
Abstract
Colorectal carcinomas (CRC) were initially thought to be rare in Africa including Nigeria, but recent studies have shown a reverse trend in our environment. This study is aimed to identify the clinical and pathological characteristics of CRC diagnosed between July 2006 and June 2015 in the University of Uyo Teaching Hospital, and a Private Specialist Laboratory, Uyo, Akwa Ibom State, Nigeria. All histological diagnosed cases of CRC seen in the two laboratories (University teaching and a private facility) in Uyo, Akwa-Ibom state, Nigeria during the study period were retrieved noting their bio-data, pathological and clinical variables. A total of 45 patients of age range 26-80 years with a mean of 55.9 years (SD 3.9) and a male to female ratio of 1.4:1 were seen. The two most common age groups affected in CRCs were 61-70 years (28.9%) and 51-60 years (24.4%) respectively. Majority of CRC patients were older than 40 years (86.7%) with identifiable predisposing factors being tubulo-villous adenoma (4 cases, 8.8%), villous adenoma (2 cases 4.4%), polyposis syndromes (2 cases, 4.4%) and schistosomiasis (1 case, 2.2%). Features of large intestinal obstruction were the most common presenting symptom of CRC (53.3%). Rectal bleeding, alteration in bowel habit and fecal incontinence were other symptoms, accounting for 33.3%, 8.9% and 4.4% of cases respectively. Left-sided CRCs were commoner (68.9%) with the majority appearing as annular-constricting type macroscopically (60.0%). Recto-sigmoid region was the preponderant site involved in CRC (29 cases, 64.5%). Adenocarcinoma (84.4%) was the most frequent histological subtype. Mucinous carcinoma, signet ring carcinoma and carcinoid tumor were other histologic subtypes seen in 8.9, 4.4 and 2.2% of cases respectively. The 22.0% of CRC patients presented at advanced stages of the disease. It can be concluded that majority of CRC patients were older than 40 years (86.7%) with features of intestinal obstruction (53.3%) and adenocarcinoma (84.4%) being the predominant mode of clinical presentation and histological subtype respectively.
Introduction
Colorectal carcinoma (CRC) is a malignant epithelial neoplasm accounting for most cases of gastrointestinal malignancy.1–8 The incidence of CRC varies from region to region with highest incidence being reported in the Western Europe, North America, Australia/New Zealand and Japan, while Africa and Asia had the lowest incidence rate. 9 Recent studies have demonstrated a gradual increase in incidence of CRC in regions previously classified as low incidence areas including Africa.3,8,10,11 The change in trend of CRC in developing countries including Africa may be adduced to adoption of westernized diets, sedentary life style, cigarette smoking and an increased awareness of symptoms and signs of CRC.2,3,8 On the other hand, a study in Africa has reported a low incidence of CRC which has been attributed to the rarity of some premalignant conditions including adenomata, inflammatory bowel disease and familial polyposis syndromes in comparison to their Caucasian counterparts. 12
The mean ages of CRC diagnosis vary from region to region. In Africa, Asia and New Zealand, mean ages ranged from 46.0 to 69.0 years while mean age higher than 70 years was reported in Europe.10,11,13–17
Although CRC is not gender specific, some studies have reported gender disparity with incidence being skewed in favor of males with a male to female ratio ranging from 1.1:1 to 1.6:1.3,8,10,11,14–20
Many predisposing factors have been implicated in the etiopathogenicity of CRC with interplay between genetic and environmental factors being at the front burner. The environmental factors include unhealthy diets rich in carbohydrate and fats, sedentary life style, cigarette smoking, obesity, ulcerative colitis, schistosomiasis, adenomatous polyps, lower socio-economic status and low rates of CRC screening programmes.8,13,14,21–28
In addition, some well-recognized hereditary conditions have been identified as the risk factors to the development of CRC in 5.0 to 10.0% of cases.26,29 They include familial adenomatous polyposis (FAP) with mutations in the tumor suppressor gene APC and hereditary non-polyposis colorectal cancer (HNPCC) with mutations in genes involved in the DNA repair pathway, namely the MLH1 and MSH2 genes.26,30 Other contributing risk factors for development of CRC include family history of colorectal cancer or adenomatous polyps in any first-degree relative younger than 60 years. 31
CRC is characterized by different symptoms and signs, some of which are anatomic location-specific. These clinical features of CRC include bleeding per rectum, weight loss, abdominal pain, diarrhea, constipation, nausea, vomiting and abdominal mass.3,8,14,16,28,32–37
Recto-sigmoid region and adenocarcinoma were the preponderant site and histologic subtype involved in CRC.2,3,8,10,11,13–16
Most patients with CRC present in late stage with dismal prognosis.3,8,11,13,16,24
The study is aimed at identifying the clinical and pathological characteristics of CRC diagnosed between July 2006 and June 2015 in the University of Uyo Teaching Hospital, and a Private Specialist Laboratory, Uyo, Akwa Ibom State, Nigeria.
Materials and Methods
A retrospective study was undertaken to review the histopathological diagnoses of all colorectal cancer at the Department of Histopathology of the University of Uyo Teaching Hospital and a private specialist (Histo-Vision) laboratory in Uyo, Akwa-Ibom state, Nigeria between July 2006 to June 2015. Akwa Ibom State with Uyo as the state capital is located in the South-South geo-political region of Nigeria.
All these patients were diagnosed on clinical, laboratory and radiological examinations. The diagnosis was confirmed pathologically after the histopathological examination of either the resected specimens or the incisional biopsy specimens. All the patients with confirmed CRC were included in the study. Restaging was performed according to TNM Classification of Malignant Tumors (TNM) staging system based on the available clinical, radiological and histopathologic findings. The compiled data included demographic data, medical history and family history of colorectal cancers, chief presenting complaints, histological types, grade, TNM staging and the site of metastasis.
Slides and paraffin-embedded blocks of the pathological specimens of the CRCs were retrieved from the archive of the department and private specialist laboratory; where necessary, new sections were cut from the paraffin embedded tissue blocks and processed with hematoxylin and eosin stain. The slides were microscopically reviewed to confirm the diagnosis. Descriptive statistics were used for analyzing the data using SPSS (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY, USA: IBM Corp.) and results were presented in percentage, simple frequency, tables, figures and photomicrographs.
Results
CRC was the most common malignant gastrointestinal tract (GIT) tumor accounting for 54.2% of all GIT malignancies; it represented 7.1% of all malignant tumors diagnosed from the two laboratories during the period under study.
A total of 45 patients of age range 26-80 years with a mean of 55.9 years (SD 3.9) and a male to female ratio of 1.4:1 were seen. The most common age group affected in CRCs was 61-70 years (13 cases, 28.9%). This was closely followed by an increase incidence in the 51-60 years age group (11 cases, 24.4%) while patients within the 21-30 years age group were least affected in CRC (2 cases, 4.4%). Majority of CRC patients were older than 40 years (39 cases, 86.7%) while only 6 (13.3%) patients were younger than 40 years (Table 1).
Age and sex distribution of patients with colorectal carcinoma.

In our study, predisposing factors were identifiable in 11 (24.4%) cases while the remaining 34 (75.6%) cases had no defined predisposing factor. The identifiable predisposing factors for CRC were tubulo-villous adenomatous polyps (4 cases, 8.8%), villous adenomatous polyps (2 cases 4.4%), polyposis syndromes (2 cases, 4.4%), obesity (2 cases, 4.4%) and schistosomiasis (1 case, 2.2%). Most patients with prior history of tubulo-villous and villous adenomas were older than 40 years in 3 (6.6%) and 1 (2.2%) cases respectively.
Two patients had family history of CRC while family history of extra-colonic malignancy was found in one patient.
Features of large intestinal obstruction were the most common presenting symptom of CRC (24 cases, 53.3%) with males (a male to female=1.2:1) and 41-50 years age group being more slightly affected. Rectal bleeding, alteration in bowel habit and fecal incontinence were other symptoms, accounting for 15 (33.3%), 4 (8.9%) and 4 (4.4%) cases respectively (Table 2).
Clinical presentation of patients with colorectal carcinoma in the study population.

Abdominal ultrasonography, sigmoidoscopy, computed tomography (CT) scan and occult fecal blood test contributed positively in the diagnosis of CRCs in 77.6, 29.9, 14.9, and 40.3% of cases respectively. Colonoscopy was not done for any of the patients.
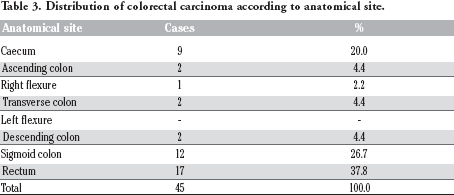
Left-sided CRCs were more common (68.9%) with the majority appearing as annular-constricting growth pattern macroscopically (27 cases, 60.0%) while right-sided CRCs were less common (31.1%) with the majority appearing as exophytic-fungating type macroscopically (8 cases 17.8%). Only a minority of CRC appeared in flat-depressed growth pattern macroscopically (2 cases, 4.4 cases). Recto-sigmoid region was the preponderant site involved in CRC (29 cases, 64.5%). The caecum was involved in 9 (20.0%) cases while ascending colon, transverse colon, descending colon were affected in 2 (4.4%) cases each. The right flexure was the least affected in 1 (2.2%) case (Table 3).
Distribution of colorectal carcinoma according to anatomical site.
Adenocarcinoma accounted for the majority of CRCs histologic subtypes (38 cases, 84.4%), many of which were well differentiated (21 cases, 55.3%), moderately (14 cases, 36.8%) and poorly (3 cases, 7.9%) differentiated. Mucinous carcinoma, signet ring carcinoma and carcinoid tumor were other histologic types seen in 4 (8.9%), 2 (4.4%) and 1(2.2%) cases respectively (Figures 1 and 2).

Histological types of colorectal carcinoma among patients in the study population.

Photomicrograph of colon showing well differentiated adenocarcinoma. Hematoxylin and Eosin 100×.
Majority of patients presented in early stage of the disease (35 cases, 77.8%) with either TNM I or TNM II. Ten CRC patients (22.0%) presented at advanced stages of the disease with 17.8% of the patients presented with regional lymphadenopathy. Two patients had distant metastasis to the liver (4.4%).
Discussion and Conclusions
Our study showed that CRC accounted for 6.7% of all malignancies and 54.2% of gastrointestinal malignancies diagnosed during the period under review. Similar studies in Nigeria, Tanzania, Saudi Arabia, and Europe have reported varying frequencies of CRC ranging from 4.7 to 29.3% of all malignancies diagnosed,1–4 which agree with most studies in which CRC was reported as the most common gastrointestinal malignancy.2,5–8 From the foregoing, it is obvious that incidence of CRC varies from region to region with highest incidence being reported in the Western Europe, North America, Australia/New Zealand and Japan, while Africa and Asia had the lowest incidence rate. 9 However, gradual rising incidence has been reported from various parts of Africa including Nigeria which were considered low incidence areas previously.3,8,10,11 The change in trend of CRC in Africa may be adduced to adoption of westernized diets poor in fibers but rich in carbohydrate and fats, an increased awareness of symptoms and signs of CRC as well as an increased hospital attendance by some patients. Nevertheless, many cases of CRC are still being underreported owing to the facts that some patients preferred to visit the trado-medical (herbalists) homes, chemists and religious outfits for treatment. Also, some patients exhibit phobia for surgery, thus declining to visit hospital for prompt diagnosis and treatment. Persistent low incidence of CRC in some African countries have been linked to low incidence of premalignant conditions including adenomata, inflammatory bowel disease and familial polyposis syndromes in comparison to their Caucasian counterparts. 12
The mean age of our patients at the time of diagnosis was 55.9 years. This finding agrees with other studies in which mean ages of 50.7 years, 57.2 years, 46.0 years, and 54.3 years were reported in South western Nigeria, Iran, Togo and South Africa respectively.8,10,11,13 These are however lower than the mean ages ranging from 67.9 to 69.0 years commonly reported in most developed countries with a differential of about 10.0 years.14,15 The frequency of CRC in patients aged 40.0 years or above in our study was 86.7% which compares relatively with findings of other studies including 77.9% in South Africa, and 77.0% in Lagos and Sagamu.8,11 In our study, bimodal peak age of incidence for CRC was seen in the 61-70 years (28.9%) and 51-60 years age group (24.4%) which is similar to 23.3% in 61-70 years and 21.5% in 51-60 years reported in South Africa. 11 These findings are however in contrast to other studies in which patients within the 60-69 years and 65-75 years age groups were reported to be the most common age group affected by CRC in South Western Nigeria and Southern Iran respectively.8,16 From the foregoing, it is obvious that incidence of CRC increases with age and the likelihood of CRC diagnosis increases progressively from age 40.0 years with the incidence rate being more than 50 times higher in persons aged 60 to 79 years than in those younger than 40 years. 17 Thus, it is imperative to encourage individuals aged 40 years or above to go for colorectal screening.
In our study, a male to female ratio of 1.4:1 in the patients with CRC showed a slight male predominance, which concurs with most studies reporting a male to female ratio ranging from 1.1:1 to 1.6:1.3,8,10,11,14–20 However, Ojo and colleagues in Ile-Ife, Nigeria recorded a contrasting male to female ratio of 2.3:1.0. 21 The gender disparity with a male preponderance reported by most studies may be coincidental findings or adduced to the use of hormone replacement therapy associated with reduced incidence of the CRC in females owing to effect of female sex hormones on cholesterol metabolism and bile acid production, a pathway if unchecked link to the development of colorectal cancer. 20
In this series, predisposing factors including tubulo-villous adenoma, villous adenoma, polyposis syndromes, obesity and schistosomiasis were identified for CRC in varying proportions with adenomatous polyps being the most commonly associated predisposing factor (13.2%). This finding is relatively consistent with findings of other studies in which many predisposing factors have been implicated in the aetiopathogenicity of CRC with special attention to strong interaction between the genetic and environmental factors. The environmental factors include unhealthy diets rich in carbohydrate and fats, sedentary life style, cigarette smoking, obesity, ulcerative colitis, schistosomiasis, adenomatous polyps, lower socio-economic status and rates of CRC screening programmes.8,13,14,22–28 Overall, the incidence of adenoma in Africa tends to be low when compared with the West. This fact is also supported by a study in South Africa where a frequency of adenoma was reported to be 5.2% and advocacy for exploitation of other possible mechanisms involved in the etiopathogenesis of CRC besides the well known classical adenoma-carcinoma sequence was made. 11
In addition, some well-recognized hereditary conditions have been identified as the risk factors to the development of CRC in 5.0 to 10.0% of cases.26,29 They include FAP with mutations in the tumor suppressor gene APC and HNPCC with mutations in genes involved in the DNA repair pathway, namely the MLH1 and MSH2 genes.26,30
In our study, few patients with proven positive family history of CRC were found (6.7%), which are lower than 26.9% reported in the first-degree relatives of patients with CRC in South Iran. 16 Also, it has been suggested that people with a stronger family history including a history of colorectal cancer or adenomatous polyps in any first-degree relative younger than age 60; or a history of colorectal cancer or adenomatous polyps in two or more first-degree relatives at any age have higher risk for the development. 31
The signs and symptoms of colon cancer are varied, nonspecific, and somewhat dependent on the anatomic location of the tumor in the colon as well as the extent of constriction of the lumen caused by the cancer.28,32 Features of large intestinal obstruction were the most common presenting symptom of CRC (53.3%) which agrees with preponderance of left sided CRCs (68.9%) presenting as annular-constricting growth pattern macroscopically (60.0%) in our series. Rectal bleeding was the second most common symptom (33.3%), which is consistent with right sided CRC presenting as an exophytic growth pattern with rectal bleeding being the most common symptom.8,14 Alteration in bowel habit and fecal incontinence were other symptoms, accounting for 8.9 and 4.4% of cases respectively. This finding compares with varying symptoms and signs including rectal bleeding, weight loss, abdominal pain, diarrhea, constipation, nausea, vomiting and abdominal mass reported in many studies.8,14,16,28,33,34 Although the presenting symptoms reported by Graham and colleagues did not differ from most studies, but they reiterated the fact that rectal bleeding appeared to be the most common presenting symptom necessitating the need to seek medical attention,3,14,35–37 which is in contrast to features of intestinal obstruction reported in our study (53.3%) and abdominal pain in Southern Iran (60.7%). 16
In addition, nature of clinical presentation varies with the state of clinical scenario in which rectal bleeding (56.0%) and altered bowel habit (31.3%) were predominant clinical presentation in elective cases whereas intestinal obstruction (55.6%) and peritonitis (22.2%) were predominant clinical presentation in emergency cases. 33 Furthermore, certain clinical indices including abdominal pain, diarrhea, constipation, abnormal rectal examination, abdominal tenderness, hemoglobin <10.0 g/dL; positive fecal occult bloods, blood glucose >10 mmol have been reported as positive predictors for CRC.14,33,34 Thus, high suspicion for early and prompt diagnosis of CRC needs to be demonstrated by medical doctors seeing patients with the aforementioned clinical indices.
Recto-sigmoid region and adenocarcinoma were the preponderant site and histologic subtype involved in CRC in 64.5 and 84.4% respectively which concur with reports from Tanzania, South western Nigeria, and Europe.3,8,38 In fact, adenocarcinoma of varying grades were widely reported by many studies as the predominant histologic subtype of CRC.2,10,11,13,15,16 In our study, most of the adenocarcinomas were either well differentiated (55.3%) or moderately (36.8%) which concurs with a study in South Western Nigeria where majority of adenocarcinomas were either well differentiated (55.5%) or moderately (21.0%), 8 but differs from findings in South Africa in which adenocarcinomas were either moderately (56%) or poorly differentiated (31%). 11 Besides adenocarcinoma few cases of mucinous carcinoma was seen in patients aged 60 years or above, exclusively restricted to the right colon (5.6%), which compares relatively with a report in which mucinous or signet ring accounted for one third of CRC cases. 11 This, however differs slightly from a study in South Western Nigeria in which mucinous, anaplastic and signet ring carcinomas accounted for 10.7, 3.6 and 1.2% of cases of CRC respectively, 14 but agrees with the preponderance of mucinous carcinoma in the right colon. 8
Although few cases of advanced stage CRC was found in our study (22.0%) with regional lymphadenopathy and distant metastasis which is at variance with a report in which most patients had advanced stage CRC (96.7%) with lymph node and distant metastasis in 30.4 and 24.7% of cases, respectively. 3 In Southern Iran, lung, brain and ovary in 99.5, 99.5 and 99.2% were metastatic sites of CRC respectively. 16 A report from South Africa, South Western Nigeria, Iran and UK reported a higher frequency of advanced stage CRC in 54.5, 35, 52 and 51.2% of cases respectively.8,11,13,24
Many reasons have been ascribed to the late presentation of patients with CRC. These include ignorance with misconception on the cause of CRC, poverty, stigmatization related to cancer moribund state, insufficient diagnostic and therapeutic equipment. In addition, absence of well structured screening programs including colonoscopy, fecal occult blood test as well as subsidized treatment policies by governmental, private and non-governmental agencies necessary for early detection and prompt treatment of premalignant lesions including adenomatous polyps and early stage CRC have been implicated.
Footnotes
Acknowledgement
Our sincere appreciation goes to the management and staff of the University of Uyo Teaching Hospital, Uyo, Akwa-Ibom state, Nigeria for their uncountable supports towards the successful completion of this study.