
Abstract
Objective
Postpancreatectomy hemorrhage is a life-threatening complication. Hemorrhage occurring >24 hours after the index operation is defined as late hemorrhage. This study was performed to analyze the therapeutic management and prognostic factors of late hemorrhage after pancreatectomy.
Methods
We identified 87 patients with late hemorrhage among 2031 patients who underwent pancreatic surgery from January 2013 to December 2017. The patients’ demographic characteristics, perioperative treatment, hemorrhage details, and prognosis were retrospectively analyzed.
Results
Of the 87 patients, 53 were men. Bleeding occurred at a mean of 8.9 ± 6.0 days postoperatively. Extraluminal and intraluminal hemorrhage occurred in 58 and 29 patients, respectively. The primary intervention was successful in 66 patients, and 16 patients required a secondary intervention. The primary and total recovery rates were 72.4% and 89.7%, respectively. Of the 87 patients, 9 died. Male sex, hemorrhage on a later postoperative day, a significantly decreased hemoglobin level, and pancreatic fistula showed statistical significance as possible risk factors for mortality.
Conclusions
Male sex, hemorrhage on a later postoperative day, a significantly decreased hemoglobin level, and pancreatic fistula are possible risk factors for mortality in patients with late hemorrhage after pancreatectomy. Hemorrhage is a dynamic process, and a secondary intervention may be necessary.
Keywords
Introduction
The mortality rate after pancreatic surgery has substantially decreased during the last several decades. However, the reported morbidity rate remains unacceptably high.1–5 The main causes of surgical morbidity are intra-abdominal infection, pancreatic fistula, delayed gastric emptying, and postoperative hemorrhage.6–9 Although postoperative hemorrhage is rare, it is the most urgent and potentially life-threatening complication, with a high mortality rate ranging from 11% to 36%.2,6,10,11
Postpancreatectomy hemorrhage (PPH) has been defined and classified by the International Study Group of Pancreatic Surgery. 12 Hemorrhage occurring within 24 hours of the index operation is defined as early hemorrhage and is usually the result of technical failure during the operation. In contrast, hemorrhage occurring after 24 hours is defined as late hemorrhage, and it may be associated with pancreatic fistulas, pseudoaneurysms, ulcers, and eroded vessels.10,11,13
Several previous studies have described late hemorrhage; however, the diagnosis, treatment, and prognosis are still controversial and imprecise. The present study was performed to analyze the therapeutic management and prognostic factors of late hemorrhage after pancreatic surgery.
Materials and methods
Patients
A total of 2031 patients underwent pancreatic surgery at our center from January 2013 to December 2017. All medical records were systematically reviewed in detail. The inclusion criteria were major pancreatic resection, late hemorrhage, and treatment at our center after bleeding. Patients with coagulopathy were excluded.
The types of major pancreatic resection performed in this study were pancreaticoduodenectomy, duodenum-preserving pancreatic head resection, distal pancreatic resection, pancreatic segment resection, and total pancreatectomy. Clinical data were collected from both inpatient and outpatient medical records. A retrospective database was constructed, and the patients’ demographic characteristics, perioperative treatments, hemorrhage details, and prognostic data were analyzed.
Perioperative management and surgical technique
All patients underwent a physical examination and computed tomography (CT) scan to assess the feasibility of surgery. The blood coagulation status was assessed preoperatively. Oral laxatives were administered to the patients the day before surgery for bowel preparation. Prophylactic antibiotics were administered via a peripheral vein before anesthetic induction. All patients underwent surgery in the supine position under general anesthesia. Any platelet aggregation inhibitors were discontinued and replaced with low-molecular-weight heparin, which was stopped 12 hours before surgery and continued 24 to 72 hours after surgery. Proton pump inhibitors and somatostatin were administered to all patients immediately after surgery. Amylase activity in the drainage fluid was measured every other day for the first week and every 3 days thereafter until removal of the drains.
The pancreatic resection pattern depended on the tumor location and presence of malignancy. Venous resection and reconstruction were performed if the tumor could not be separated from the superior mesenteric vein or the portal vein. Lymphadenectomy was performed in patients with malignant tumors. The ligamentum teres hepatis was used to embed the pancreatic cut surface during distal pancreatic resection. The gastroduodenal artery stump and splenic artery were routinely ligated with nonabsorbable 4-0 suture and additionally ligated with 2-0 thread. For pancreaticoduodenectomy, reconstruction was performed using Child’s technique. All patients underwent pancreatojejunostomy anastomosis, and no patients underwent pancreatogastrostomy. Manual interrupted sutures were routinely placed after completing the gastrointestinal anastomosis with staples.
Definitions
In this study, both PPH and pancreatic fistula were defined according to the criteria proposed by the International Study Group of Pancreatic Surgery.12,14
PPH (i.e., postoperative hemorrhage after major pancreatic resection) is defined by three parameters: time of onset (early or late), location (intraluminal or extraluminal), and severity (mild or severe). 12 PPH is also graded according to the three above-mentioned parameters and clinical impact. 12 Grade A includes early, intraluminal or extraluminal, mild PPH. Grade B includes early, intraluminal or extraluminal, severe PPH and late, intraluminal or extraluminal, mild PPH. Grade C includes late, intraluminal or extraluminal, severe PPH.
Pancreatic fistula is defined as any measurable volume of drainage fluid with an amylase level of more than three times the upper limit of the reference range for serum amylase on or after postoperative day 3 in association with a clinically relevant condition. 14 A previously described system of three clinical grades of pancreatic fistula was used in this study. 14 According to this system, biochemical leakage (grade A) is no longer considered a true pancreatic fistula. Grade B requires a change in postoperative management (persistent drainage for >3 weeks, percutaneous or endoscopic drainage, clinically relevant change, angiographic procedures for bleeding, or signs of infection without organ failure). Grade C is defined as organ failure, reoperation, or mortality attributable to the pancreatic fistula.
Statistical analysis
Linear variables are presented as mean ± standard deviation, and categorical variables are presented as absolute number or frequency. Differences between the study groups were analyzed using the χ2 test, Fisher’s exact test, or Student’s t-test as appropriate. All statistical analyses were performed using the Statistical Package for the Social Sciences software version 25.0 (IBM Corp., Armonk, NY, USA). A p-value of <0.05 was considered statistically significant.
Ethics
All patients or their legal guardians provided written informed consent for the surgical procedures performed, and the study was approved by the Peking Union Medical College Hospital Institutional Review Board for studies in humans (S-K1133). The requirement of informed consent for the publication of data was waived because of the retrospective nature of the study.
Results
Of the 2031 patients who underwent pancreatic surgery from January 2013 to December 2017 at our hospital, 87 patients (4.3%) with late PPH were included in the analysis (Figure 1). Of these 87 patients, 53 were men (60.9%) and 34 were women (39.1%), and their mean age was 57.2 ± 13.2 years (range, 24–81 years). Details regarding the pathologic diagnoses and surgical procedures are shown in Table 1. Malignancy was the indication for surgery in 62 patients (71.3%), and 63 patients (72.4%) underwent pancreaticoduodenectomy or total pancreatectomy. Bleeding occurred at a mean of 8.9 ± 6.0 days (range, 2–26 days) after surgery. All patients except one developed late PPH during the first hospital stay. The mean length of hospital stay was 41.4 ± 26.5 days (range, 7–214 days). Twenty-seven patients developed a postoperative pancreatic fistula (grade B and C in 14 and 13 patients, respectively).

Flow diagram of inclusion criteria. Of the 309 patients who did not undergo major pancreatic resection, 234 underwent resection of pancreatic neuroendocrine tumors, 62 underwent internal drainage of pancreatic pseudocysts, and 13 underwent debridement and external drainage of pancreatic abscesses.
Pathologic diagnoses and surgical procedures in patients with late postpancreatectomy hemorrhage.

PD: pancreaticoduodenectomy, TP: total pancreatectomy, DPPHR: duodenum-preserving pancreatic head resection, DPR: distal pancreatic resection, PSR: pancreatic segment resection, TG: total gastrectomy.
Fifty-eight patients with late PPH developed abdominal discomfort and bleeding from the surgical drain with low blood pressure, and they were considered to have extraluminal hemorrhage. The remaining 29 patients developed melena, hematemesis, or bleeding from the nasogastric tube, and they were considered to have intraluminal hemorrhage. Blood tests were performed in all patients to confirm the hemorrhage and assess the severity of bleeding. The hemoglobin level decreased by ≥30 g/L in 46 patients. All of these patients had clinical symptoms such as hypotension, tachycardia, dizziness, and thirst, and they were classified as having grade C PPH.
All patients underwent fluid resuscitation, electrocardiographic monitoring, and oxygen inhalation immediately after the diagnosis of PPH, and they were strictly confined to their hospital bed. Invasive treatment was performed when the initial conservative treatment was ineffective. A secondary intervention was performed when the primary intervention failed. In patients who underwent angiography, the vascular sheath was introduced through either the left or right common femoral artery, and a 5-Fr angiographic catheter was navigated at the celiac artery; angiography was then performed to identify the culprit lesion. A microcatheter was navigated into the bleeding site, and spring coils and Gelfoam particles (Pfizer, New York, NY, USA) were used to embolize it. In patients who underwent endoscopy, gastroscopy was performed under deep sedation or general anesthesia. The gastrointestinal anastomosis and stomach were carefully examined. Injection and mechanical hemostatic clips were used to control the bleeding if the culprit lesion was found. In patients who underwent a reoperation, the surgical principles were hemostasis and damage control by removal of the hematoma, simple ligation or repair of the bleeding site, external drainage, and reconstruction of the anastomosis if possible. The detailed approaches and treatment outcomes are presented in Table 2. Of the 58 patients with extraluminal hemorrhage, 45 recovered after the primary intervention (conservative treatment, n = 29; operation, n = 7; angiography, n = 9), 7 recovered after the secondary intervention (reoperation or operation), and 6 died. The primary and total recovery rates were 77.6% (45/58) and 89.7% (52/58), respectively. Of the 29 patients with intraluminal hemorrhage, 21 recovered after the primary intervention (conservative treatment, n = 13; operation, n = 2; angiography, n = 1; endoscopy, n = 5), 5 recovered after the secondary intervention (operation), and 3 died. The primary and total recovery rates were 72.4% (21/29) and 89.7% (26/29), respectively.
Treatments and outcomes in patients with late postpancreatectomy hemorrhage.

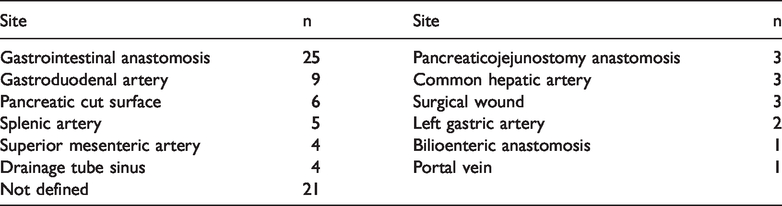
Endoscopy, angiography, CT, and clinical examinations were performed to detect the bleeding sites. The source of the bleeding could be identified in 66 patients; the remaining 21 patients had extraluminal hemorrhage and were cured after conservative treatment (Table 3). Gastrointestinal anastomosis was the most common bleeding site (25 patients [28.7%]). Nine patients (10.3%) died despite timely treatment. The detailed data and statistical differences between the patients who survived and those who died are presented in Table 4. The sex distribution, postoperative day of hemorrhage, decreased hemoglobin level, and presence of a pancreatic fistula were significantly different between the two groups (p < 0.05).
Bleeding sites in patients with late postpancreatectomy hemorrhage.
Comparison between patients who survived and died after PPH.
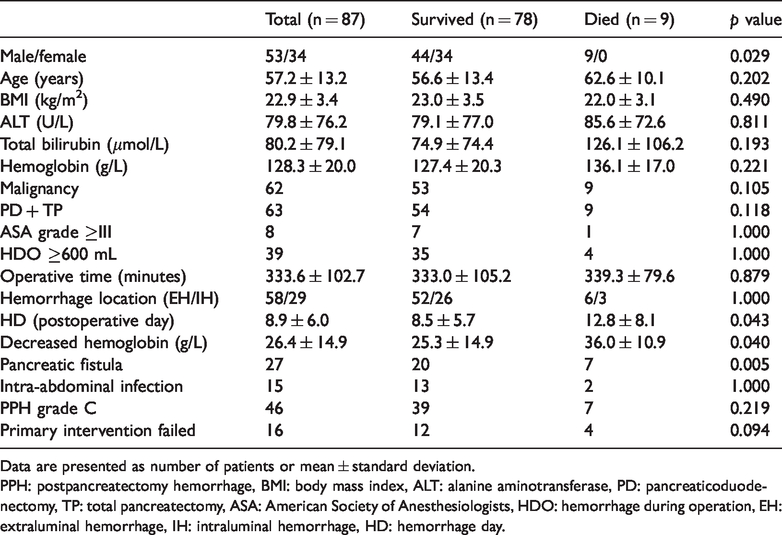
Data are presented as number of patients or mean ± standard deviation.
PPH: postpancreatectomy hemorrhage, BMI: body mass index, ALT: alanine aminotransferase, PD: pancreaticoduodenectomy, TP: total pancreatectomy, ASA: American Society of Anesthesiologists, HDO: hemorrhage during operation, EH: extraluminal hemorrhage, IH: intraluminal hemorrhage, HD: hemorrhage day.
Discussion
Pancreatic resection is a demanding surgery, even in experienced centers, because of both the challenging operative technique and the need to manage complications. Emergency relaparotomy is more common in patients with PPH than in patients with other complications, such as a pancreatic fistula, intra-abdominal infection, or delayed gastric emptying. A median PPH rate of 5.9% was reported in a systematic review of a large number of patients. 15 Additionally, mortality and morbidity rates have been shown to be high in patients with PPH. 16 Thus, PPH should be considered a critical complication.
It is very difficult to precisely define late hemorrhage, and definitions vary among different studies. A clear, concise, and quantifiable characterization of PPH had been lacking until the International Study Group of Pancreatic Surgery presented its definition and classification in 2007. 12 The threshold is considered to be 24 hours after the index operation. In the present study, we adopted this definition and found an incidence of 4.3%. In our series, most patients with late PPH had malignant tumors (71.3%) and underwent pancreaticoduodenectomy or total pancreatectomy (72.4%). Both of these characteristics have been previously reported as risk factors for PPH.17,18
For patients with early PPH, routine reoperation is recommended to avoid polytransfusion and treatment delays.10,11,13 However, the optimal treatment for late PPH is controversial, and the choice mainly depends on the clinical presentation. 19 Once late PPH has been diagnosed or suspected, the first step is to assess whether the patient is stable. Reoperation should be performed in unstable patients. If the hemodynamic condition is stable, angiography, endoscopy, or CT should be performed in addition to conservative therapy to identify the bleeding sites. Identification of the bleeding sites is very useful to determine the appropriate treatment. Because hemorrhage is a dynamic process, assessment of the patient’s condition should also be a dynamic process.
Unstable patients usually have major bleeding events, such as active arterial and anastomotic bleeding. Laparotomy may be the only approach to rescue these patients. The choice of the surgical procedure is important for emergency surgery, and simple operations with a low risk of injury are preferred. Completion pancreatectomy is very complex because of the modified anatomy, postoperative adhesions, and inflammatory reactions. Some researchers have even attempted to use special drainage instead of completion pancreatectomy.20,21 Because of the significant operative trauma associated with laparotomy, it is not the first choice in hemodynamically stable patients, and several different procedures may be used instead.
Arteriography with embolization is used worldwide because of its minimal invasiveness. It avoids damage to other organs and is superior to reoperation in terms of survival. 22 As time progresses after pancreatic surgery, the probability of anastomotic bleeding decreases and that of visceral arterial bleeding increases. The use of modern radiological equipment and technology for treatment of visceral arterial bleeding has a high success rate. Thus, angiography is especially suitable for patients with late PPH, and it has been recommended in several previous studies.23–27 Arteriography with embolization can be used as a temporary hemostatic measure to gain sufficient time for the next operation. Even if the procedure fails, the bleeding site can still be identified, which is crucial for the subsequent operation. To make the patient’s condition more suitable for embolization, surgeons should suture-ligate and dissect the gastroduodenal artery as far as possible from the common hepatic artery during the first operation, thereby creating enough space for embolization. In contrast, angiography is not appropriate when bleeding is intermittent, diffuse, or venous. Endovascular treatment is only suitable for hemodynamically stable patients. 28 In the present study, angiography was performed in 16 patients with extraluminal hemorrhage and 4 with intraluminal hemorrhage during the primary intervention. Nine patients in the first group and one patient in the second group recovered.
Endoscopy is a direct diagnostic procedure in patients with intraluminal hemorrhage. Endoscopic therapy can be performed immediately after identification of the bleeding site. Endoscopy is useful for suspected gastrointestinal hemorrhage, but it might show false-positive results and delay treatment for actual causes of bleeding. 13 In addition, upper endoscopy is not recommended for the first several postoperative days to protect the pancreatoenteric and bilioenteric anastomoses. Although the use of endoscopy is limited, it is useful to exclude intraluminal bleeding and treat bleeding in selected patients. In the present study, endoscopy was performed in seven patients with intraluminal hemorrhage, and five of these patients recovered completely. In the remaining two patients, the bleeding sites were not detected, and they underwent surgery as a secondary intervention. A previous study showed that endoscopy could detect the bleeding site in only 25% of patients who underwent pancreaticojejunostomy. 29
In the present study, the primary recovery rates for extraluminal and intraluminal hemorrhage were 77.6% and 72.4%, respectively. Among the 21 patients who did not recover, 5 died (3 with extraluminal hemorrhage and 2 with intraluminal hemorrhage), and the remaining 16 patients did not achieve successful outcomes and required a secondary intervention. Surgery was the approach used for the secondary intervention, and 12 patients were ultimately rescued. Thus, the overall recovery rate was 89.7%, which was considered acceptable. When the primary treatment is ineffective, it is very important to initiate alternative therapy.
Most cases of PPH originate from the visceral arteries and gastrointestinal tract. In our series, gastrointestinal anastomoses were the most common bleeding sites, followed by the gastroduodenal artery. Several surgical techniques can be used to avoid such bleeding. After completing the gastrointestinal anastomosis with staplers, manual interrupted stitching is recommended. In addition, the ligamentum teres hepatis can be used to embed the pancreatic cut surface. In four patients, the drainage tube sinus was the bleeding site. If the drainage tube is left in the body for an extended period, friction may occur with the surrounding sinus during walking, turning over, and lying down. Therefore, the drain should be removed as early as possible if the patient’s condition allows. In line with the findings of a previous study, 19 the exact bleeding sites were unknown in some patients with non-severe PPH who underwent conservative treatment. Their bleeding sites were likely within the surgical wound and small veins.
The mortality rate of late PPH could be as high as 30%. 30 In the present study, nine patients (10.3%) died. The high mortality rate of late PPH can be attributed to diagnostic difficulties and sudden bleeding onset. As shown in Table 4, male sex, bleeding on a later postoperative day, a significantly decreased hemoglobin level, and a pancreatic fistula were possible risk factors for mortality. Previous studies have shown that a pancreatic fistula is a risk factor for PPH,17,30,31 possibly because of subsequent local sepsis. The fistula may erode the anastomotic site and vascular wall. The vessels are usually skeletonized and ligatured at the arterial end stump, most commonly in patients with malignancy requiring lymphadenectomy during radical resection, and this is a potential cause of acute arterial bleeding and pseudoaneurysm development. Acute arterial bleeding and pseudoaneurysm rupture can result in death, and their effects are more pronounced over time. Thus, the occurrence of a pancreatic fistula and delayed postoperative bleeding are possible risk factors. If a pancreatic fistula has already been diagnosed, the patient should be followed closely and carefully to avoid late PPH and death. A significant decrease in the hemoglobin level indicates severe bleeding, which is more life-threatening than mild bleeding. However, the mechanisms underlying an increase in the mortality rate among men are unclear.
The present study has some limitations. First, because of the retrospective nature of this study, the patient volume, registration information, and variables assessed could not be determined beforehand. Second, there was no control group. Third, arteriography and endoscopy were not routine procedures after PPH, and this may have caused some bias. Fourth, a multivariate analysis was not applicable because of the small sample size and mortality rate, and such an analysis was not performed on the potential risk factors for PPH mortality. Prospective, observational, and multicenter clinical trials are required to obtain more robust and reliable findings.
In conclusion, late PPH is a severe complication of pancreatic surgery, and gastrointestinal anastomosis is the most common bleeding site. The mortality rate is high because of diagnostic difficulties and sudden bleeding onset. Male sex, bleeding on a later postoperative day, a significantly decreased hemoglobin level, and a pancreatic fistula are potential risk factors for mortality. Laparotomy, angiography, and endoscopy are suitable treatments for different situations. Alternative therapy should be initiated when the primary treatment is ineffective. Low mortality rates can only be achieved with timely recognition and suitable intervention.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Xin Wu and Ge Chen designed the study. Xin Wu, Wenming Wu, Taiping Zhang, Quan Liao, and Menghua Dai analyzed the data and drafted the manuscript. Ge Chen, Wenming Wu, and Yupei Zhao revised the manuscript for important intellectual content. All authors approved the final manuscript.