
Abstract
Objective
Oropharyngeal squamous cell carcinoma (OPSCC) is a malignant tumor that occurs at the tongue base, soft palate, palatine tonsil, and pharyngeal wall. Few studies of OPSCC have been performed in elderly patients.
Methods
Patients with human papilloma virus (HPV)-related OPSCC were extracted from the Head and Neck with HPV Status Database of the Surveillance, Epidemiology, and End Results (SEER) database between 2010 and 2016. We identified 355 patients with HPV-positive status, and we retrospectively evaluated elderly (≥65 years) and younger (30–64 years) patient groups to compare the differences.
Results
Of the 355 patients who were diagnosed with HPV-related OPSCC, 113 constituted the elderly group. Comparing the elderly group with the younger group, the 3-year HPV-positive overall survival (OS) rates were 62.4% and 70.2%, respectively, and the 5-year OS rates were 50.4% and 59.2%, respectively. Cox regression analysis demonstrated that tumor (T) stage and chemotherapy were prognostic factors for OS.
Conclusion
Elderly patients with OPSCC had different clinicopathological characteristics. T stage and chemotherapy should be priorities when evaluating the OS of elderly patients with OPSCC.
Keywords
Introduction
Oropharyngeal squamous cell carcinoma (OPSCC) is a common type of head and neck cancer and accounts for more than 13% of all head and neck cancers globally.1,2 The clinicopathological characteristics of OPSCC vary greatly in different regions, and according to race, sex, and living habits. 3 The OPSCC incidence is increasing among elderly patients, and few studies are available.4–6 A retrospective study of 43 elderly patients with OPSCC by Dave et al. 7 found that 3-year overall survival (OS) was 85.5% (95% confidence interval (CI): 71.4%–100%), and 3-year disease-free survival was 67.3% (95% CI: 49.7%–91.0%). The current study reviewed the clinicopathological characteristics and OS of elderly patients with OPSCC in a large national population-based database to measure the effect of treatment and prognostic factors, to provide suggestions for clinical work.
Methods
Patient selection
Patients diagnosed with OPSCC between 2010 and 2016 were abstracted selectively from the Surveillance, Epidemiology, and End Results (SEER) database. 8 The study cohort constituted patients with International Classification of Diseases (ICD) for Oncology, third edition (ICD-O-3), 9 histology code 8070-8075. Eligible patients had primary tumors, histologically-confirmed malignant OPSCC, complete follow-up data, and known age and race; autopsy or death certificate-only cases were excluded. Signed authorization and permission were obtained from SEER to evaluate and use the dataset. The need for ethical approval and informed consent was waived by our local ethics committee because SEER data are publicly available and de-identified.
Variables
We analyzed the following prognostic factors in patients with OPSCC: race, sex, American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) stage (manually adjusted according to the AJCC Cancer Staging Manual, 8th edition), 10 surgery, radiotherapy, and chemotherapy.
Statistical analyses
The observed differences between the groups were compared using the t test with IBM SPSS 23.0 (IBM Corp.; Armonk, NY, USA). Kaplan–Meier cumulative survival curves for each patient variable were constructed with R 3.6.1 (R Core Team, 2014) and were weighted using the log-rank test. Prognostic variables were determined by Cox proportional hazards regression and were reported as hazard ratios (HRs). Variables with P < 0.05 in the univariate analysis were included in the multivariate analysis. Nomograms for OS were constructed with R 3.6.1 according to the prognostic variables (P < 0.05) in the multivariate analysis.
Results
Patient characteristics
We identified 1848 patients with OPSCC in the SEER database. We excluded 421 patients with missing TN stage and surgical status data and 756 patients with unknown HPV status; 671 patients had HPV-diagnosed OPSCC. Of the 671 patients, 113 patients aged ≥65 years (elderly patient group) and 242 patients aged 30 to 64 years (younger patient group) were diagnosed as having HPV-positive OPSCC (Table 1). The majority, 102 (90.3%) and 100 (88.5%), were white and male, respectively. Fifty-three patients (46.9%) were stage I, 38 (33.6%) were stage T2, and 73 (64.6%) were stage N1 according to the 8th edition of the AJCC TNM classification. When we used the 7th edition of the TNM classification, 61.1% of the patients were classified as having stage IVA disease. In the younger group, 36.4% and 37.6% of the patients were classified as stage I and III, respectively, while 56.2% of the patients were classified as stage IVA.
Baseline characteristics of patients who were HPV-positive.

* Constitutes Black, Asian, Pacific Islander, Native American, and Alaska Native.
Values are presented as n (%).
HPV, human papilloma virus; TNM, tumor-node-metastasis; T stage, tumor stage; N stage, node stage.
Survival according to TNM stage and treatment
The survival probability of the two groups did not differ significantly (Figure 1a–d). The 3-year OS for early-stage (I–II) and advanced-stage (III–IV) OPSCC was 70.9% and 35.6%, respectively, in elderly patients, and 85.6% and 43.8%, respectively, in younger patients (Table 2). Figure 2a–h shows the survival curves for OS in each group. Survival rates for T2 stage and N1 stage were 70.1% and 55.7%, respectively, in elderly patients, and 39.6% and 74.7% for T4 stage and N1 stage, respectively, in younger patients. The Kaplan–Meier survival curves revealed no statistically significant difference between the three treatments (surgery, radiotherapy, and chemotherapy) in the two groups. However, intra-group Kaplan–Meier analysis showed that surgery and chemotherapy were the only non-significant factors in the elderly and younger groups, respectively (Figure 2b, 2h). Figure 3 is a nomogram for predicting 3- and 5-year OS.

Kaplan–Meier estimates of overall survival in elderly and younger patients with OPSCC by (a) overall survival, (b) surgery, (c) radiotherapy, and (d) chemotherapy.
Treatments and 3-year overall survival of elderly and younger patients with OPSCC.
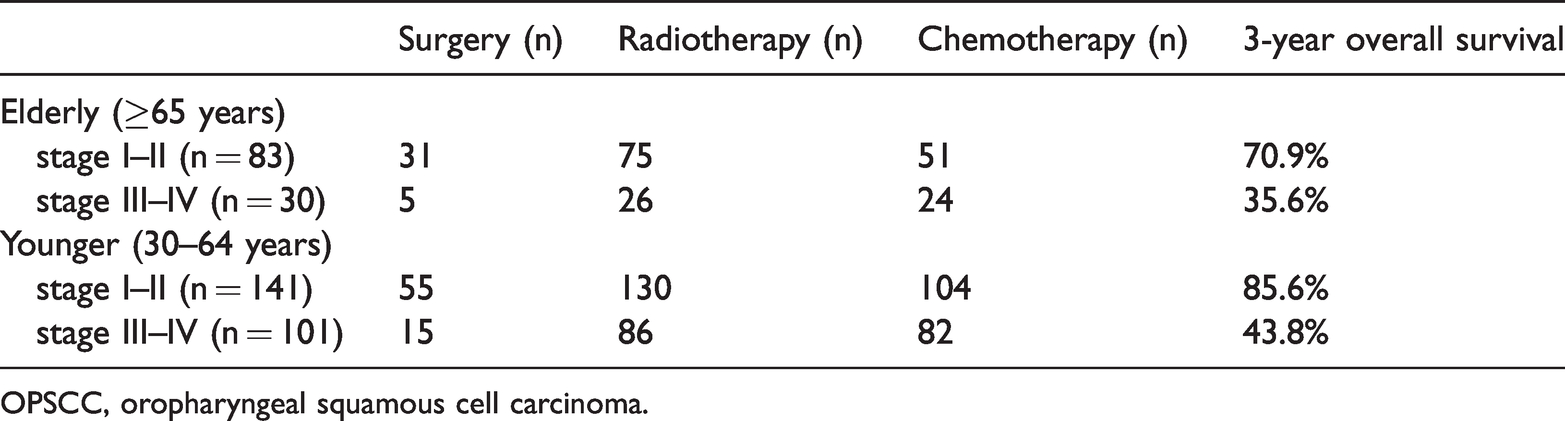
OPSCC, oropharyngeal squamous cell carcinoma.
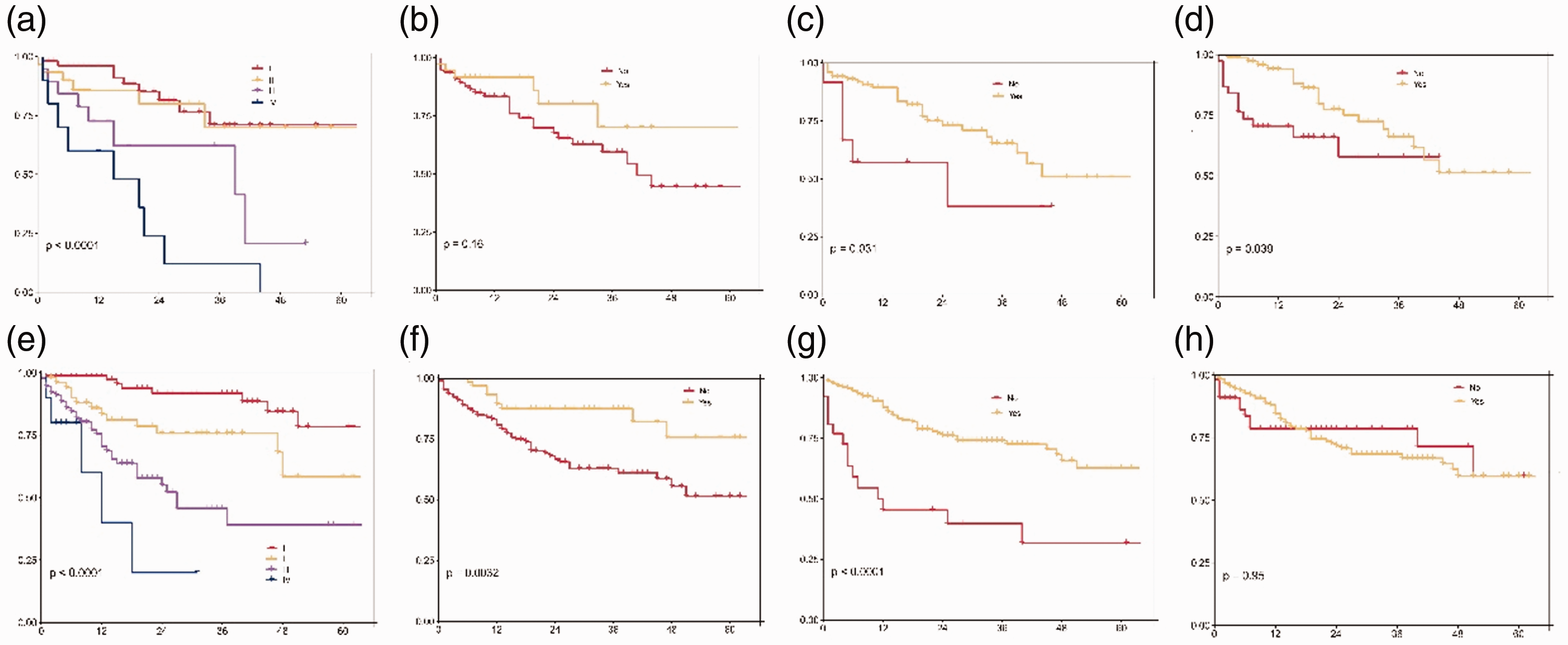
Kaplan–Meier estimates of overall survival in elderly patients with OPSCC by (a) TNM stage, (b) surgery, (c) radiotherapy, and (d) chemotherapy; and in younger patients by (e) TNM stage, (f) surgery, (g) radiotherapy, and (h) chemotherapy.

Nomogram to predict 3- and 5-year OS in elderly patients with OPSCC.
In the univariate Kaplan–Meier survival analysis (Figure 1 and Figure 2), radiotherapy (P = 0.031) and chemotherapy (P = 0.039) were independent factors affecting OS in the elderly group, while surgery had no significant effect. In the younger group, radiotherapy (P < 0.001) and surgery (P = 0.0032) were independent factors affecting OS.
COX regression analysis of the prognostic factors
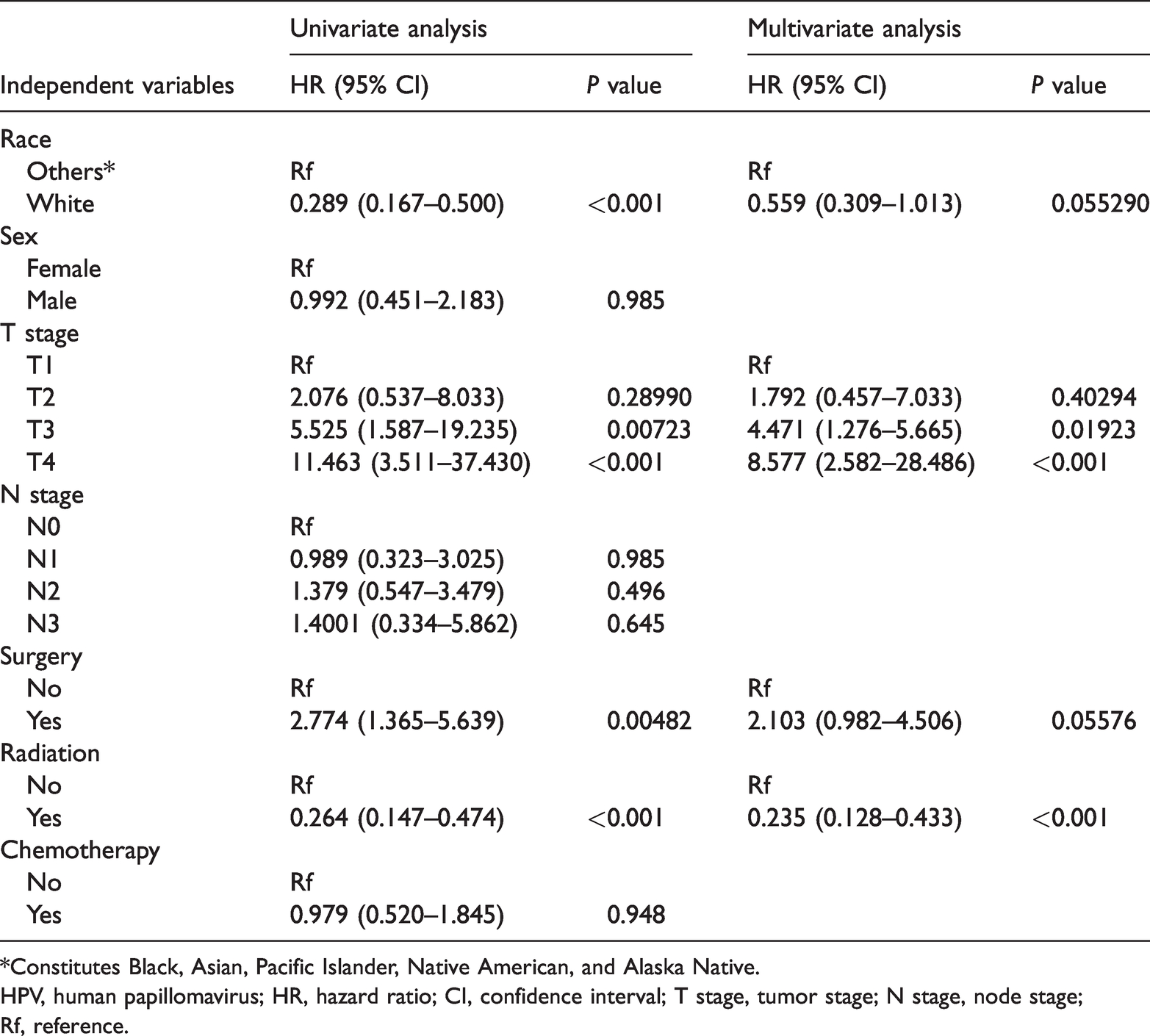
According to the multivariate Cox regression analysis, in elderly patients, T stage (P = 0.0015; Table 3) and chemotherapy (P = 0.004; Table 3) were significant prognostic factors for OS (Table 3); radiotherapy (P < 0.001) and T stage (P < 0.001) were significant prognostic factors for OS in younger patients (Table 4). The multivariate analysis included all covariates with P < 0.05 in the univariate analysis and showed that T stage, radiotherapy, and chemotherapy were independent predictors of survival. According to the multivariate Cox regression analysis, in elderly patients, T stage (P = 0.0015) and chemotherapy (P = 0.004) were significant prognostic factors for OS (Table 3); radiotherapy (P < 0.001) and T stage (P < 0.001) were significant prognostic factors in younger patients (Table 4). The distinction between the two groups was radiotherapy (younger patients) and chemotherapy (older patients).
Univariate and multivariate COX proportional hazard analysis in elderly patients who were HPV-positive.

*Constitutes Black, Asian, Pacific Islander, Native American, and Alaska Native.
HPV, human papilloma virus; HR, hazard ratio; CI, confidence interval; TNM, tumor-node-metastasis; T stage, tumor stage; N stage, node stage; Rf, reference.
Univariate and multivariate COX proportional hazard analysis in younger patients who were HPV-positive.
*Constitutes Black, Asian, Pacific Islander, Native American, and Alaska Native.
HPV, human papillomavirus; HR, hazard ratio; CI, confidence interval; T stage, tumor stage; N stage, node stage; Rf, reference.
Discussion
In this study, we aimed to describe the clinical features and prognosis of elderly patients with HPV-related OPSCC compared with younger patients. In our study cohort, male patients constituted 88.5% of the elderly cohort, which is consistent with existing reports and indicates that elderly patients with OPSCC have a strong male predominance. 11 Although an association of race with head and neck cancer prognosis has been reported,12,13 it is not appropriate to isolate race as an independent prognostic factor. There are significant differences among ethnic groups regarding economic status and the level of treatment that directly affect survival. Race cannot be considered a factor when considering overall outcomes.
The 8th edition of the AJCC Cancer Staging Manual significantly downgraded the TNM staging of patients who are HPV-positive, especially elderly patients. In the 7th edition, these patients were mainly classified as stage IV, while in the 8th edition, patients were mainly classified as stage I after the downgrading, and in the younger group, the patients were classified as stage I and III. Compared with the 7th edition, the 8th edition considers HPV status according to tobacco and alcohol use, only. 14 Patients with P16 protein-positive oropharyngeal carcinoma are more sensitive to radiotherapy and chemotherapy, and their prognosis is significantly better than that of those with P16 protein-negative status. P16 is considered an independent prognostic factor affecting the prognosis.15,16 The better prognosis is mainly owing to the better biological behavior of HPV-related diseases, as well as to relatively young age and good health status at the time of diagnosis. Our study showed that the proportion of patients who were in the early stage according to the 8th edition TNM staging was significantly higher than that according to the 7th edition, and the difference was statistically significant (P < 0.001), which was consistent with the results of previous studies. 17 As a direct result of the downgrading, there are differences in OS and treatment regimens between the older and younger groups. Age is an important factor affecting the prognosis of many tumors, but in our study, the Kaplan–Meier survival analysis indicated no significant difference in OS between the elderly and younger groups, which may be because of the relatively reasonable treatment plan formulated by clinicians according to the staging in the 8th edition.
Radiotherapy is the most commonly used treatment for oropharyngeal tumors. While radiotherapy and chemotherapy effectively avoid the risk of cosmetic deformities compared with surgery, the long-term adverse effects are not negligible. There is a need to improve radiotherapy regimens to reduce toxic adverse effects. Some novel therapies have been reported to be effective, but their effectiveness in older patients remains to be demonstrated. 2 Radiotherapy and chemotherapy significantly improve OS and relapse-free survival compared with radiotherapy alone, according to a randomized clinical trial involving patients with advanced oropharyngeal cancer. 18 In the treatment of oropharyngeal cancer, especially in the advanced stage, surgery combined with radiotherapy/chemoradiotherapy and radiotherapy combined with chemotherapy are often used. According to the 2017 American Society for Radiation Oncology oropharyngeal cancer management guidelines, 19 radical radiotherapy is not recommended in patients with stage I and II disease undergoing systemic concurrent chemotherapy. The guidelines also do not recommend routine induction chemotherapy for patients with OPSCC. Our study indicated that in elderly patients, especially those with early-stage OPSCC, both Kaplan–Meier and COX survival analyses emphasized the therapeutic effect of chemotherapy.
During treatment, in addition to formulating the corresponding treatment plan, follow-up is essential. 20 We constructed a nomogram to predict the 3- and 5-year OS of patients. The timely adjustment of the treatment plan by predicting results, and follow-up, may help improve the survival of elderly patients with OPSCC.
One limitation of our study is that tobacco and alcohol use were not listed in the SEER database; therefore, these factors could not be assessed in this study. Smoking and alcohol are associated with high risk of developing OPSCC. 21
Conclusion
Elderly patients with OPSCC had different clinicopathological characteristics. Determining the T stage and administering chemotherapy should be priorities when evaluating the OS of elderly patients with OPSCC.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a High-level Hospital Construction Research Project of Maoming People’s Hospital, China Postdoctoral Foundation (Project No.: 2018m633286), the clinical effect of 3D printing-assisted reconstruction of jaw defects (Project No.: 190403221700895), Science and Technology Special Fund of Guangdong Province (Project No.: 2020S00049), Maoming Science and Technology Plan Project (Project No.: 2019018023), and the Medical Science and Technology Research Foundation of Guangdong Province (Project No.: B2018061, A2017490).