
Abstract
Mucinous cystic neoplasms (MCNs) make up a morphologic family of similar appearing tumors arising in the ovary and various extraovarian organs such as pancreas, hepatobiliary tract and mesentery. MCNs of the pancreas occur almost exclusively in women. Here, we report a rare case of MCN in a male patient. A 39-year-old man was admitted to our hospital with the chief complaint of back pain. Abdominal computed tomography revealed a multilocular cyctic mass 6.3 cm in diameter in the pancreatic tail. In addition, the outer wall and septae with calcification were demonstrated in the cystic lesion. On magnetic resonance imaging, the cystic fluid had low intensity on T1-weighted imaging and high intensity on T2-weighted imaging. Endoscopic retrograde cholangio-pancreatography (ERCP) showed neither communication between the cystic lesion and the main pancreatic duct nor encasement of the main pancreatic duct. Endoscopic ultrasonography revealed neither solid component nor thickness of the septae in the cystic lesion. Consequently, we performed distal pancreatectomy with splenectomy under the diagnosis of cystic neoplasia of the pancreas. Histopathologically, the cystic lesion showed two distinct component: an inner epithelial layer and an outer densely cellular ovarian-type stromal layer. Based on these findings, the cystic lesion was diagnosed as MCN.
Introduction
Mucinous cystic neoplasms (MCNs) have been defined as large, separated, thick-walled cysts without connection to the pancreas duct system. 1 Based on the WHO criteria in 1996, the study for 130 cases of MCN with ovarian type stroma (OS) indicated to be female patients appearances in whole cases and body/tail location in almost. 2 Therefore, as a rough rule for pancreas cystic neoplasms, in male and in the head of the pancreas are likely to be IPMNs, whereas cyctic lesions in the body/tail in female may be either an MCN or IPMN. 3 And, in the past several years, mucinous cystic neoplasms of the pancreas have been diagnosed more and more frequently. Then it has become crucial for physicians working in this field to have a clear understanding of the biology on these tumors. From recent our experience for a male case with MCN, which is quite rare, diagnostic evaluation and therapeutic procedures including surgical indication will be argued with the references.
Case Report
A 39-year-old man was admitted to our hospital with the chief complaint of back pain. There was no history of previous abdominal imaging examinations, and another abdominal episode, such as sudden abdominal pain, abdominal trauma, or abdominal operation. He was just social drinker of alcohol and was not smoker. On physical examination, abdomen was soft and flat, and no tenderness was noticed. Laboratory tests showed an elevation of both AST, up to 39 IU/l (normal≦35 IU/L), and ALT, up to 56 IU/L (normal≦40 IU/L). The other data including tumor markers (CEA, CA19-9 and DUPAN-2) were within normal range. Abdominal CT revealed a multilocular cyctic mass, 6.3 cm in diameter, with wall calcification in the pancreatic tail (Figure 1). On MRI, the cystic lesion was hypointense in T1-weighted imaging and hyperintense in T2-weighted imaging with low intense capsule and septum (Figure 2a,b). ERCP showed neither communication between the cystic lesion and the main pancreatic duct nor encasement nor interruption of the main pancreatic duct. Endoscopic ultrasonography revealed neither solid component nor thickness of the septae in the cystic lesion. Consequently, under the diagnosis of neoplastic cyst of the pancreas, such as lymph epithelial cyst, serous cystic neoplasm, branched-type lesion of IPMN, cystic change of endocrine tumor, and epidermoid cyst derived from accessory spleen in the pancreas, distal pancreas with spleen was removed. Macroscopically (Figure 3), the cystic lesion, measuring for 6.5×5.8×5.2 cm in size, was round with a smooth surface and was surrounded by normal pancreatic tissue. The cut surface demonstrated a multilocular cystic pattern containing thick yellowish mucin, and the lesion was surrounded by a fibrous capsule. There was neither mural nodule nor papillary projections inside the cystic lesion. Microscopically (Figure 4a,b), the cystic lesion showed two distinct component; an inner mucinous epithelial layer and an outer densely cellular stromal layer. The mucinous epithelium showed no cytological atypia and did not infiltrate into the stromal layer. This stromal layer was consisted of spindle-shaped cells with round to oval nucrei and a small amount of cytoplasm, suggesting the finding for OS. From the immune-histopathological staining, the stromal layer was detected for negative on both estrogen and/or progesterone receptors.
Abdominal CT revealed a multilocular cyctic mass, 6.3 cm in diameter, with wall calcification and no solid component in the pancreatic tail.
Magnetic resonance imaging showed that the cystic lesion was hypointense in T1-weighted imaging (a) and hyperintense in T2-weighted imaging with low intense capsule and septum (b).
Macroscopic findings for removed specimen. The cystic lesion, measuring for 6.5×5.8×5.2 cm in size, was round with a smooth surface and the cut surface demonstrated a multilocular cystic pattern containing thick yellowish mucin, and the lesion was surrounded by a fibrous capsule.
(a) Microscopic findings; low magnification. The pathological procedure showed two distinct components; an inner epithelial layer and an outer densely cellular stromal layer, no cytological atypia in the epithelium and no infiltrate into the stromal layer. (b) Microscopic findings; high magnification. The stromal layer was consisted of spindle-shaped cells with round to oval nucrei and a small amount of cytoplasm, suggesting the finding for OS.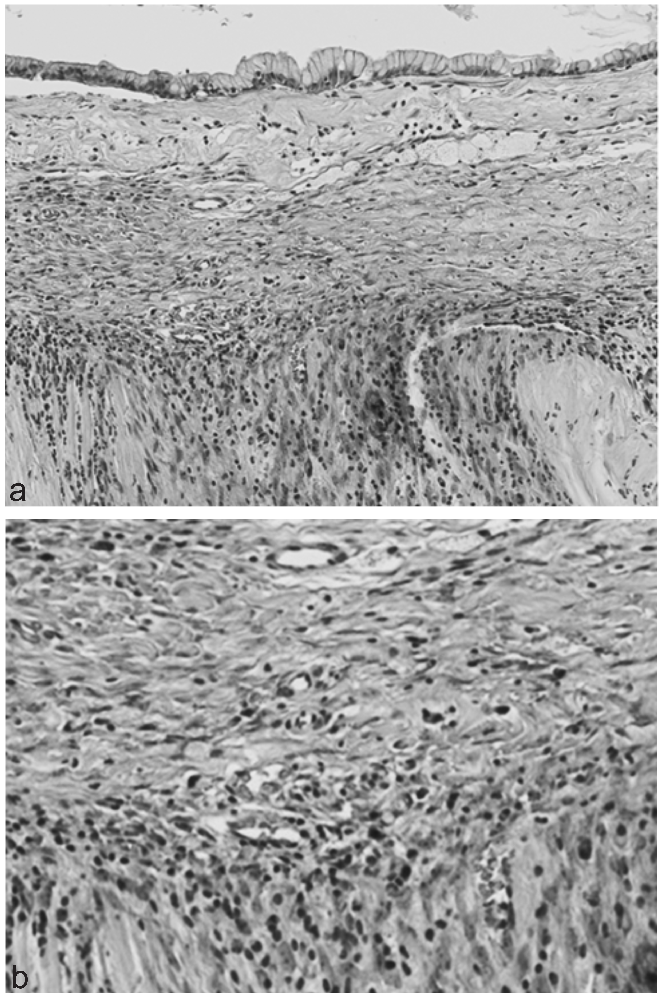
In addition, there was no communication between the cystic lesion and the ductal system. According to these findings, the cystic lesion was diagnosed for MCN of the pancreas. The patient was discharged from the hospital without any events. And, on these 14 months, any recurrence signs have not been detected.
Discussion
Mucin-producing cystic neoplasms of the pancreas have developed a well-recognized entity. In the two decades, due to the utility of high-resolution abdominal imaging techniques, similar cystic lesions of the pancreas are increasingly identified incidentally, 4 and a large number of patients have undergone surgical resection. 5 In 1996, under the aim to describe and categorize the cystic lesions of the pancreas, the WHO classification defined MCN as cystic epithelial neoplasms composed of columnar, mucin-producing epithelium, supported by OS. 6 The OS is known for forming a band of densely packed spindle cells beneath the epithelium; its presence has become a critical requirement as MCN. Then, the MCN was estimated for the different concept from IPMN in the past categories for cystic lesion. And, the Armed Forces Institute of Pathology (AFIP) classification also added the finding for no communication with the pancreas ductal system. 7 Taken together, no doubt to diagnose the present cystic lesion as MCN was detected. Although the developmental process of MCN has not been well understood, it is indicated to originate from remnant primordial gonadal cells that migrated to the pancreas, because the left primordial gonad and dorsal pancreas anlage lie side by side during embryogenesis. 8 The dorsal anlage develops the body and tail of the pancreas; therefore the MCN was frequently raised in the dorsal pancreas and detected in female. Indeed, from the past reports for 130 cases 2 and 56 cases 8 with MCN, no male case has been demonstrated. According to the recent research for pancreas cystic tumors by the Japan Pancreas Society (1992–2001), detected 179 cases with MCN were female in whole. 9 To diagnose the cystic lesion for MCN, the presence of OS pattern should be important; if limiting the tumor with OS but not without OS, all male cases were excluded. 7 Therefore, it is likely that many of the MCN cases reported in male in the early literature were IPMN or other cystic lesion. 1 To the best of our knowledge, 2 male cases with WHO criteria-mediated MCN have been reported for a 43-year-old man in 1998 10 and a 25-year-old man in 2005. 11 Both of them, the cystic lesions were located in pancreas tail, 2.5 cm and 5 cm in size, and the expressions of estrogen/progesterone receptor were demonstrated in stromal component immunohistochemistly. By contrast, the present MCN was found to have neither estrogen nor progesterone receptors. These rare patterns become the originality of MCNs to be unclear, and then further investigations should be continued.
Similar to IPMNs, MCNs have been divided into those with low-grade, moderate grade and high grade dysplasia, and invasive adenocaricinoma. The prevalence of invasive carcinoma reported in MCNs has varied widely in the range of 6–36%.2,8,12 The MCNs are commonly solitary and the recurrence does not occur after complete resection. 13 The biological and clinical behavior of invasive adenocarcinoma arising from the background of cystic neoplasms might be different from the common invasive ductal adenocarcinoma. Infiltrating carcinoma associated with MCNs, and also IPMNs, appears to grow less aggressively and to have a lower incidence of peritoneal and vascular invasion. 14 Then, the patients suffering from malignant cystic neoplasms of the pancreas are likely to get a better for survival after resection than patients with ductal adenocasrcinoma. The patients with ductal pancreatic cancer show around 20% for 5-years survival even after curative resection, while the patients with malignant MCNs demonstrate over 50% for 5-years survival rate. 15 According to the Japan Pancreas Society also, the 5-year survival rate of MCN patients was 100% in adenoma to minimally invasive carcinoma cases, and 57.7% in invasive carcinoma cases. 9 In spite of low grade malignant potential,16,17 a common recommendation should be removal for all mucin-producing neoplasms because of the fear of ultimately developing cancer.2,18 For the surgical procedures, the consideration about not only operative indications but also care for safety might be argued.19,20
Footnotes
Acknowledgments:
the authors thank Dr. Akio Yanagisawa (Kyoto Prefectural University of Medicine, Department of Pathology, Kyoto Japan) for the excellent diagnostic indication from the pathological diagnosis.