
Abstract
Background:
Despite the approval of mTOR inhibitor everolimus and CDK4/6 inhibitors in the management of hormone-receptor-positive HER2 non-amplified metastatic breast cancer (HR+ HER2-MBC), the optimal sequence of therapy is unclear. There are no clinical data on efficacy of everolimus in HR+ HER2-MBC after cancer progresses on CDK4/6 inhibitors.
Objective:
The objective of this study is to find the efficacy of everolimus in HR+ HER2-MBC after they progress on a CDK4/6 inhibitor palbociclib.
Methods:
This is a retrospective, 2-institute review of HR+ HER2-MBC from Jan 2015 to March 2018 treated with everolimus after progression on palbociclib. Primary end point was median progression-free survival (PFS), secondary end points objective response rate (ORR), clinical benefit ratio (CBR), and overall survival (OS).
Results:
Out of 41 women with median age 61 years (33, 87) enrolled, 66% had received adjuvant systemic therapy, 61% had visceral disease, and 95% had prior nonsteroidal aromatase inhibitors. About 83% women had 3 or more chemotherapy or hormonal therapies prior to everolimus. Kaplan-Meier estimates showed a median PFS of 4.2 months (95% confidence interval [CI]: 3.2-6.2). The median OS was 18.7 months (95% CI 9.5 to not reached). Objective response rate and CBR were both 17.1%.
Conclusion:
Everolimus was associated with modest PFS and ORR in HR+ HER2-MBCs postprogression on palbociclib.
Introduction
Endocrine therapy forms the backbone in the management of metastatic-hormone-receptor-positive (HR+) breast cancer. In the recent years, novel targeted approaches when combined with endocrine therapy have shown to improve progression-free survival (PFS). The BOLERO2, a phase-3, randomized, controlled trial of women with advanced HR+ HER2 non-amplified (HER2–) metastatic breast cancer (MBC), demonstrated a statistically significant improvement in (PFS) in women who were treated with the combination of everolimus plus exemestane as compared to exemestane alone. 1 The combination was approved in the United States for treatment HR+ HER2-MBC after failure of treatment with an aromatase inhibitor (AI) in July 2012. 2 Since 2015, the US Food and Drug Administration (FDA) has approved 3 CDK4/6 inhibitors, palbociclib, ribociclib, and abemaciclib, in combination with endocrine therapy as first line or subsequent lines of therapy for HR+ HER2-MBC after their respective phase-3 clinical trials showed significant improvement in PFS with these combination as compared to endocrine therapy alone in both front and subsequent line therapies.3-11 Current paradigm favors the use of CDK4/6 inhibitors prior to everolimus in the treatment sequence, although optimal sequence of therapy has not been established. Breast tumor biology evolves with treatment, acquiring genetic changes and developing resistance to therapy. 12 The tumor biology and resistance pattern of the BOLERO2 cohort could be significantly different from present day HR+ MBC cohorts who are resistant to CDK4/6 inhibition. Multiple preclinical studies have suggested interactions between the PI3K/Akt/mTOR pathway and the downstream Cyclin D/CDK4/6/Rb pathway. It raises the possibility of cross-resistance between an mTOR inhibitor and CDK4/6 inhibitors while other studies have shown that cell cycle inhibition is associated with a compensatory activation of mTOR/AKT pathway, increased Cyclin D expression leading to a leak in the cell cycle block and thus resistance to CDK4/6 inhibitor.13-20 Currently, there are no clinical data on the efficacy of everolimus combinations in HR+ HER2-MBC after they have progressed on CDK4/6 inhibitor-based combinations. The objective of this study is to find the efficacy of everolimus combinations among HR+ HER2-MBC patients after progression on palbociclib combinations.
Methods
This is a retrospective, 2-institute review of HR+ HER2-MBC patients from January 2015 to March 2018 treated with everolimus combinations after progression on palbociclib combinations. MBC patients with biopsy proven estrogen receptor-positive (ER+) HER2– carcinoma who received palbociclib combinations prior to everolimus combinations were eligible for the study. Based on the American Society of Clinical Oncology/College of American Pathologists guidelines, breast carcinomas with 1% of more immuno-reactive tumor cells for ER on immunohistochemistry (IHC) or an Allred score of 3 or more were considered as ER+ breast cancer. 21 Similarly, 0 or 1+ scores of HER2 stain on IHC or average HER2 copy number <4.0 signals per cell (single probe assay) or HER2/CEP17 ratio <2.0 and average HER2 copy number <4.0 signals per cell (dual-probes assay) using fluorescence in situ hybridization (FISH) was considered HER2 non-amplified. 21 Patients with primary ER+ carcinoma whose biopsy of subsequent metastatic tissue was ER– were eligible for study only if these patients continued to receive endocrine-based therapy for the metastatic disease based on providers’ clinical judgment. Women who received everolimus or palbociclib for less than 4 weeks were excluded to ensure minimum meaningful exposure to both drugs in enrolled patients. Any starting dose of everolimus was allowed. Primary end point of the study was the analysis of median PFS and secondary end points were to calculate the objective response rate (ORR), clinical benefit ratio (CBR), and overall survival (OS) of these patients on everolimus combinations. Progression-free survival was defined as the time from the initiation of everolimus to the date of death or progression, whichever occurs first. Progression was determined by the treating physicians based on radiological, biochemical, and/or clinical criteria. Best overall response rates were determined based on available radiological data. The objective response rate was defined as the rate of any complete or partial responses (CR or PR). Clinical benefit (CB) was defined as CR or PR or stable disease (SD) of at least 6 months.
Separate institutional review board (IRB) approvals were obtained at Roswell Park Comprehensive Cancer Center (Roswell Park) and University of Pittsburgh Medical Center (UPMC) prior to data extraction. Preliminary patients’ lists were generated by computer-based queries by respective bioinformatics resources available at these centers. Chart review and eligibility assessment were performed by A.D. (Roswell Park) and R.A.T (UPMC). Final composite data were analyzed at Roswell Park.
Results
Screening
Initial query on electronic medical records from Roswell Park main campus and a satellite location yielded 31 eligible patients, out of which 7 patients were excluded: 4 patients received everolimus prior to palbociclib, 1 patient received everolimus for less than 4 weeks, 1 patient received insurance approval for everolimus but never used it and last patient’s subsequent biopsy showed triple-negative breast cancer though she had ER+ primary breast cancer in the past. Similarly, out of 27 initial patients from UPMC, 10 were excluded: 5 patients received everolimus for less than 4 weeks, 4 patients received everolimus prior to palbociclib and 1 patient received palbociclib for less than 4 weeks. Among those 6 ineligible patients who received everolimus for less than 4 weeks, everolimus was discontinued due to progression of disease in 3 patients, intolerance in 1, and data were immature (less than 4 weeks) for the remaining 2 patients. Full data extraction and analysis was performed on a total of 41 patients.
Patients’ characteristics
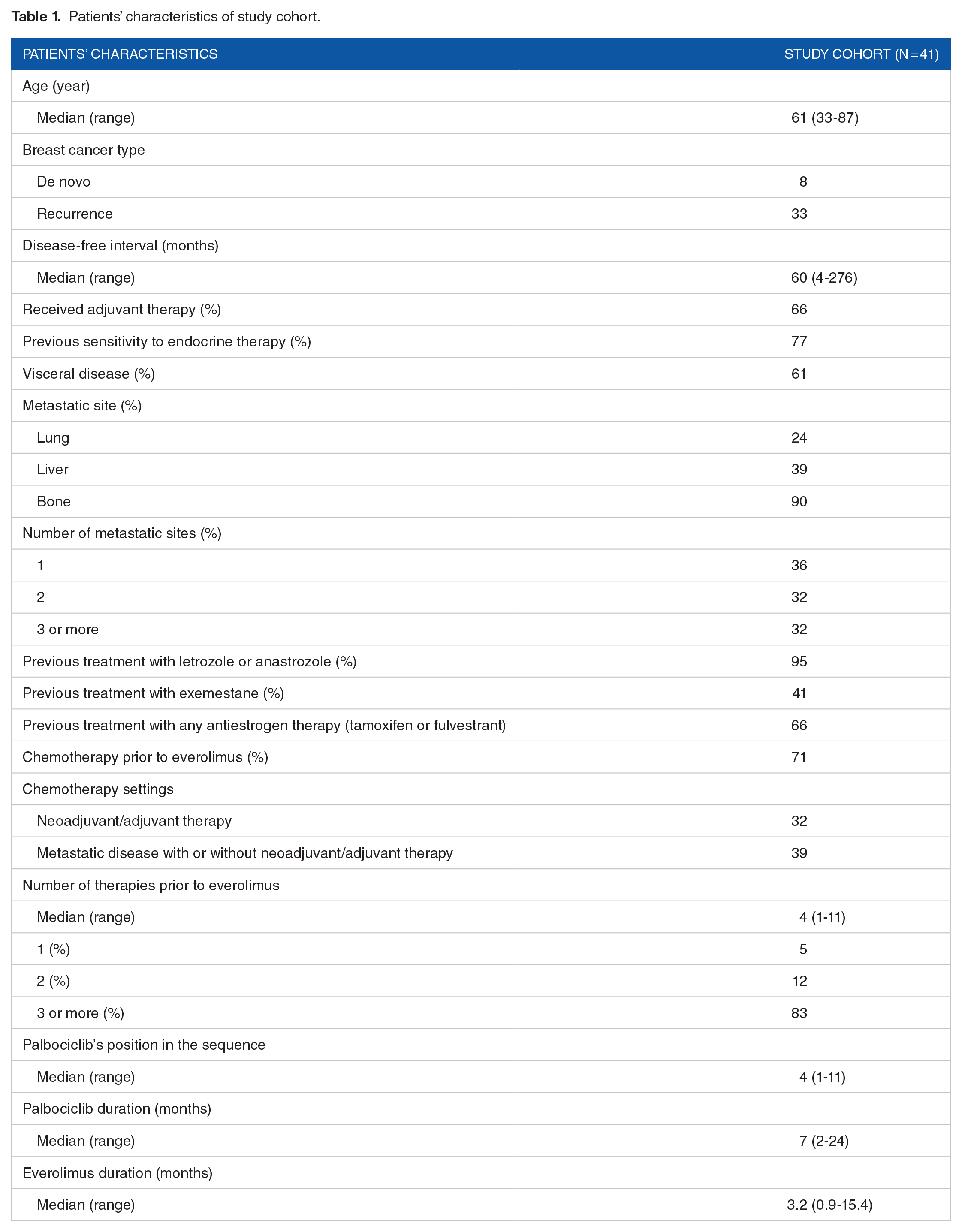
Median age of the patients was 61 years (range: 33-87). Thirty-eight patients had biopsy proven ER+ MBC while the remaining 3 patients had ER+ breast cancer in their primary biopsy but ER– in the biopsy of the metastatic site. These patients were treated by their physicians as ER+ breast cancers based on the clinical judgment which appeared to be influenced by natural history of disease and suboptimal biopsy tissue from the metastatic site. These patients were also enrolled in the study. Around 72% of the women had progesterone-receptor-positive tumor, all of the women had HER2– (56% by IHC alone, remaining confirmed by FISH) disease. Median disease-free interval (duration between diagnosis of primary breast cancer and the recurrence) was 60 months (4, 276). Twenty-six out of 41 patients (66%) had received adjuvant therapy (chemotherapy and/or hormonal therapy). Out of 14 patients who did not receive any adjuvant chemotherapy and/or hormonal therapy, 8 were de novo metastatic disease. About 77% patients had demonstrated prior sensitivity to endocrine therapy, which was defined as at least 24 months of endocrine therapy before recurrence in the adjuvant setting or a complete or partial response or stabilization of disease for at least 24 weeks on endocrine therapy for advanced disease. About 61% women had visceral disease, 90% of the women had bone metastases, and 32% had 3 or more organs involved with metastases. Almost 95% had prior non-steroidal AIs, 41% had prior exemestane, and 66% had prior tamoxifen. Around 71% had received prior chemotherapy for breast cancer, of which 45% had received it in adjuvant/neoadjuvant settings while the remainder received chemotherapy in the metastatic or in both settings. Median number of therapies, counting chemotherapy, and hormonal therapy, prior to everolimus was 4 (1, 11), and 83% had 3 or more prior chemotherapy or hormonal therapies prior to everolimus. Median order of palbociclib was 4th (1st, 11th) in the sequence of therapies, and median duration of palbociclib-based therapies was 7 months (2, 24). Median duration of everolimus combinations was 3.2 months (0.9, 15.4). See Table 1 for patients’ characteristics of study cohort.
Patients’ characteristics of study cohort.
Efficacy of everolimus-based therapy
Out of 41 patients, 27 patients had primary events (25 progressions, 2 deaths) on everolimus therapy. Out of 25 patients who progressed, 23 had radiographic evidence of progression. The remaining 2 patients were considered to have progressed by their physicians based on clinical and laboratory evidence (increasing tumor markers and new skin and breast mass; increasing tumor markers and decline in overall performance status, patient referred to hospice). Kaplan-Meier estimates showed a median PFS of 4.2 months (95% confidence interval [CI]: 3.2-6.2) (Figure 1). At a median follow up of 7.4 months (0.9, 23.2), 10 patients had died. The median OS was 18.7 months (95% CI: 9.5 to not reached) (Figure 2). About 17.1% of women had partial response, 36.6% had stable disease, 31.7% had progressive disease, and 14.6% had not reached a response yet. About 17.1% had objective responses on everolimus combinations, 63.4% did not have any objective responses while 19.5% had not reached objective responses at the time of data extraction. Median time to objective response was 3.1 months (2.0, 4.2). By the time of final data extraction, 7 (17.1%) patients had achieved clinical benefit with everolimus combinations. Median duration of clinical benefit was 8 months (7, 16) with mentionable duration of 13 and 16 months in 2 women. Twenty-four patients failed to achieve clinical benefit, while data were premature for remaining 10 patients, 5 of which already had stable diseases on restaging scans. See Table 2 for response rates of study cohort.

Kaplan-Meier estimates show a median progression-free survival of 4.2 months (95% CI: 3.2-6.2). CI indicates confidence interval.

Kaplan-Meier estimates show a median overall survival of 18.7 months (95% CI: 9.5 to not reached). CI indicates confidence interval.
Tumor response on everolimus-based therapy.

Discussion
This study has provided clinical efficacy data of everolimus-based combination in HR+ HER2-MBC patients, who have progressed on palbociclib-based combinations. The median PFS of our study cohort was 4.2 months (95% CI: 3.2-6.2) while that of the everolimus plus exemestane arm of the BOLERO2 was 6.9 months (95% CI: 6.4-8.1). 1 The median OS of our study cohort was 18.7 months (95% CI: 9.5 to not reached), while that of the everolimus cohort of BOLERO2 was 31.0 months (95% CI: 28.0-34.6). 22 About 17.1% of women in our study cohort had an objective response and same percentage achieved predefined clinical benefit. About 9.5% women in the everolimus cohort of BOLERO2 had an objective response. The patient and disease characteristics between this study cohort and the everolimus cohort of BOLERO2 are comparable in terms of age, disease-free interval, prior sensitivity to endocrine therapy, and disease burden. This study cohort received a median of 4 lines of therapy prior to an everolimus combination as compared to a median of 3 lines of therapy on the BOLERO2 cohort. About 83% women in the study cohort received 3 or more lines of therapy prior to the everolimus combination while only 54% women in the everolimus plus exemestane cohort of BOLERO2 had 3 or more lines of prior therapy. Thus, our study cohort had more heavily pretreated women and everolimus combinations were initiated in later stages of the MBC therapy as compared to BOLERO2 cohorts. In addition, our cohort received up to 23.6 months (median 7.0 months) of palbociclib therapy in the earlier part of the MBC therapy. Thus, compared to everolimus cohort of BOLERO2, women on our cohort received longer duration of prior endocrine-based therapy due to the use of palbociclib.
Given the clear PFS benefit in front-line settings as compared to an AI and relatively good side effect profile, CDK4/6 inhibitors are being used as first or second line of therapy, and everolimus combinations are used later in the sequence of therapies for HR+ HER2-MBC. Whether this sequence is the best approach will become clearer after the maturity of OS data from the first-line CDK4/6 inhibitors trial and the BOLERO4 trial.4-6,23 A randomized study comparing the sequence of CDK4/6 inhibition followed by mTOR inhibition versus the opposite may provide a definite answer and some biomarkers to help guide clinicians.
A retrospective study design, a relatively small sample size, and nonstandard response assessments are the major limitations of this study. In addition, performance status could not be analyzed in this retrospective study due to the inconsistent documentation in the medical record. Unlike the BOLERO2 where all patients in the everolimus cohort received everolimus plus exemestane, our cohort contained patients treated with everolimus plus any AI or fulvestrant. Detail information of the endocrine therapy partner of everolimus was not obtained during the chart review. However, 41% of the patients had prior exemestane in our cohort, 95% had prior letrozole or anastrozole, and 66% had prior fulvestrant or tamoxifen. Everolimus toxicity and dose reduction information was not obtained in this study. The results of the BOLERO2 trial has been used as a reference for the efficacy of everolimus combinations in the pre-CDK4/6 inhibitor era in this study. The real-world data may differ from the data of clinical trials as the clinical trials triage fitter patients with lesser comorbid conditions and monitor patients more closely. We did not obtain data of everolimus combination used in the pre-CDK4/6 inhibitor era at our institutions in this study. However, there are some published real-world data on the efficacy of everolimus combination in HR+ HER2- MBC after the progression of an AI. Hao et al 24 performed a chart review of 192 ER+ MBC patients from community-based oncology practices, who received everolimus combination after progression on an AI, showing a median PFS was 9.1 months. Similarly, Xie et al 25 performed a chart review of 243 ER+ MBC patients from community-based oncology practices, who had received everolimus combination after progression on an AI, demonstrating a median PFS of 8.5 months.
Our study is the first to provide evidence of clinical benefit of targeting mTOR pathway postprogression on CDK4/6 inhibitor combination. Despite limitations of our study, we show that everolimus remains a potential treatment option in the current treatment climate with small percentage of patients obtaining prolonged clinical benefit.
Conclusion
Our study, for the first time, provides clinical data showing benefit of using everolimus combinations postprogression on CDK4/6 inhibitor treatment in patients with HR+ MBC. The combination was associated with a modest PFS of 4.2 months and ORR of 17.1%. Only 7 out of 41 women achieved clinical benefit, but 2 of them had prolonged benefit of 13 and 16 months. These results will assist clinicians in having an informed conversation with patients when everolimus therapy is being considered after CDK4/6 inhibition therapy.
Footnotes
Acknowledgements
Clinical Data Network (CDN), Roswell Park Cancer Institute Shared Resource.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute (NCI) grant P30CA016056 involving the use of Roswell Park Cancer Institute’s Pathology Network, Genomic, and Clinical Data Network Shared Resources.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.G.L. has received royalty from UpToDate. A.B. has/had consulting or advisory role for Agendia, Bayer, bioTheranostics, Celgene, Genentech/Roche, Genomic Health, Lilly, NanoString Technologies, Novartis, Pfizer, and Puma Biotechnology. A.P.E. has received honorarium from Pfizer. M.O. has received research fund from Pfizer/NCCN and has/had consulting or advisory role for Novartis and AstraZeneca. A.D. has received honorarium from Daiichi Sankyo. All other authors declare that they have no conflict of interest.
Authors’ Contribution
A.D. and M.O. contributed to the study conception and all authors contributed to study design. A.D. and R.A.T. performed material preparation and data collection. A.D., M.O., K.A., and A.M. contributed to statistical analysis and interpretation. M.O. provided supervisory role in the study. A.D. and M.O. wrote the first draft of the manuscript. All authors have provided critical input to the design of the study and the manuscript preparation. All authors read and approved the final manuscript.
Ethical Standard
This study was approved by Institutional Review Boards at Roswell Park Comprehensive Cancer Center and the University of Pittsburgh Medical Center. This research did not involve animals or human participants. This research was a retrospective chart review.
Prior Publication
None. Abstract presented at ASCO annual meeting, 2018.