
Abstract
Objective
To describe patient profiles and clinical outcomes associated with first-line endocrine monotherapy (ET) and chemotherapy (CT) for postmenopausal HR+/HER2– metastatic breast cancer (mBC) patients.
Methods
This is a retrospective chart review of 139 postmenopausal HR+/HER2– mBC patients initiating first-line ET monotherapy or CT. Overall survival (OS) was described using Kaplan–Meier curves. Exploratory comparative proportional hazards regression was conducted.
Results
Patients on first-line CT had significantly more frequent liver metastases than patients on first-line ET monotherapy at baseline. The median OS was 35.5 months [95% confidence interval (CI), 22.7–41.2 months] for patients on first-line ET monotherapy and 22.2 months (95% CI, 13.6–25.9 months) for those on first-line CT (P = 0.021). Adjusting for baseline characteristics, the OS between first-line ET monotherapy and CT was not significantly different.
Conclusions
Patients who were prescribed CT as first-line treatment had evidence of more advanced disease at baseline and shorter OS than those who received ET monotherapy as first-line treatment, suggesting a need for additional safe and effective treatment options for these patients.
Keywords
Introduction
Breast cancer is the most common type of malignancy among women, with over 200,000 new breast cancer cases diagnosed in 2014 in the United States. 1 Hormone receptor positive (HR+) breast cancer, including both estrogen-receptor positive and progesterone-receptor positive cancers, accounts for 75% of all breast cancer diagnoses. 2 Human epidermal growth factor receptor 2 negative (HER2–) breast cancer is characterized by the normal expression of the HER2 gene with few HER2 proteins in the tumor. 3 In a recent study among breast cancer cases with known HR and HER2 status, 72.7% were found to be HR+/HER2–. 4
HR+/HER2– metastatic breast cancer (mBC) typically receives one of two options of first-line treatment: endocrine therapy (ET) or chemotherapy (CT). 5 The goal of these therapies is to improve quality of life and prolong survival. 6 ET includes aromatase inhibitors (AIs), which block steps in the biosynthetic pathway of estrogen, and selective estrogen receptor modulators (SERMs), which modulate the effect of estrogen at the receptor level.6,7 AIs have largely replaced SERM treatments as the preferred ET for mBC in postmenopausal women. 8 ET is currently recommended as first-line treatment for mBC, while CT is recommended only after three sequential ET regimens, except in cases of endocrine resistance or symptomatic visceral disease (often termed visceral crisis).9,10
Wilcken et al conducted a meta-analysis of randomized controlled trials comparing CT and ET in the treatment of mBC, but reported conflicting results on the comparative efficacy of the two treatment options. 11 Their pooled analysis of 10 previous studies found that CT was associated with a higher response rate than ET, but that the two treatment methods had similar overall survival (OS) rates. However, the studies used outdated ET and CT regimens and did not exclude cases whose HR status was negative or unknown. The comparative efficacy between contemporary ET and CT regimens is still poorly documented. Studies that assess the clinical outcomes of the two treatment options in real-world clinical practice are needed to provide further evidence on this topic. The objective of this study is to describe the clinical outcomes of ET monotherapy and CT used as first-line treatment for postmenopausal HR+/HER2– mBC patients in real-world clinical settings.
Methods
Patients
This is a retrospective chart review study, and details of the study have been published previously. 12 Briefly, patient charts were selected from a network of 13 community-based oncology practices in the United States. Adult women with HR+/HER2– advanced breast cancer who progressed on adjuvant or first-line treatment of advanced disease at any time between January 1, 2004 and September 30, 2010 were included. Advanced breast cancer was defined as breast cancer (new diagnosis or local, regional, or distant recurrence) not amenable to surgery or radiotherapy, including Stage IIIA (except for T3N1M0 disease), Stage IIIB, Stage IIIC, and Stage IV. From this larger cohort, patients were selected for inclusion in this study if they were postmenopausal with a confirmed diagnosis of Stage IV (metastatic) HR+/HER2– breast cancer and had started either ET monotherapy or CT as their first-line treatment for mBC (Fig. 1). The study was approved by the jurisdictional IntegReview Institutional Review Board (IRB).

Sample selection for postmenopausal HR+/HER2– mBC patients.
Collection of patient data
A standardized chart abstraction form was developed by the study investigators to collect patient information, including demographics, insurance plan type, menopausal status, comorbidities, sites of metastasis, treatment history, and outcomes information. Experienced clinical research nurses verified the inclusion criteria, abstracted data from the electronic medical records for each patient, and entered the information into the online chart abstraction form. Abstracted patient data were anonymous and nonidentifiable.
Outcome measures
OS was defined as the time from the initiation of first-line therapy for mBC to death. Time on treatment was defined as the time from the initiation of first-line therapy to the discontinuation of the last observed line of therapy for mBC. Patients without death or discontinuation dates were censored at their last available visit date or at the end of the study period (September 30, 2012), whichever came first.
Statistical analysis
The overall sample was classified by first-line treatment of mBC into ET monotherapy and CT groups. A modified Charlson Comorbidity Index (CCI) was calculated, which excluded breast cancer from the index. Baseline characteristics were compared among three subgroups: first-line CT, first-line ET monotherapy with CT at later lines, and first-line ET without CT at later lines, using Wilcoxon rank-sum tests for continuous variables and Fisher's exact tests for categorical variables.
The OS of patients on first-line ET monotherapy and CT was estimated using Kaplan-Meier curves and compared using log-rank tests. OS was further stratified by baseline metastatic sites. Time on treatment was described and compared between patients on first-line ET monotherapy and CT. In an exploratory analysis, multivariable Cox proportional hazards regression models were used to examine the association of first-line treatment with OS while adjusting for potential confounding due to available baseline characteristics. The baseline characteristics included age, commercial insurance, modified CCI, baseline metastasis (visceral, bone, other), history of adjuvant treatment, and time to recurrence (for recurrent tumors, this was the time from the initial diagnosis of breast cancer to recurrence, and the time was standardized before entering the model; for other cases, it was defined as zero).
Results
A total of 139 patients were included in the study with a median follow-up time of 26 months, among whom 34 received CT and 105 received ET monotherapy as their first-line treatment. Among patients receiving first-line ET monotherapy, 66 patients received CT at later lines (Table 1). A majority of patients had commercial or private insurance, though patients who received CT tended to be more likely to have commercial insurance. Patients who received first-line ET monotherapy and no later CT tended to be older than those who received CT for first-line or later line treatment (P < 0.001).
Baseline characteristics of Stage IV postmenopausal patients who received first-line chemotherapy (CT) or endocrine monotherapy (ET).

Refers to patients who received chemotherapy either as monotherapy or in combination with other therapies as first-line treatment.
Continuous variables were compared between groups using Wilcoxon rank-sum tests, while categorical variables were compared using Fisher's exact tests.
Other insurance plan types include AARP and Medicare supplement.
Other sites of metastatic disease include the bone marrow, peritoneum, chest wall, colon, stomach, omentum, bladder, and skin. One physician reported the disease as “widely metastatic”. Pleural effusion and subcutaneous masses on back and skin were also noted.
P < 0.05;
P < 0.001.
The median modified CCI (excluding breast cancer) was 0.0 for patients in all three subgroups, which suggests similar baseline comorbidity levels among these groups. However, patients who received first-line ET monotherapy and no later CT had higher CCI levels (levels 3 and 4) compared with patients who had ever received CT. The most frequent metastatic site at the initiation of first-line therapy was bone, followed by liver and lung. Patients on first-line CT had more frequent liver or lung metastases than patients on first-line ET monotherapy, although the difference of lung metastases was not statistically significant (P = 0.087). The frequency of metastasis of other sites did not differ significantly among the three groups. The most frequently used first-line ET agents were letrozole (35.2%), followed by anastrozole (28.6%) and fulvestrant (21.9%). The most frequently used first-line CT agents were capecitabine (35.3%), followed by paclitaxel (29.4%), docetaxel (29.4%), gemcitabine (14.7%), and cyclophosphamide (11.8%). No patient received any HER2-targeted therapy.
The median survival time was 35.5 months [95% confidence internal (CI), 22.7–41.2 months) for patients on first-line ET monotherapy and 22.2 months (95% CI, 13.6–25.9 months) for those on first-line CT, and the difference was statistically significant (P = 0.021, Fig. 2). When patients on first-line ET monotherapy were further stratified, those who received CT at later lines appeared to have a shorter median survival (34.1 months; 95% CI, 22.5–41.0 months) compared with those who never received CT (39.5 months; 95% CI, 19.2–59.7 months). The median time on treatment was 33.4 months (95% CI, 22.3– 39.3 months) for patients on first-line ET monotherapy and 19.6 months (95% CI, 10.5–24.4 months) for those on first-line CT, and the difference was also statistically significant (P = 0.027, Fig. 3).

Comparison of overall survival between postmenopausal BC patients receiving endocrine monotherapy versus chemotherapy as first-line treatment for stage IV BC.

Comparison of time to treatment discontinuation between postmenopausal BC patients receiving endocrine monotherapy versus chemotherapy as first-line treatment for stage IV BC.
When stratified by baseline metastatic status (Table 2), patients who had visceral metastasis and received first-line ET monotherapy had significantly longer survival, compared with those who received first-line CT (P = 0.037). However, among patients with only bone metastasis, there was no significant difference in OS between the two treatment groups (P = 0.721). In the exploratory Cox regression analyses (Table 3), the unadjusted hazard ratio (HR) for the risk of death for patients on first-line ET monotherapy versus CT was 0.60 (95% CI, 0.39–0.93; P = 0.023), suggesting that patients in the ET group had longer OS. After adjusting for baseline characteristics, the HR was no longer statistically different from equivalence (HR = 0.64; 95% CI, 0.39–1.06; P = 0.084).
Overall survival of postmenopausal women receiving endocrine therapy versus chemotherapy as first-line treatment for stage IV BC stratified baseline metastatic status.

P-values were generated from log-rank tests.
Cox proportional hazards model for survival time in Stage IV postmenopausal patient receiving first-line chemotherapy or endocrine monotherapy.
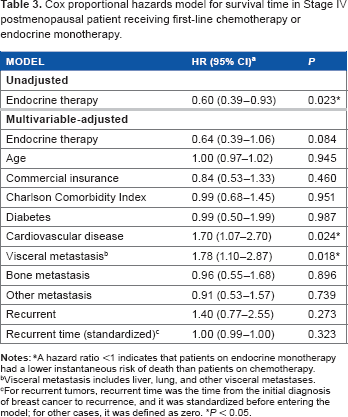
A hazard ratio <1 indicates that patients on endocrine monotherapy had a lower instantaneous risk of death than patients on chemotherapy.
Visceral metastasis includes liver, lung, and other visceral metastases.
For recurrent tumors, recurrent time was the time from the initial diagnosis of breast cancer to recurrence, and it was standardized before entering the model; for other cases, it was defined as zero.
P < 0.05.
Discussion
In this study, we investigated the clinical outcomes of ET monotherapy and CT when used as first-line treatment for postmenopausal HR+/HER2– mBC patients. The presence of liver metastases at the initiation of treatment was associated with an increased use of CT as first-line therapy, whereas the presence of bone metastasis seemed uncorrelated with CT use. This is consistent with current recommendations that CT be used for the treatment of symptomatic visceral disease. 5 Patients on first-line CT did not differ significantly from those on first-line ET monotherapy on other baseline characteristics, including CCI and the presence of other metastatic sites. About 42% of the patients who received first-line ET never received CT in later lines (throughout the treatment history during the study period). Compared with patients who received CT for first- or later line treatment, patients who were treated with ET only were significantly older in age, had more comorbid conditions, and were less likely to have liver metastasis (suggesting less aggressive disease). This suggested that in the clinical practice setting, physicians’ key considerations for choosing ET (over CT) might be older age, more comorbidities, and less aggressive disease.
Overall, there were indications that patients receiving first-line CT might have had more advanced or aggressive disease than those receiving first-line ET monotherapy. In univariate analysis, the ET monotherapy group had a longer median OS; however, after adjusting for baseline covariates, the difference between the first-line ET monotherapy and CT groups became nonsignificant. This result suggests that the observed difference of survival times between patients on first-line ET and those on first-line CT might be due to differential patient characteristics at baseline. Results of the analyses stratified by baseline metastatic sites support this hypothesis, since the survival benefit of first-line ET was observed only among patients with visceral metastasis but not with only bone metastasis.
Furthermore, one recent cross-sectional survey indicated that patients with HR+/HER2– mBC receiving ET reported greater health-related quality of life, satisfaction with treatment, and better feeling about side effects compared with those receiving CT. 12 In addition, previous studies found that costs related to CT adverse events were significantly higher compared with those of the ET-based regimens in the treatment of advanced breast cancer. 13 The goal of the systemic treatment of mBC is to prolong survival and to enhance quality of life; thus, the guidelines usually prefer ET, which can be effective with less toxicity than CT. 5 Even though CT is recommended when there is endocrine refractory disease or symptomatic visceral disease, the guidelines still recommend ET for asymptomatic visceral involvement in the absence of endocrine refractory disease.5,14
The primary objective of this study was to describe the clinical outcomes of different first-line treatments, and the comparative analyses were exploratory. This study is subject to several important limitations. First, the statistical power may be limited by small sample size. Future studies with a larger sample size of mBC patients are warranted to confirm these results. Second, the difference of OS between patients on first-line ET monotherapy and CT is subject to confounding by indication, because more severe cases with worse prognosis are often treated with CT. We have adjusted several surrogate factors at baseline to control for this confounding, but these variables may not be sufficient to fully capture the baseline differences between patients who started with ET monotherapy and those who started with CT. Thus, the possibility of residual confounding cannot be excluded. Third, the quality of life at the treatment initiation could be an important confounder, and relevant inputs from physicians or patients would be conducive to confounding control. However, such data were not captured in the medical charts. Although baseline measures of performance status, including the Karnofsky Performance Status (KPS) and the Eastern Cooperative Oncology Group (ECOG) Score were collected in the current study, the data retrieved were sparse and insufficient to adjust in the multivariate models. Moreover, information on the rationale or factors of consideration for physicians’ decision making on the treatment choice was not available. Unmeasured or sparsely measured confounders such as these are a limitation of real-world retrospective data collection.
Conclusion
Patients who were prescribed CT as first-line treatment for postmenopausal HR+/HER2– mBC appeared to have more advanced disease at baseline and shorter OS than those who received ET monotherapy as first-line treatment. This suggests that ET might be a safe and effective treatment option for patients who, in real-world practice, receive first-line ET. However, safer and more effective treatments are needed for patients who receive first-line CT. Future studies with larger sample sizes and systematic documentation of patient severity are warranted to further explore associations between first-line treatments and outcomes in mBC.
Author Contributions
Conceived and designed the study: YH, AM, PL, JS, EW. Analyzed the data: YS, AM, PL. Wrote the first draft of the manuscript: YS. Contributed to the writing of the manuscript: YH, AM, PL, JS, EW. Agree with manuscript results and conclusions: YS, YH, AM, PL, JS, EW. Jointly developed the structure and arguments for the paper: YS, YH, AM, PL, JS, EW. Made critical revisions and approved final version: YS, YH, AM, PL, JS, EW. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
The authors thank Emily Meade, an employee of the Analysis Group, Inc., who contributed to the preparation and editing of the manuscript.