
Abstract
Primary adenocarcinoma of the bladder is a rare tumor. The classification between primary vesical and urachal is debated. We present the case of a young female who presented clinicopathological features of a metastatic urachal adenocarcinoma, but the histological result revealed primary adenocarcinoma of the bladder contrary to expectancy. To the best of our knowledge this is the first reported case of a metastatic adenocarcinoma of the bladder in a 25 years old female. This case emphasizes the challenge for urologists to recognize and manage this aggressive tumor in the setting described.
Introduction
Pure adenocarcinoma of the bladder is a rare tumor accounting for 0.5–2% of all bladder cancers. 1 It is classified in primary vesical, urachal and metastatic. The incidence of primary adenocarcinoma is greater in areas where bilharziasis is endemic (5–11.4% of all bladder tumors) and in adult exstrophy patients (4%).2,3 It is more common in patients over 50 years old. The rate of extravesical disease at diagnosis is higher compared to urothelial carcinoma because it is often a solitary lesion, has predilection for local invasion and symptoms are late. Clinical presentation is similar to others bladder tumors with hematuria, suprapubic pain and voiding difficulties being the most common symptoms. Diagnosis is made by cystoscopy, urinary cytology and transurethral resection of the baldder.
The pathogenesis is different: the urachal adenocarcinoma arises from the remnant of the embryonic allantoic stalk, which connects the umbilicus to the fetal bladder. Consequently, the location of the tumor is always at the dome of the bladder whereas primary adenocarcinoma of the bladder arises from metaplastic changes of unstable urothelium, potentially from any portion of the bladder.4,5 Some classifications have been suggested. Most widely used, the Sheldon's classification has restrictive criteria. Tumor located at the dome of the bladder, absence of cystitis glandularis and cystitis cystica, primary involvement of muscle or deeper structures, clear demarcation between tumor and normal urothelium, presence of urachal remnant in association with the neoplasm and extensions of the tumor to the space of Retzius are all considered as necessary criteria to classify a tumor as an urachal adenocarcinoma. 6 Other classifications use less restrictive criteria considering a mass arising from the dome of the bladder as adenocarcinoma of urachus unless a transition between normal urothelium and adenocarcinoma is proved. 7
We report a first case of a young female with a metastatic primary vesical adenocarcinoma to liver and lung at the time of diagnosis. This case emphasizes the challenge for urologists to differentiate urachal and primary adenocarcinoma of the bladder preoperatively.
Case Report
A 25 years old female patient without prior medical history was referred to our hospital for painless hematuria. Blood tests and physical examination were normal. At cystoscopy, a bleeding necrotic mass arising from the bladder dome was found without any other lesion of the urothelium. Cytology revealed an adenocarcinoma. A computed tomography (CT) scan confirmed the mass of the bladder dome extending to the abdominal wall and showed multiple liver metastases and one pulmonary metastasis of the right lower lobe (Figure 1). Urachal adenocarcinoma was suspected because of the typical localization of the primary tumor. A partial cystectomy with en bloc urachectomy up to the umbilicus and bilateral pelvic lymph node dissection was performed. Histological results showed a muscle-invasive mucinous adenocarcinoma, 7.5 cm in length, without infiltration of urachal remnants (Figure 2). Because of the presence of glandular cystitis, villous adenoma with intestinal metaplasia and absence of tumoral infiltration of the urachus, the tumor was considered as a primary vesical adenocarcinoma (Figure 3). Two abdominal but no pelvic lymph node were invaded. TNM staging was pT3a, pN2, M1, G2–3, R0. Since the tumor presented histological features of the digestive tract, a palliative chemotherapy protocol consisting in bevacizumab, oxaliplatin, 5-fluorouracil and folinic acid was started.
Computed tomography scan shows a mass arising from the bladder dome, compatible with a cancer of the urachus.
Gross appearance of the tumor which measured 7.5 cm of length with no involvement of the abdominal wall.
Glandular cystitis adjacent to a villous adenoma with high grade dysplasia and infiltrating adenocarcinoma.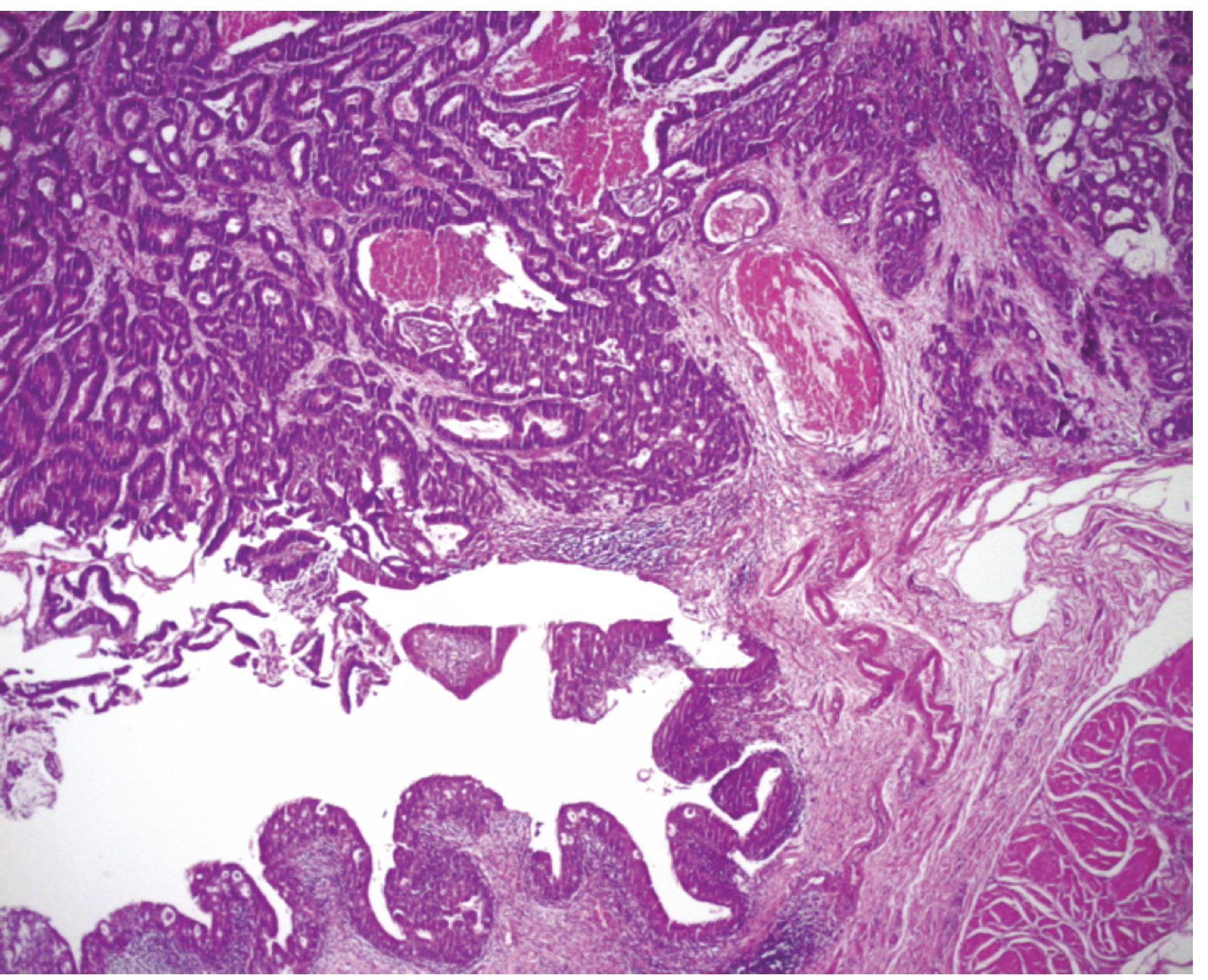
CT scan at 3, 6, 9, 12 and 15 months showed regression of hepatic metastases, unchanged pulmonary metastasis and no new metastasis while treated with 5 fluoro uracil, bevacizumab and folinic acid.
Discussion
Urachal and primary vesical adenocarcinoma are two different tumors, but the importance of this distinction for the management and survival is debated. Urachal adenocarcinoma seems to have better survival rate than primary vesical adenocarcinoma. Unfortunately, heterogeneity exists in published data, with regards to treatment modalities (margin status, adjuvant therapy, extent of node dissection) and patient's inclusion criteria. Therefore, careful interpretation of results is needed.2,7 Because of the anatomical difference, surgical management is different: radical cystectomy is performed for primary bladder adenocarcinoma whereas partial cystectomy with en bloc urachectomy up to the umbilicus is considered the gold standard for the treatment of urachal carcinoma. Staging at cystectomy is considered the strongest predictor of mortality. Reported 5-year overall survival rate is poor because the diagnosis is late when the tumor is often locally advanced and has spread systemically. Moreover adjuvant treatment has low efficiency. Adenocarcinoma is known to be radioresistant and there is no approved chemotherapy protocol.8–10
The case of this patient is very unusual for her age and clinical history. The radiological and clinical features mimicked an adenocarcinoma of the urachus. The pathologic result was unexpected. The operation performed was not the procedure normally performed in primary adenocarcinoma of the bladder. In this situation, with the patient's consent, palliative chemotherapy was undertaken. After a 15 month follow-up, the patient is free from local recurrence or new metastasis contrary to expectancy. Nevertheless since surgical management is different for urachal and non urachal adenocarcinoma, we believe that when a mass at the dome of the bladder is found, an extensive transurethral resection of the bladder should be always performed to differentiate these two close tumors.
Footnotes
Acknowledgements:
the authors have no substantial direct or indirect commercial or financial incentive associated with publishing this article. The authors alone are responsible for the content and writing of the paper.