
Abstract
Recurrent respiratory papillomatosis is a benign neoplastic growth of the respiratory system, often linked to human papillomavirus types 6 and 11. This case report presents a rare progression to severe airway obstruction and potential malignancy in a 59-year-old male with a history of smoking, hepatitis B carrier status, pulmonary tuberculosis, and a tracheal papilloma. Initially hospitalized for right upper lobe pneumonia, a computed tomography scan revealed a bronchial tumor. Bronchial brushing, washing, and biopsy confirmed squamous cell papilloma. Treatment included bronchoscopy with argon plasma coagulation ablation and debulking surgery for the right upper lobe bronchus and airway tumor; however, recurrence was noted on a follow-up computed tomography scan. Repeat bronchoscopy with argon plasma coagulation ablation confirmed squamous cell papilloma with squamous cell carcinoma in situ. The patient was administered human papillomavirus vaccination to mitigate disease progression and remains under active surveillance. This paper highlights a rare malignant transformation of airway recurrent respiratory papillomatosis.
Introduction
Recurrent respiratory papillomatosis (RRP) is a rare disease characterized by recurrent wart-like growths along the respiratory tract, caused by human papillomavirus (HPV) types 6 and 11. It is more prevalent in children; however, the exact mechanisms of viral transmission remain incompletely understood. Vertical transmission through contact with infected secretions in the birth canal has been proposed as a potential route in juvenile-onset RRP, but current evidence is limited, and this mechanism alone does not fully explain observed epidemiological patterns.
In adults, HPV infection has been associated with sexual transmission, including oral–genital contact; however, this association remains controversial and does not account for all reported cases. Emerging evidence suggests that HPV transmission in RRP may involve multiple pathways, including non-sexual transmission, autoinoculation, and possible latent viral reactivation. Overall, the routes of infection in both juvenile- and adult-onset RRP are likely multifactorial and remain to be fully elucidated.
While RRP rarely leads to malignant transformation, it can cause airway obstruction in a subset of patients. Intrapulmonary dissemination refers to the spread of papillomatous lesions into the lower respiratory tract and lungs, representing a rare but particularly challenging manifestation of the disease and complicating clinical management. Treatment options for intrapulmonary dissemination have demonstrated only limited efficacy, underscoring the need for further clinical experience and investigation of novel therapeutic strategies.
We present a case of RRP and malignant change who is now under our treatment. This case report is reported in accordance with the CARE guidelines (Supplemental Material).
Case presentation
A 59-year-old male with a history of smoking, hepatitis B carrier status, and prior pulmonary tuberculosis was diagnosed with tracheal papilloma at another hospital, without surgical intervention. On January 3, 2023, he was admitted to Taipei Municipal Wanfang Hospital for fever and a productive cough. Computed tomography (CT) revealed right upper lobe (RUL) pneumonia and a bronchial tumor (Figure 1). Bronchial brushing, washing, and biopsy, which revealed squamous cell papilloma (Figure 2). Treatment included bronchoscopy with argon plasma coagulation (APC) ablation and debulking surgery targeting the RUL bronchus and airway tumor (Figure 3). Follow-up CT scans conducted at 6 months and 1 year post-surgery indicated recurrence and disease progression, respectively. Repeat bronchoscopy with APC ablation of the RUL bronchus and tracheal tumor was performed (Figure 4). Pathology findings indicated squamous cell papilloma with squamous cell carcinoma in situ (Figure 5 and Table 1).
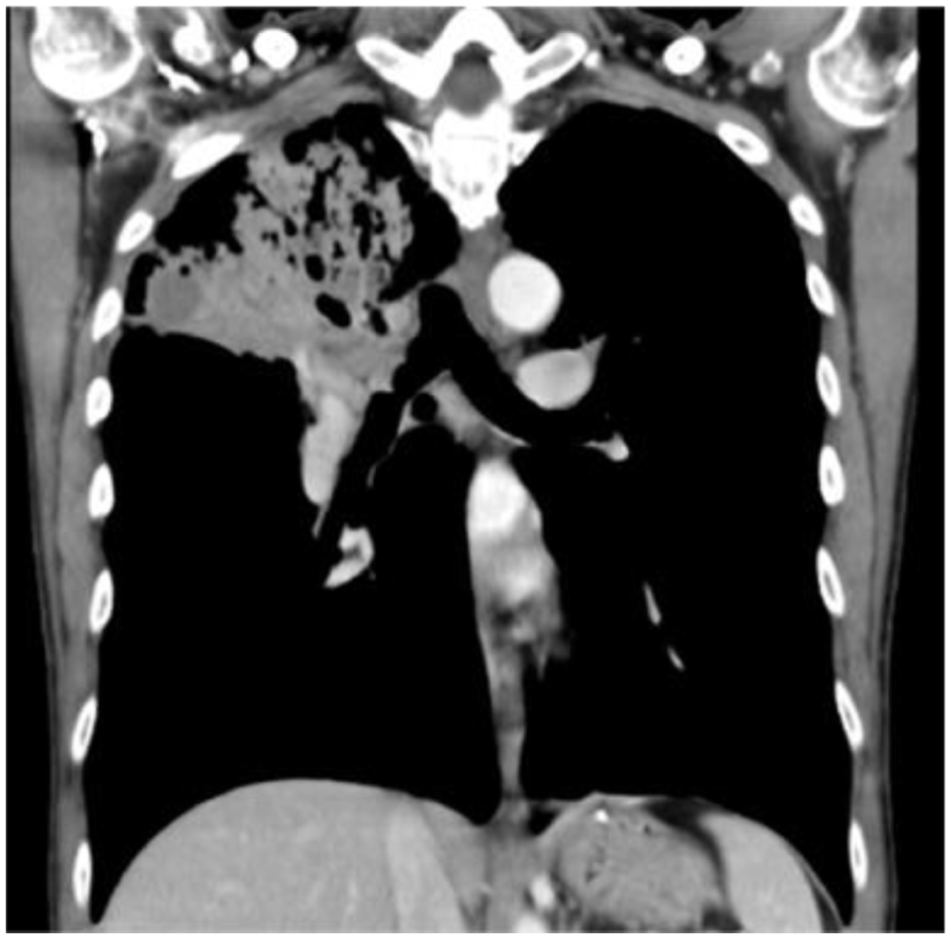
Coronal view of computer tomography showed tumor obstruction at right main bronchus with pneumonia.

Pathology collected through bronchoscopy biopsy; respiratory papillomatosis was found.

Respiratory papillomatosis tumor resection was done through argon plasma coagulation.
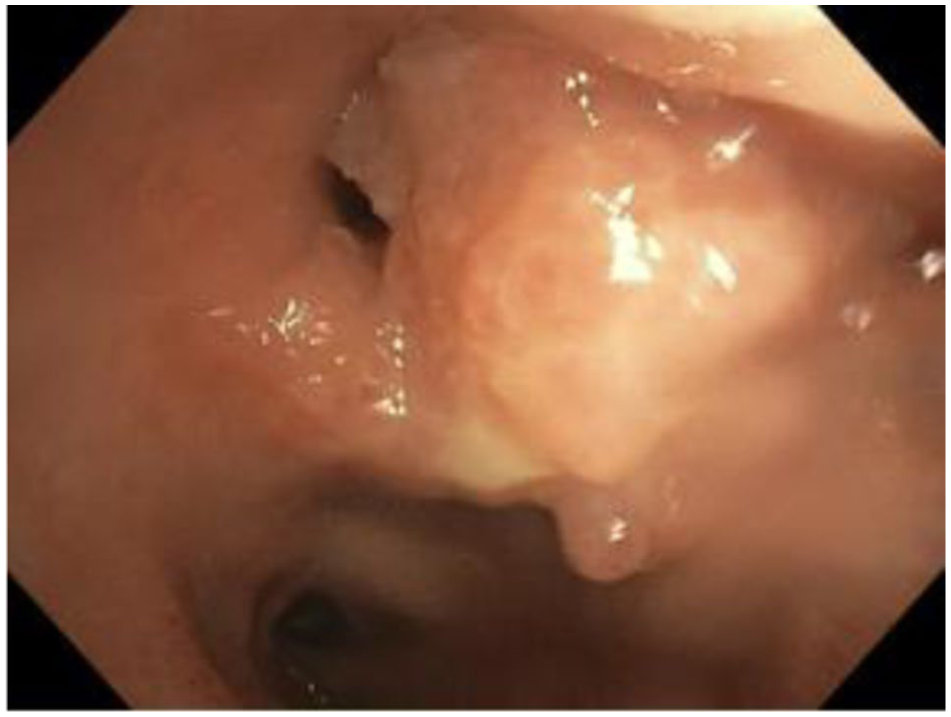
Intra-lumen tumor, found through bronchoscopy. Argon plasma coagulation tumor resection was done as the following surgery. Tissue was collected for pathology.
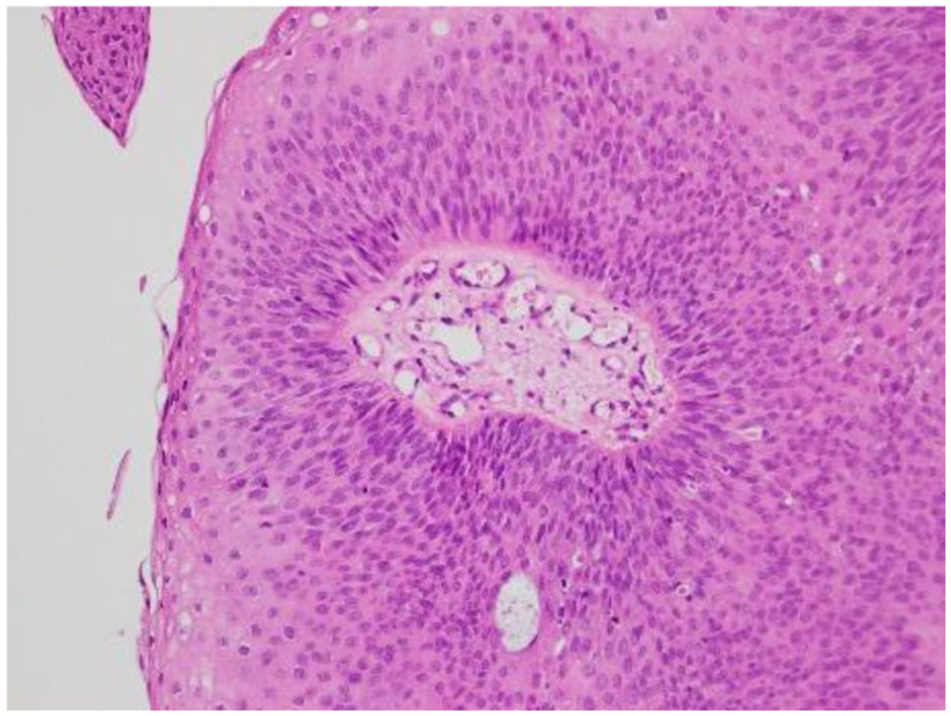
Recurrent respiratory papillomatosis with malignant changes was found through pathology.
The examinations and pathology findings we arranged to diagnose the patient’s disease and treat his disease.
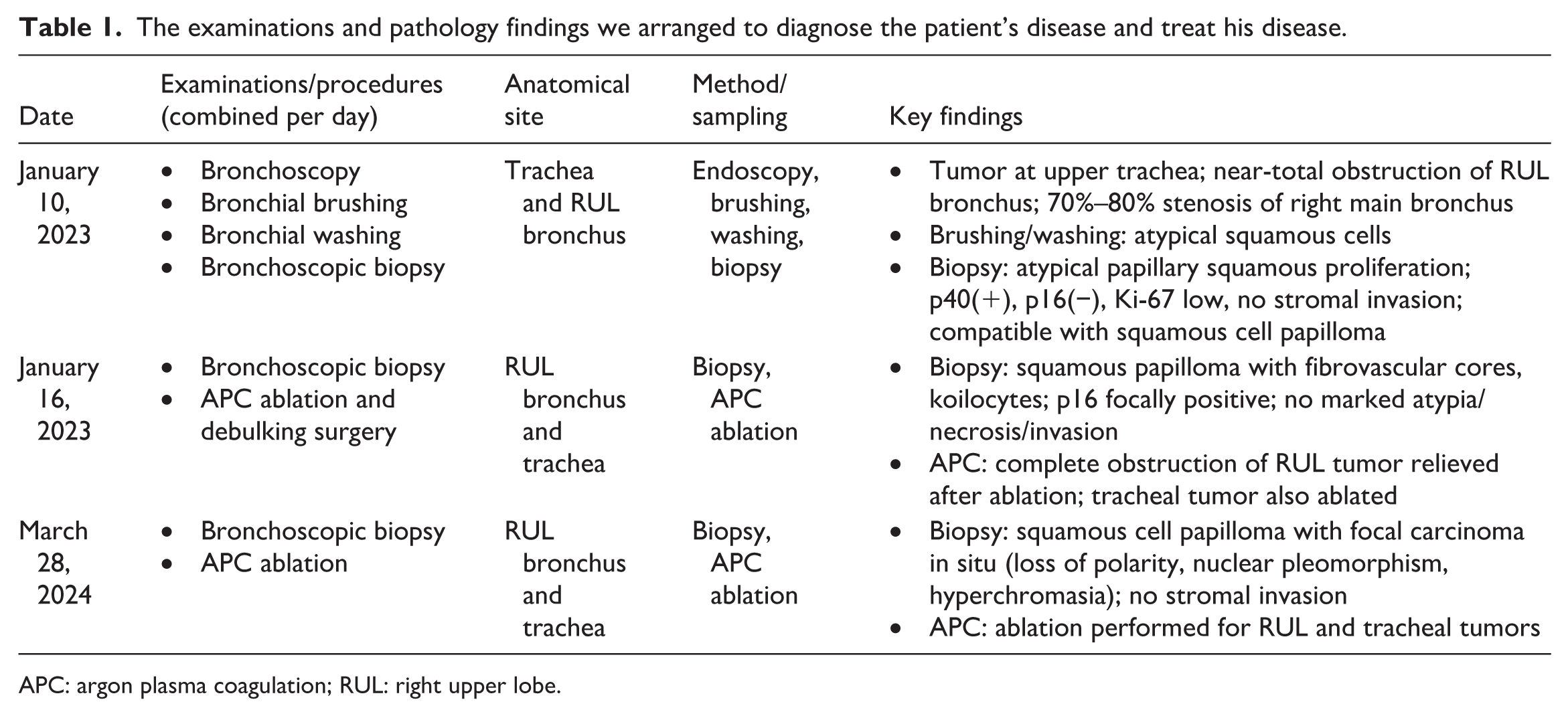
APC: argon plasma coagulation; RUL: right upper lobe.
Consequently, a vaccine for HPV was administered to mitigate disease progression. We arrange CT image and bronchoscope examination to follow-up disease progress after treatment every half year, and arrange surgical resection if there are positive findings on CT. CT found RUL bronchus and trachea squamous papilloma post-debulking surgery, a stationary extent of airway and lung nodular lesions with emphysema and atelectasis. No recurrence and no new airway lesion were found through bronchoscopy. The patient remains under active surveillance.
Discussion
This case highlights diagnostic and therapeutic challenges in tracheobronchial RRP with histologic progression to carcinoma in situ. Tracheobronchial involvement represents a more aggressive disease phenotype and is associated with increased morbidity and procedural burden compared with laryngeal-limited disease.1,2 Serial bronchoscopic examinations with correlated pathology in the present case support stepwise neoplastic progression rather than misclassification at initial diagnosis, although sampling bias cannot be entirely excluded.
Primary involvement of the tracheobronchial tree without synchronous upper aerodigestive tract lesions is uncommon in RRP. Delayed recognition of proximal disease or under-sampling of the larynx during earlier evaluations may account for this rare presentation.1,2 Such atypical disease distribution underscores the importance of comprehensive endoscopic assessment of the entire aerodigestive tract at diagnosis and during follow-up.
Malignant transformation in RRP is infrequent, reported in ~1%–4% of adult cases, but remains a clinically significant concern.3,4 Risk factors for malignant change include long-standing disease, smoking, prior radiation exposure, and persistent HPV infection, particularly HPV-11, which has been associated with more aggressive disease behavior and distal airway involvement.2,5 In the present case, HPV genotyping was not performed, representing a major limitation and precluding genotype-specific risk stratification.
With regard to management, repeated endoscopic debulking remains the mainstay for maintaining airway patency in tracheobronchial RRP. 2 Various adjuvant therapies have been proposed to reduce recurrence and disease burden, including intralesional agents and systemic therapies such as bevacizumab, although evidence is largely derived from observational studies and small series. 6 Prophylactic HPV vaccination has recently been explored as an adjuvant strategy in patients with established RRP, with retrospective data suggesting a reduction in disease burden and surgical frequency following vaccination. 7 However, given the retrospective nature of these studies, causal inference cannot be established, and the potential therapeutic benefit of vaccination should be interpreted cautiously.
Surveillance strategies for tracheobronchial RRP with dysplasia or carcinoma in situ have not been standardized. Regular bronchoscopic evaluation with targeted biopsies, supplemented by interval chest imaging to assess distal airway and pulmonary involvement, represents a pragmatic approach based on current clinical practice and expert opinion. 2 Multidisciplinary management involving pulmonology, thoracic surgery, pathology, and oncology is essential to balance airway preservation with oncologic vigilance in patients at risk for malignant progression.
Limitations
The present report has several limitations. Most notably, HPV genotyping was not performed. Given the well-established genotype-specific differences in disease behavior and malignant potential in RRP, the lack of virological characterization represents a significant limitation and constrains etiologic inference in this case. In addition, as with all single-case reports, causal relationships between interventions and outcomes cannot be established.
Conclusion
This case highlights the diagnostic and therapeutic challenges of tracheobronchial RRP with histologic progression to carcinoma in situ. Careful longitudinal documentation with serial bronchoscopic examinations and correlated pathological assessment is essential to support neoplastic progression and to guide timely intervention in patients with airway involvement. Given the risk of recurrence and potential for malignant transformation, individualized surveillance strategies incorporating regular endoscopic evaluation and interval imaging are warranted. While adjuvant measures such as HPV vaccination may be clinically reasonable in selected patients, causal inferences regarding therapeutic efficacy should be avoided in single-case observations. Multidisciplinary management and long-term follow-up remain crucial to optimize airway patency and clinical outcomes in this rare but potentially aggressive disease.
Supplemental Material
sj-docx-1-sco-10.1177_2050313X261436099 – Supplemental material for Rare case of recurrent respiratory papillomatosis with malignant transformation
Supplemental material, sj-docx-1-sco-10.1177_2050313X261436099 for Rare case of recurrent respiratory papillomatosis with malignant transformation by Kae-Feng Yang, Wei-Cheng Lin and Yin-Chun Chang in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
The authors would like to thank all colleagues and students who contributed to this study. We are grateful to Dr. Yin-Chun Chang and Dr. Wei-Cheng Lin for their advice during treatment and for composing the article. We thank the editors for constructive criticisms of an earlier version of this case report.
Ethical considerations
Taipei Medical University Joint Institutional Review Board (N202506118/2025.09.08).
Consent to participate
We informed the patient that his data and pathology will be used as research, and the patient agrees with his data and image being used as research. The form will be uploaded as a supplementary file.
Consent for publication
Written informed consent was obtained for anonymized patient information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Available upon request from corresponding author due to ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.