
Abstract
Mucinous cystic neoplasms (MCNs) of the pancreas in male patients are very rare. Though few cases of MCNs in male patients have been reported, it is difficult to reveal them preoperatively. The first patient was a 50-year-old man and was incidentally found to have a cystic mass of 51 mm in the tail of the pancreas. We performed a distal pancreatectomy. The second patient was a 73-year-old man, incidentally found to have a cystic mass of 25 mm in diameter in the tail of the pancreas and a carcinoma of the bile duct. We performed a subtotal stomachpreserving pancreaticoduodenectomy and distal pancreatectomy. In both cases, the cystic lesion was diagnosed pathologically as MCNs. Since MCNs have the risk of malignancy, a resection is recommended. Cases of MCNs in male patients exhibit features that are similar to MCNs in women. We should recognize that MCNs of the pancreas in male patients exists.
Introduction
Mucinous cystic neoplasms (MCNs) were defined by the World Health Organization in 1996 and by the Armed Forces Institute of Pathology in 1997. MCNs of the pancreas are thought to occur almost exclusively in women; therefore, these are often misdiagnosed preoperatively in men. It is important to remember that MCNs may occur in men, and we should consider MCNs as one of the differential diagnoses when assessing a cystic lesion of the pancreas in male patients. Here we report two cases of MCNs in men.
Case Report #1
A 50-year-old man was referred to our hospital with a cystic mass in the tail of the pancreas. This cystic mass was incidentally detected when he underwent a laparoscopic cholecystectomy for cholecystitis 7 years previously, and it increased from 22 to 51 mm. The laboratory tests were normal. Abdominal computed tomography (CT) revealed a multilocular cystic mass without any nodules in the pancreatic tail (Figure 1). On magnetic resonance imaging, the cystic mass was observed to be hyperintense with a septum in T2-weighted images. Because of the increase in the cyst size, the patient underwent distal pancreatectomy with splenectomy. On histopathological examination, the cystic lesion exhibited a flat mucinous epithelial layer and an ovariantype stroma. No significant atypia was identified, and there was no communication between the main pancreatic duct and the cystic lesion. Immunohistochemical analysis revealed that the stromal layer was positive for estrogen and progesterone receptors. From these findings, the cystic lesion was diagnosed as MCNs of the pancreas. The patient was discharged on postoperative day 15 without any complications.
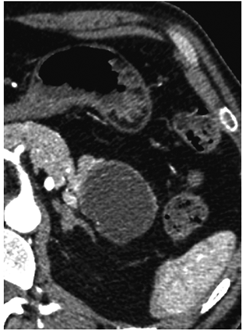
Abdominal computed tomography. The size of the multilocular cystic mass was 51 mm, without a nodule in the pancreatic tail.
Case Report #2
The patient was a 73-year-old man who had undergone an endovascular aortic repair for an aneurysm of the iliac artery. A cystic lesion was incidentally detected in the pancreas by CT obtained for the workup of the aneurysm 3 years previously. The cystic mass had increased from 15 to 25 mm. Laboratory tests showed elevated CEA levels of up to 5.2 ng/mL (normal range, <5 ng/mL) and CA19-9 levels of up to 156.3 U/mL (normal range, <37 U/mL). Abdominal CT revealed a multilocular cystic mass without any nodules in the pancreatic tail and intrahepatic biliary dilation and stenosis of the common bile duct (Figure 2). On endoscopic retrograde cholangiopancreatography, the cystic lesion showed no communication with the main pancreatic duct. Cytological examination of bile samples showed false positive. We diagnosed primary bile duct cancer and MCNs of the pancreas; therefore, we performed a subtotal stomach-preserving pancreaticoduodenectomy and distal pancreatectomy, preserving the spleen. Microscopically, the cystic lesion revealed a single layer of mucinous columnar cells and an ovarian-type stroma. No significant atypia was identified. Immunohistochemical analysis revealed that the stromal layer was positive for estrogen receptors. From these findings, the cystic lesion was diagnosed as MCNs of the pancreas. Further, histological examination confirmed a well-differentiated tubular adenocarcinoma of the bile duct [T3N0M0 stage IIA (UICC TNM staging)]. The patient was discharged from the hospital without any adverse events.

Abdominal computed tomography. a) The size of the multilocular cystic mass was 25 mm, without a nodule in the pancreatic tail. b) The common bile duct was enhanced and stenosed.
Discussion
According to the definition by World Health Organization, MCNs are characterized by columnar, mucin-producing epithelium supported by ovarian-type subepithelial stroma. The origin of the ovarian-type stroma in MCNs remains unclear, but MCNs are generally thought to occur almost exclusively in women. 1
MCNs carry a malignant potential with a reported incidence of high-grade dysplasia or invasive adenocarcinoma of 10-39%.2–7 An increased tumor size, particularly those >4 cm, the presence of mural nodules, and elevated serum CEA and CA19-9 levels are associated with a high risk of malignancy.4,5,8 Radical resection of MCNs without malignant lesions is determined as complete cure, and these lesions do not recur. However, in patients with malignant lesions, the 5-year survival rate is 15-35%. 9 Therefore, early diagnosis and early surgical intervention are important, and the international consensus guidelines recommend resection of all suspected MCNs when feasible. 10
MCNs are rare in male patients and are often misdiagnosed preoperatively. Only 12 cases have been reported to date (Table 1),4,5,9,11–17 and none of these cases, except for case 2 presented in this report, was diagnosed as MCNs preoperatively. The remaining 11 cases underwent surgical resection because of increasing tumor size, and the median tumor size at the time of the surgery was 45.5 mm. Case 1, presented in this report, was followed up at a local clinic for 7 years, during which the pancreatic tumor doubled in size from 22 to 51 mm. Fortunately, no malignancy was found during the postoperative pathologic examination, but the increased risk of malignancy related to the increased tumor size, particularly those >40 mm, warranted prompt surgical intervention. Case 2 had a 25-mm multilocular cystic lesion in the pancreatic tail. Except for the patient's sex, the typical radiological findings (multilocular cyst-incyst mass in the pancreatic tail and no communication between the main pancreatic duct and the cystic mass) led to MCNs as one of the preoperative diagnoses. The lesion was small, but because the patient was also diagnosed with cholangiocarcinoma, he underwent surgical resection of both the lesions, and the postoperative pathologic examination confirmed MCNs diagnosis.
Mucinous cystic tumor in male patients.
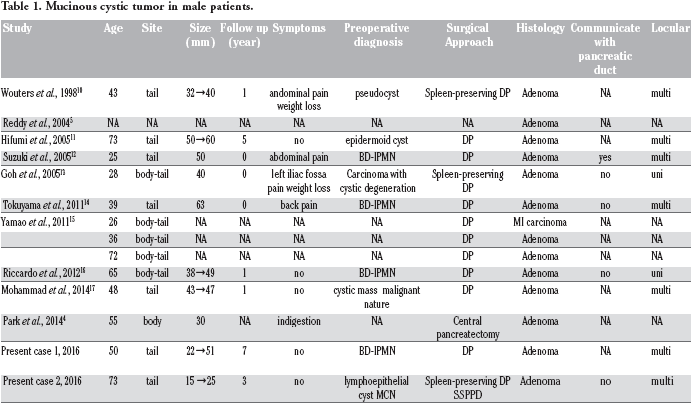
According to the 12 cases reported to date, there seems to be no typical age group for male subjects with MCNs; the reported median age was 49 years (range, 25-73 years). The typical features of MCNs, such as cystic lesions with a multiloculated cystin- cyst appearance occurring in the distal pancreas, can also be applied to male patients. 16 Although MCNs typically have no communication with the main pancreatic duct, some cases of MCNs that do communicate with the pancreatic duct have been reported. 18 It is important to acknowledge that MCNs occur in male patients. When the radiological findings are highly suggestive of MCNs, it should be considered as one of the differential diagnoses, even in male patients.
Conclusions
We reported two cases of MCNs in male patients. When the typical features of MCNs are observed in a male patient, it must be considered as one of the differential diagnoses and surgical resection must not be delayed.
Footnotes
Acknowledgements
We wish to thank department of Pathology, Seirei Hamamatsu General Hospital for supporting.