
Abstract
Langerhans cell sarcoma of the skin is a rare tumor with aggressive behavior. There are reports of Langerhans cell sarcoma involving the skin in patients with underlying systemic Langerhans cell histiocytosis. However, to our knowledge, sarcomatous transformation of skin Langerhans cell histiocytosis, has not been previously described. We report a case of Langerhans cell sarcoma of the skin representing a probable transformation from Langerhans cell histiocytosis. The lesion had a clinical and pathological biphasic pattern, presenting as a plaque and nodule in the lower leg of a 66 year-old female. The plaque area showed a superficial epidermotropic proliferation of atypical Langerhans cells. The associated deep nodule had an overtly sarcomatous Langerhans cell proliferation. The immunohistochemistry profile was characteristic of Langerhans cells in both components. We consider this case a unique example of deep nodular Langerhans cell sarcoma of the skin, in which the associated superficial Langerhans cell proliferation is consistent with the precursor lesion.
Introduction
Langerhans cell sarcoma was first described as a multisystemic aggressive process termed malignant histiocytosis X.1,2 Few cases of primary cutaneous Langerhans cell sarcoma have been reported. 3 Unlike other neoplastic processes, the association of a precursor lesion and transformation into a overtly malignant process has been elusive in Langerhans cell sarcoma. A case of pulmonary malignant Langerhans cell transformation in the lung, 4 and association of Langerhans cell sarcoma with systemic histiocytosis X have been reported. 5 We report here a case of deep nodular Langerhans cell sarcoma arising in association with a superficial plaque of Langerhans cell proliferation, consistent with the precursor lesion.
Case Report
The patient is a 66 year old female, who presented with a rapidly growing 3×1.5 cm reddish plaque on the anterior distal left lower leg. Beneath the distal portion of the plaque there was a 1 cm hard, deep and relatively well circumscribed, spherical nodule (Figure 1). Separate biopsies were obtained from both the plaque area and from the deep nodule. Histological evaluation of the biopsy from the plaque showed a superficial proliferation of atypical mononuclear cells with epidermotropism (Figure 2A). Melanocytic, B-cell lymphocytic, and epithelial markers were negative. The cells in both the superficial and deep component had the characteristic features described in proliferations of Langerhans cells, 6 but exhibited cytologic atypia. The cells from the deep nodule exhibited marked atypia, areas of necrosis and abnormal mitoses (Figure 2B-D), as has been described in overtly malignant Langerhans cell tumors. 7 Immun histochemistry studies performed in both biopsies showed markers typical of Langerhans cells, including expression of CD1a (Figure 3A,B), S-100, CD68, CD4 and CD45. CD30 is expressed in both the superficial and deep components (Figure 3C,D), with the highest expression in the superficial component. CD3 is expressed in both the superficial (Figure 4A) and the deep component (Figure 4B). CD207 (Langerin) is expressed in the superficial component (Figure 4C) but not in the deep component (Figure 4D). Beta and Gamma T-cell receptor monoclonality was not detected by PCR in neither the superficial or deep components. No BRAF gene mutation was detected by PCR, which was performed on both specimens.

Clinical photo of the lesion prior to biopsy. Arrow indicates the biphasic lesion composed of a plaque and nodule on the anterior distal left lower leg.
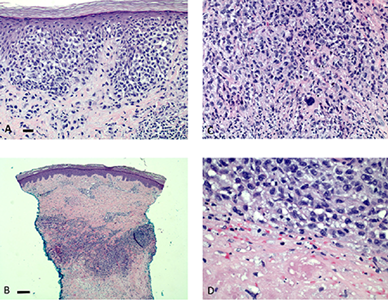
Histology of the lesion. The plaque (A) shows atypical Langerhans cells with epidermotropism. The nodular lesion, without epidermotropism (B) shows highly atypical Langerhans cells (C) and tumor necrosis (D). Bar: Approximately 50 microns in A, C and D and 500 microns in B.

Immunohistochemistry of the lesion showing CD1a expression in both the superficial atypical Langerhans cells from the plaque (A) and in the highly atypical deep tumor cells (B). CD30 is expressed in the superficial component (C) and focally in the deep component (D). Bar: Approximately 100 microns in A, B, C and D.

Immunohistochemistry of the lesion showing CD3 expression in both the superficial atypical Langerhans cells from the plaque (A) and in the highly atypical deep tumor cells (B). Langerin is expressed in the superficial component (C) but not in the deep component (D). Bar: Approximately 100 microns in A,B,C and D.
Materials and Methods
The biopsies were processed by routine tissue histology methods. Immunohistochemistry was performed at Miraca Life Sciences with appropriate controls using a Benchmark Ultra Ventana automated stainer, Ventana Medical Systems, Inc., Tuczon, AZ. The antibodies were from Cell Marque, Rocklin, CA., and Ventana Medical Systems, Inc., Tuczon, AZ. Immunohistochemistry for Langerin was performed at Associated Regional and University Pathologists, Inc. (ARUP), Salt Lake City, UT. Beta and Gamma T-cell receptor clonality and BRAF gene mutation analysis was performed by PCR on both specimens at Miraca Life Sciences, Phoenix, AZ.
Discussion and Conclusions
Langerhans cell sarcoma may arise in the skin as a primary cutaneous neoplasm,3,8 or represent a cutaneous manifestation of a systemic malignant process.9–11 In either condition, understanding the process of malignant transformation in Langerhans cell neoplasms has proven difficult, and few cases have reported a bona fide precursor lesion. 4 In addition, the neoplastic transformation of Langerhans cells is even more complex given the potential of different cell progenies to acquire phenotypic and immunologic features of Langerhans cells by mechanisms known as clonal plasticity and trassdifferentiation.12–15 The process of clonal plasticity and transdifferentriation may explain the expression of CD30 and CD3 in our case. However, there are lesions described as resembling Langerhans cell histiocytosis, some of which may be neoplastic or reactive, in association with lymphoproliferative disorders. 16 There is also a published report of a CD30 positive anaplastic large-cell lymphoma mimicking Langerhans cell histiocytosis. 17 In contrast to that report, the absence of T-cell clonality in our case supports the process of clonal plasticity and transdifferentiation of a Langerhans cell malignant neoplasm rather than a T-cell lymphoma mimicking a Langerhans cell process. This mechanism may explain the CD3 positivity seen in our case. Supporting this premise, there is a report of cytoplasmic CD3 expression in Langerhans cell sarcoma. 18 However, although CD1a is expressed in both the superficial and the deep component, it is noticeable the absence of Langerin in the deep component of the lesion. This observation opens the possibility of malignant Langerhans proliferations with loss of characteristic Langerhans cell markers, or malignant proliferations with multipotential pathways towards lymphoid and Langerhans cell differentiation. The limited number of cases and the lack of known carcinogenetic events adds to the poor understanding of this disease. 19 Although our case does not clarify the mechanism of sarcomatous transformation, the presence of a superficial proliferation consistent with a precursor lesion suggest that certain Langerhans cell proliferations may have the potential for becoming an aggressive neoplasm. Although BRAF gene mutation analysis performed on both biopsy specimens found no mutation, only 50-60% of cases demonstrate a mutation. 20 Reevaluation of the multiple variants of Langerhans cell histiocytosis may prove helpful in determining the steps of malignant transformation, as it has been for other epithelial, hematopoietic and mesenchymal neoplasms.
Footnotes
Acknowledgements
We thank Carolyn Ng and Rosa Gonzales at Miraca Life Sciences, Union, NJ., for their expert immunohistochemistry technical work.