami IRB. The time period chosen for primary analysis was 1996–2006 to provide an approximate two-decade span from the previous publication.
4
Since one of the authors of this manuscript (CLV) helped establish the philosophical therapeutic strategies in the older series and the present series, this potential confounding variable was also likely mitigated. Excluded patients included men, patients with a primary diagnosis other than breast cancer, patients relapsing before 1996 or after 2006, patients rendered clinically and continuously disease-free after primary local-regional therapy, onetime consultations, and patients who had most care outside our clinic. In addition, patients with
In the present analysis, the date of first relapse was the date of unequivocal confirmation of systemic recurrent breast cancer. The interval from the date of primary surgery to diagnosis of first recurrent systemic metastasis was considered the DFI. Biomarkers were performed in a wide variety of clinical laboratories, and quality control for ER and progesterone receptor could not be readily verified for every subject. Various adjuvant therapies were used at the time of initial diagnosis of primary breast cancer, including anti-hormonal therapies for women with ER-positive tumors generally given after conclusion of cytotoxic chemotherapy and/or radiation when either or both of those two cytotoxic modalities were employed. Standard combination and sequential adjuvant and neo-adjuvant chemotherapeutic regimens were used when indicated, generally including some of the following: cyclophosphamide, methotrexate, 5-fluorouracil, doxorubicin, paclitaxel, and docetaxel. Trastuzumab was included in adjuvant regimens in women with HER2-positive tumors after 2006.
At the time of first relapse, patients generally had a complete physical examination and ancillary lab tests, which generally included complete blood count (CBC), complete metabolic panel (CMP), carcinoembryonic antigen (CEA), cancer antigen (CA) 15–3, bone scans, confirmatory bone radiographs, and computed tomography (CT) scans. Positron emission tomography (PET) scans, biopsies of metastatic sites when feasible, and magnetic resonance imaging (MRI) scans were performed when appropriate.
During the time period studied, treatment strategies for patients with hormone receptor-positive recurrent disease were conservative and hormonally oriented whenever possible. Cytotoxic chemotherapy generally was reserved for hepatic metastases, “visceral crisis”, or ER-positive patients who did not respond to at least one hormonal treatment. Patients with indolent and/or asymptomatic clinical features frequently received hormonal agents initially and for as long as the disease remained responsive to estrogen blockade.
Recognition of the potential effects of lead-time bias was an important feature of our analysis and was based on the experience gained from our first publication on this topic. 4 Our final study population consisted of patients who experienced their first relapse between January 15, 1996 and December 1, 2006, and whose date of first relapse occurred no more than 60 days before first contact with our medical center. Essentially, these patients experienced a relapse at the initial visit to our institution or slightly later. Patients who had a relapse more than 2 months before the first contact with our institution were analyzed separately, as this group was potentially confounded by lead-time bias.
The literature search was performed using PubMed.gov using the search terms “ breast cancer”, “relapse,” and “survival”. Studies included in our literature search were published between 1999 and 2013, had at least 50 patients, and included both retrospective and prospective cohorts.
Statistical methods
In our first publication,
4
patients relapsing greater than 2 months prior to being seen by our group were found to have a significantly improved MSFR. Because we suspected the result was due, in part, to lead-time bias, we separated those patients in the present series (
Results
From 1986 to 2011, 5,168 patients were seen in this oncology practice, and >95% had breast cancer. Of the patients who met our inclusion criteria (
Baseline patient characteristics.

Chi-square analysis-study population versus patients excluded due to potential lead-time bias.
Two-sided
The primary endpoint of this study was to determine the MSFSR using an analytic design similar to that of our metastatic disease population approximately two decades earlier. 4 The MSFSR for our primary study population of 189 patients was 33 (29.2–36.8) months (39 months for ER positive and 23 months for ER negative). The MSFSR for the 101 patients possibly confounded by lead-time bias was longer, at 46 (38.5–53.5) months (49 months for ER positive and 35 months for ER negative). Allowing for different therapeutic advances during the 10 years of the study, the MSFSR was further analyzed by 5-year intervals in Table 2, but changes in these two time intervals were minimal.
Univariate and multivariate analysis.

Log-rank.
oportional hazards regression significance of variable.
Significantly more patients in our study cohort, relative to the patients excluded due to possible lead-time bias, received prior adjuvant chemotherapy (Table 1). There were no significant differences between the study population and the excluded patients with regards to DFI, ER status, dominant site of metastasis, or any other variable. After initial univariate screening of the whole group, a Cox proportional hazards regression analysis was performed using 10 potential prognostic variables (Table 2). The following variables were identified as being associated with a significantly worse prognosis on regression analysis: HER2 negativity, ER negativity, DFI less than 24 months, greater number of metastatic sites, and age >50. The year of metastasis and site of dominant metastasis did not contribute significantly to the multivariate model in the presence of the other factors. Although patients who had received prior adjuvant chemotherapy, radiation therapy, or hormonal therapy appeared to do worse than those who did not, these patient subgroups tended to have more advanced (node-positive) disease at initial diagnosis. Importantly, for comparison with other series from the literature, 72% of our series received some form of adjuvant chemotherapy.
Based on the results from our Cox proportional hazards regression analysis, the expected MSFSR was calculated for patients with different constellations of the major prognostic variables similar to the analysis done in our previous publication (4; Table 3). These variables roughly define a spectrum of prognostic subgroups. When this analysis was performed, 150 of 189 patients (79.4%) in our study population had died. One-hundred and fifty-three (80.1%) of the patients were alive at 1 year, 73 (38.6%) at 3 years, 35 (18.5%) at 5 years, and 9 (4.7%) at 10 years. In our original publication (Table 4), the heterogeneity of survival was greater than in our current series. 4 The decreased heterogeneity in observed survival is likely due to the exclusion of patients with local-regional recurrences in our present series, since those patients tend to have a more favorable prognosis. Interestingly, the patients with the longest survivals were HER2-positive cases, with 14/16 having dual ER and HER2 positivity.
Median overall survival time from first systemic relapse: variations as a function of major prognostic determinants.

Total number of patients with available data for all prognostic determinants.
Review of literature.
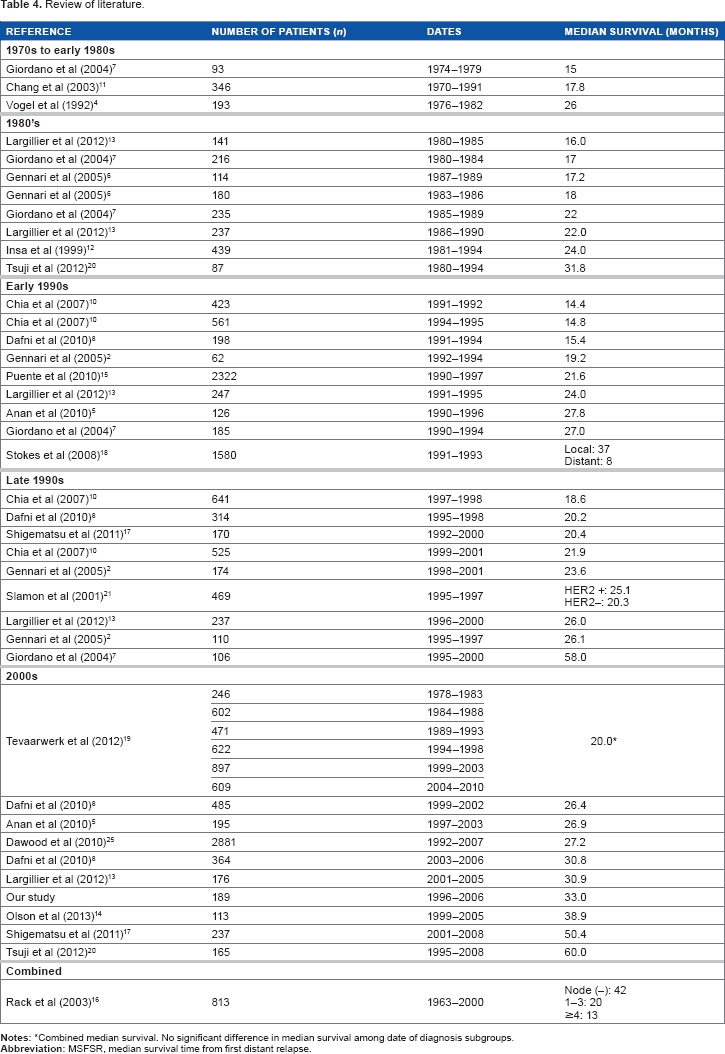
Combined median survival. No significant difference in median survival among date of diagnosis subgroups.
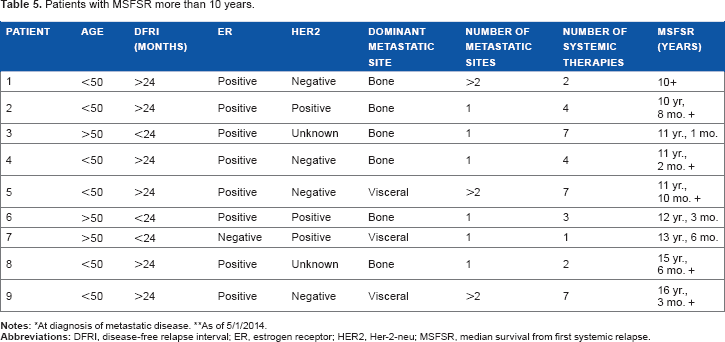
We also explored the number of patients in our series that had lived for more than 10 years (Table 5). Approximately 4.7% of our overall population lived for >10 years, and, as expected, was largely comprised of patients with bone-dominant disease.
Patients with MSFSR more than 10 years.
Discussion
Since our last report, most studies in the literature looking at clinical outcomes in mBC patients have demonstrated an improved median overall survival (OS) over time. In our last report, looking at recurrent breast cancer patients from 1976 to 1982, we found an MSFR of 26 months, 4 a figure that was found to be consistent with other reports at the time.7,11,25 Comparing our current series with our last report, the MSFSR over time has increased to 33 months, ie, 7 months longer than in the previous study. This increase is likely an underestimate of the improvement because the current MSFSR data excludes the favorable soft-tissue subgroups included in the original MSFR dataset. This improvement is fairly consistent with most other studies of the late 1990s through the early 2000s.2,7,8,10,13,25
Our current study population, when compared to that of our original series, 4 had younger patients (age <50: 49.2% vs 29.5%) and a greater proportion of ER-positive tumors (70.6 vs 41.4%). Additionally, more patients had a long DFI (>2 years: 74.6% vs 46.1%) but were more likely to have visceral metastases (54.5% vs 38.9%). Our current study population may have had an improved DFI, compared with our earlier series, due to the improvement in adjuvant therapies over this time period. There were differences in ER positivity rates between current and prior retrospective series, but this is likely secondary to a high proportion of borderline and unknown ER patients in our earlier series. The high proportion of patients with visceral metastases in our current population relative to that of our earlier series is likely influenced by the exclusion of patients with local-regional recurrences in the present study. Patients with local-regional recurrences are well known to have a favorable long-term prognosis relative to other sites of distant metastasis, with many patients likely being potentially curable. 26 – 28
Our previous study did not incorporate the number of metastatic sites, which is a known prognostic indicator, and was found to have prognostic value in our current study. One of the other major differences between our two series was the incorporation of HER2 testing and availability of HER2-targeted therapies, eg, trastuzumab, in our current series. HER2-targeted therapies have completely transformed the natural history of HER2-positive mBC, and this is illustrated by the improvement in a MSFSR of 54 months for ER+/HER2+ tumors compared to those other subtypes. As was seen in our previous series, although to a lesser extent, patients who received prior adjuvant chemo with or without radiation therapy had a worse median OS than those that did not. This is likely explained by patients with higher recurrence risks generally receiving adjuvant chemotherapy and possibly radiotherapy.
As was the case in our previous series, 4 the patients not included in our primary study group who were excluded because of the possibility of lead-time bias had a longer MSFSR compared with the primary study group. This finding emphasizes the importance of considering features contributing to lead-time bias as a confounding variable when analyzing other publications. In both our previous and current studies, ER status and DFI were found to be important prognostic determinants, attesting to the consistent value of these variables in prognostication in recurrent breast cancer patients.
The issue of prior adjuvant chemotherapy becomes very important when one considers two of the most important prominent outliers in our literature review. Both the trial of Tevaarwerk et al 19 and the most recent cohort in the series presented by Giordano from the MD Anderson Cancer Center (MDACC) 7 studied patients who had all received adjuvant chemotherapy. In our series, 72% of patients had received adjuvant chemotherapy. The second outlier is the 58-month MSFR in the MDACC most recent cohort, 7 which included patients with local-regional relapse and had a median DFI of 6–8 years, a favorable characteristic that was more than double the DFI of any of their prior cohorts.
Both our literature review (Table 4) and the review by Stokes et al 18 point to the significant heterogeneity and variability in median OS between published series. Interestingly, both articles specifically analyzing distant recurrence including Stokes et al 18 (MSFSR = 8 months) and Tevaarwerk et al 19 (MSFSR = 20 months) are significantly less encouraging than are our own data (33 months). One possible explanation is that, while our data were generated from within a breast-cancer-specific practice, Stokes et al's 18 data were generated from an older population of Medicare patients in the SEER database. The low MSFSR could be explained by a higher risk of death from other causes in this older population without the management of metastatic disease, likely delivered by a highly varied group of oncologic specialists rather than breast-specific oncologists. Likewise, while patients in Tevaarwerk et al's study were treated by highly competent ECOG physicians, patterns of metastatic breast cancer care after adjuvant protocol therapy may well have differed significantly among practices. 19
All trials identified ER positivity and longer DFI as favorable prognostic variables as did we. All studies identified predominant metastatic site as the third important variable as we had identified in our 1992 publication. 4 While our current series specifically excluded soft-tissue disease from analysis, all other series identified that subset as the most favorable.
Conclusion
Our data, compared with a similar cohort of patients two decades earlier, 4 shows a definitive improvement in median survival from 26 months to 33 months despite the exclusion of the most favorable group of patients (those with soft-tissue-dominant disease most of whom had local-regional disease) in the present series. A literature review of recent publications revealed heterogeneity of data and conclusions, with most suggesting improvement in median survival in more recent patient cohorts and all confirming ER, DFI, and the dominant site of metastasis as important variables. Improvements have likely been due to more widespread use of taxanes, aromatase inhibitors (AIs), trastuzumab, and other new agents in recent years. Our data suggest that the new benchmark for MSFSR approaches 3 years.
Author Contributions
SBZ, TA, JZ, AJM, RLM, ERA, AM, SH, NJM, CLV conceived and designed the experiments, analyzed the data, wrote the first draft of the manuscript, contributed to the writing of the manuscript, agree with the manuscript results and conclusions, jointly developed the structure and arguments for the paper, made critical revisions and approved final version, and reviewed and approved the final manuscript.