
Abstract
Digital papillary adenocarcinoma (DPA) is a rare malignant tumor of the sweat glands that often presents as a solitary painless mass on the digits of the hands or feet. We present a rare case of DPA on the ankle in a 54 year-old African American man. Although the most common location for digital papillary adenocarcinoma is on the hands and feet, it can present in other locations. Treatment modalities and concerns such as the level of margin resection, degree of negative margins, and the need for a sentinel lymph node biopsy might be different if the tumor is encountered in locations other than the digits. In the following manuscript, we discuss the natural history of this rare tumor including a review of the current literature with emphasis on documented treatment strategies as well as the approach in treating patients with a unique presentation.
Introduction
Digital papillary adenocarcinoma (DPA) is a rare malignant tumor of the sweat glands originally described by Helwig in 1979.1,2 It often presents as a solitary painless mass commonly found on the volar surface of the fingers and toes and on the adjacent skin of the palms and soles.3–7 It is three times more common on the hands than feet, occurs almost exclusively on the digits, and is most frequently diagnosed in Caucasian men in their 50s-70s. 8 These tumors are mainly asymptomatic and can be present for several months to years before medical attention is sought. These tumors are often not recognized because of their rarity, which can be detrimental to the patient as there is high potential for metastasis, with a local recurrence rate of 50% and a 14% rate of metastasis, most commonly to the lungs (70%).8,9 DPA can also occasionally be misdiagnosed for a metastasis of papillary adenocarcinoma originating in the colon, thyroid, or breast. 10 These malignancies should be excluded in patients presenting with DPA. In the present report, we describe a patient with DPA of the ankle. The unusual location of the tumor is discussed along with the various reported treatment options for both local and metastatic disease.
Case Report
This is a case of a 54-year-old African American man with DPA with an unusual location of his initial tumor and whose management required further assessment of metastasis and need of addressing a lateral positive margin. The patient initially presented to clinic in 2012 with complaints of a six-year history of a bump on his left ankle. The patient described the bump as a non-painful mass that had been steadily enlarging over the past several years. There was no history of ulceration, redness, or discharge from the site and the patient denied any constitutional symptoms. On physical exam, the patient had a skin mass approximately 0.5 cm in diameter on the lateral dorsum of his right foot. The mass was freely mobile, non-erythematous, and smooth. At the time of his initial presentation, he expressed interest in surgical removal of the mass. The patient was lost to follow up prior to his surgery and presented to the clinic again in 2014 with the same complaint and indicated that the mass had now grown in size. The patient again denied any constitutional symptoms. The patient underwent excisional biopsy of this lesion. Pathological examination of this specimen demonstrated a 2.0×1.7×1.5 cm circumscribed unencapsulated dermal-based mass with a homogenous tan cut surface. Microscopically, the lesion proved to be an adenocarcinoma with ductal differentiation and predominantly cribriform pattern. Occasional mitotic figures and foci of comedo-like necrosis were present. The histologic findings were diagnostic of DPA (Figure 1). The cauterized lateral margin was positive for tumor. Given the natural history associated with this diagnosis and the positive surgical margin, colonoscopy and positron emission tomography (PET) were ordered. Colonoscopy was negative for malignancy. There was no history of physical findings suggestive of thyroid or breast malignancy. PET demonstrated a focus of intense activity in the right iliopsoas muscle neighboring the right femoral neck that was thought might represent metastatic disease (Figure 2). No other areas demonstrated activity. Based on the results of the PET, a magnetic resonance imaging (MRI) study was obtained, which showed a soft tissue mass anterior to the right femoral neck that was indeterminate in imaging appearance, but was thought to be a possible metastatic lesion. Based on both the PET and MRI results the decision was made to proceed with a fine needle aspiration (FNA) biopsy to determine the nature of the lesion. Computed tomography (CT) guided FNA biopsy of the mass demonstrated changes consistent with an inflammatory process, but showed no malignant cells and no evidence of metastatic adenocarcinoma. He was then re-scheduled for re-excision of margins and follow up for both clinical exam and a screening chest X-ray in 1 year. 8 He underwent excisional biopsy of margins, which demonstrated all to be negative for tumor.
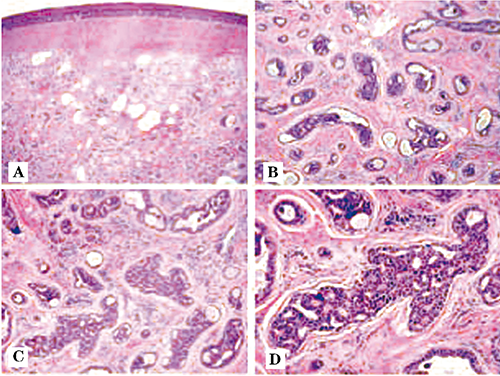
The histologic findings (Hematoxylin & Eosin).

Positron emission tomography images demonstrating a focus of intense activity in the right iliopsoas muscle neighboring the right femoral neck.
Discussion
Digital papillary adenocarcinomas are rare malignant tumors of the sweat glands most commonly occurring on the hands and feet of white men in their 50s-70s. After the initial description by Helwig in 1979, as aggressive digital papillary adenocarcinoma (ADPA), around 100 cases have been reported in the literature. Kao and colleagues published a large case study of 57 patients with what they called ADPA in 1987. 8 These cases were divided into adenoma versus adenocarcinoma based on histologic findings. Adenocarcinoma was characterized by poor glandular distribution, necrosis, cellular atypia, and invasion of soft tissue bone, and blood vessels. The authors concluded that this tumor was distinct from other adnexal tumors as it had significant locally aggressive behavior and that histology findings characteristic of adenocarcinoma were predictive of increased incidence of recurrence and/or metastasis. 8 However, in 2000, Duke et al. published an additional retrospective study that analyzed the same 57 cases and found that of the 30 cases that had originally been diagnosed as ADPA, nine patients had a recurrence and three progressed to metastatic lesions. 9 They found that regardless of the differentiation of adenoma versus adenocarcinoma, there was only a 5% recurrence rate if re-excision or digital amputation was carried out after the initial diagnosis and 50% if there was no further treatment. 9 The authors, therefore, concluded that because of the metastatic potential of both subtypes, and since a histological diagnosis of adenoma could not be made accurately, all cases should be considered aggressive digital papillary adenocarcinoma and treated accordingly. 9 Due to the high metastatic potential of these tumors, it is imperative to diagnose and treat these tumors as early as possible. ADPA is referred to in a historical context since that is the term the various authors used in their case reports, however a recent paper by Chen and Asgari argues against this term on the basis that the tumor is not inherently aggressive, not restricted to the digits, and does not always have papillary features on microscopic exam. 11 They also suggest it may actually be an adenomyoepithelial tumor versus an adenocarcinoma based on review of the current literature and associated pathologic findings. 11 Wheedon suggests that the term aggressive is redundant, as these tumors are all now regarded as malignant. 12 Since our patient seems to adhere to this definition, we have adopted such classification for this report.
This tumor almost always presents as a solitary mass on digits of the fingers and toes.3–7,13 It most often occurs on the fingers as compared with the toes (3:1) and is more commonly found in men than women. 8 These tumors are often painless masses with no associated constitutional symptoms and they can be present for months to years before the patient seeks medical attention.
The natural history of these tumors is not well defined due to their rarity. However, DPA should be considered to be a tumor with high incidence of recurrence and metastatic potential. For instance, from Kao's 1987 study, 66.7% of patients that had an amputation were cured while 57.1% of patients treated with excision developed recurrent lesions. 8 In addition, the regional lymph nodes were involved in 57% of patients. 8 The study also found that 41.2% of all patients diagnosed with DPA developed distant metastases, some as late as 19 years after their initial diagnosis, and 71.4% of these metastases occurred in the lung parenchyma. 8 Thus, margins and follow up must be addressed carefully in these patients.
The mainstay of management for patients with DPA is surgical intervention – either wide local excision or digital amputation, although a search of the literature reveals no consensus regarding margins or extent of amputation. In Kao et al.'s 1987 study, three of the 57 patients underwent digital amputation while 14 had wide local excision involving the diseased digit. 8 Given that the authors found a recurrence rate of 57.1% with simple excision, the conclusion can be drawn that if the tumor is located on a digit, and there is no evidence of metastasis, the surgeon should perform an amputation versus wide local excision. 8 For the ankle it is not as clear if negative margins are required, as there are no reports in the literature of the importance of negative margins when performing a wide local excision of DPA. If there is no concurrent evidence of regional or distant metastases; then it may be beneficial to achieve negative margins in an effort to control local spread and it would be sound to proceed with obtaining the greatest negative margins without compromising wound complications or need for a graft. However, this tumor still has a high metastatic potential so even with negative margins, the tumor may have already seeded nearby sources. For this reason, even if surgical intervention achieves negative margins or if they proceed with an amputation, patients should still have scheduled follow up every year with an exam and screening chest X-rays to look for any evidence of distant disease.
In the setting of metastatic disease, margins may be of less importance. There is some thought that it is still important to achieve local control so that should the patient's metastatic lesions regress with treatment, there is less likely to be a recurrence from the original site. While patients have been cured, i.e. no evidence of metastatic disease, who underwent amputation, in patients with metastatic disease chemotherapy has not been shown to be successful in treating the distant lesions as was documented in two separate case reports by Kao et al. and Frey et al. respectively.8,14 Therefore, unless there is another reason for desiring negative margins, it may not be beneficial to take the patient back to the operating room for additional procedures to achieve adequate margins should the patient have documented metastatic disease. These issues must be individualized and are best addressed at multi-disciplinary conference.
In addition to the question of obtaining negative margins, there is discussion on various ways to treat distant metastases. Kao et al. reported several cases where isolated metastatic lesions were removed with varying degrees of success. 8 One patient was found to have a lung metastasis and underwent a lobectomy however died when the tumor spread to his omentum and later central nervous system. A second patient had a lobectomy performed for a lung metastasis and was alive one year following his surgery. A third patient had a metastasis to the tibia that was excised but later died as a result of metastatic disease to the pelvic bones and lungs. These findings suggest that if a patient has an isolated and easily resectable metastatic lesion, it can be beneficial to excise the lesion. However, given the high metastatic potential of this tumor, patients who undergo a metatestectomy should still be closely followed for recurrence and both local and distant spread.
Besides resection of distant metastases, there are also reports in the literature of using chemotherapy as one option to treat patients with unresectable metastases. In Kao et al.'s case study, two of the patients with metastatic tumors were treated with chemotherapy without any obvious benefit. 8 Frey et al. also published cases of two patients with DPA, one of which was treated with chemotherapy. 14 This patient had a mass on his right foot that was initially excised with negative margins, however a lung CT showed a nodule in the left upper lung concerning for metastasis. He was treated with paclitaxel and carboplatin every 3 weeks for his metastatic disease. However, carboplatin and paclitaxel caused neuropathy and were discontinued. He then developed a new metastatic lesion in the axilla. He refused radiation therapy and was treated with docetaxel, but the axillary mass continued to increase. Carboplain and 5-flurouracil were added to his chemotherapy regimen, but the patient died 4 months later. 14 The case reports by Kao et al. and Frey et al. documenting the ineffectiveness of chemotherapy in treating DPA led Malafa et al. to investigate the use of sentinel lymph node biopsy in staging DPA. 15 They report using sentinel lymph node biopsy to stage a patient who presented with DPA on the second toe of his left foot. Because this patient did not have negative nodes, no adjuvant therapy was provided after his initial amputation. However close follow up is indicated as there are reports of metastases occurring up to 30 years after the initial diagnosis. 8 Malafa et al. question if the failure of chemotherapy in the previously described patients might be attributed to the high tumor burden of these patients at the time of metastases and hypothesized that chemotherapy may be more effective when treating patients with occult metastasis. 15 They conclude that the real benefit of sentinel lymph node biopsy in patients with DPA may be in discovering those patients with occult regional lymph node metastases who are at higher risk for systemic metastases yet have minimal tumor burden and could benefit from treatment with adjuvant chemotherapy. However, in a recent report inclusive of 31 cases of DPA, 4 patients had sentinel lymph node biopsies, all of which were negative, and none of these four patients developed metastatic disease. 13 The remainder of the patients in the case report did not receive a sentinel lymph node biopsy and of these patients, 2 had subsequent metastases to regional lymph nodes. 13 In addition, 5 of the patients who were found to have lung metastases had no clinical evidence of involvement of regional lymph nodes at presentation, although one patient did have a regional lymph node metastasis prior to the occurrence of the lung metastasis. 13 These findings led the authors to conclude that additional study is needed to address the benefit of sentinel lymph node biopsy in these patients before any recommendations can be made. 13
As of this case report, there has been no documentation in the literature of using radiation as an adjuvant therapy to treat DPA. However, if a patient has a metastatic lesion that is not easily surgically accessible, there may be some benefit for radiation therapy for local control or palliation depending on the situation.
Regardless of which treatment modality is selected, should a patient present with metastatic disease or is cured with no evidence of metastases after either amputation or excisional biopsy, these patients require close clinical follow up given the high rate of metastasis and the risk of progression of DPA. The most recent guidelines come from Kao et al. as a result of their 1987 case report, which entails an exam and chest x-rays once a year for a minimum of 10 years after the initial diagnosis since these tumors have been documented to show up as long a 19 years after the initial diagnosis. 8
Conclusions
The present report describes an unusual case of digital papillary adenocarcinoma on the left ankle. This case report addresses the various treatment strategies that have been published in the literature and additional options that have until now not been reported, and also emphasizes how location of this rare tumor, especially if not on the digits of the hand or feet, may alter the treatment modalities utilized by the treating physicians.
Footnotes
Acknowledgements
Authors would like to thank Robert M. Genta, MD for his assistance with photomicroscopy of this case.