
Abstract
Basal cell adenocarcinoma is a low-grade malignancy of the salivary glands. Basal cell adenocarcinoma of the minor salivary gland is an extremely rare disease that originates from the maxillary sinus. The histopathological characteristics of basal cell adenocarcinomas are similar to those of basal cell adenomas. However, basal cell adenocarcinomas can be differentiated from basal cell adenomas based on their tendency to invade surrounding tissues. Surgical resection is the first-line treatment for basal cell adenocarcinomas. An 86-year-old man underwent operations for a maxillary sinus tumor twice in our department. The pathological results of the tumor at both times revealed basal cell adenoma. After 4 and 5 years since the last operation, the tumor recurred, and the patient was treated with partial maxillectomy using Weber–Ferguson incision. We observed invasions to the surrounding tissue, and based on immunohistochemical findings, the patient was diagnosed with basal cell adenocarcinoma. Herein, we present an extremely rare case of basal cell adenocarcinoma arising from the maxillary sinus, in detail.
Introduction
Basal cell adenocarcinoma (BCAC) is a rare tumor of the salivary gland that most commonly affects the parotid gland. BCAC of the major salivary gland was first reported by Ellis and Wiscovitch. 1 Since then, only three cases of the development of BCACs in the maxillary sinus have been reported.2,3 BCACs often invade the maxillary sinus from the palate and buccal mucosa and rarely develop from the maxillary sinus independently because minor salivary glands are most frequently recognized in the buccal mucosa and hard palate. Similarly, paranasal BCACs probably originate from minor salivary gland tissue; however, the distribution of the minor salivary gland in the maxillary sinus is unknown. BCAC is histologically similar to basal cell adenoma (BCA), and its differentiation can be particularly challenging with small biopsy specimens. According to the fourth edition of the World Health Organization Classification of Tumors, BCACs are classified as low-grade adenocarcinomas with favorable prognoses. 4 Minor salivary gland tumors tend to infiltrate surrounding tissues, thereby requiring wide local excision to ensure complete resection. Herein, we present a rare case of BCAC arising from the maxillary sinus.
Case
An 86-year-old man underwent operations for maxillary sinus tumor in 2016 and 2017 in the Department of Otorhinolaryngology—Head and Neck Surgery. The first procedure for excision was the Denker operation, and the second was endoscopic surgery. The pathological results of these tumors were BCAs.
In 2019, the patient developed diplopia, frequent epistaxis, and buccal swelling, and a tumor recurred in the left maxillary sinus. The orbital floor bone was affected due to tumor invasion.
Based on these findings and the patient’s clinical course, the clinical diagnosis was a left maxillary carcinoma with a TNM Classification of Malignant Tumors of cT4aN0M0. We recommended extended excision; however, the patient requested to preserve his left eyeball. Therefore, we decided to perform partial maxillary resection and recommended postoperative radiotherapy. Partial maxillary resection was performed via Weber–Ferguson incision. The maxilla had not been infiltrated by the tumor and thus was reserved. The tumor had partially invaded the orbital floor bone; thus, the orbit floor and orbital fat were partially resected. Pathological findings revealed malignant atypical cells and stroma infiltrations (Figure 1(a)); however, because the tissue had a palisading pattern similar to BCA (Figure 1(b)), we diagnosed the tumor as BCAC. The tumor had a solid-type structure, and the tumor cells with mitosis (Figure 1(c)) were significantly fragile, making it difficult to judge the surgical margin. We recommended radiotherapy in our initial treatment plan; however, the patient was reluctant for radiotherapy.
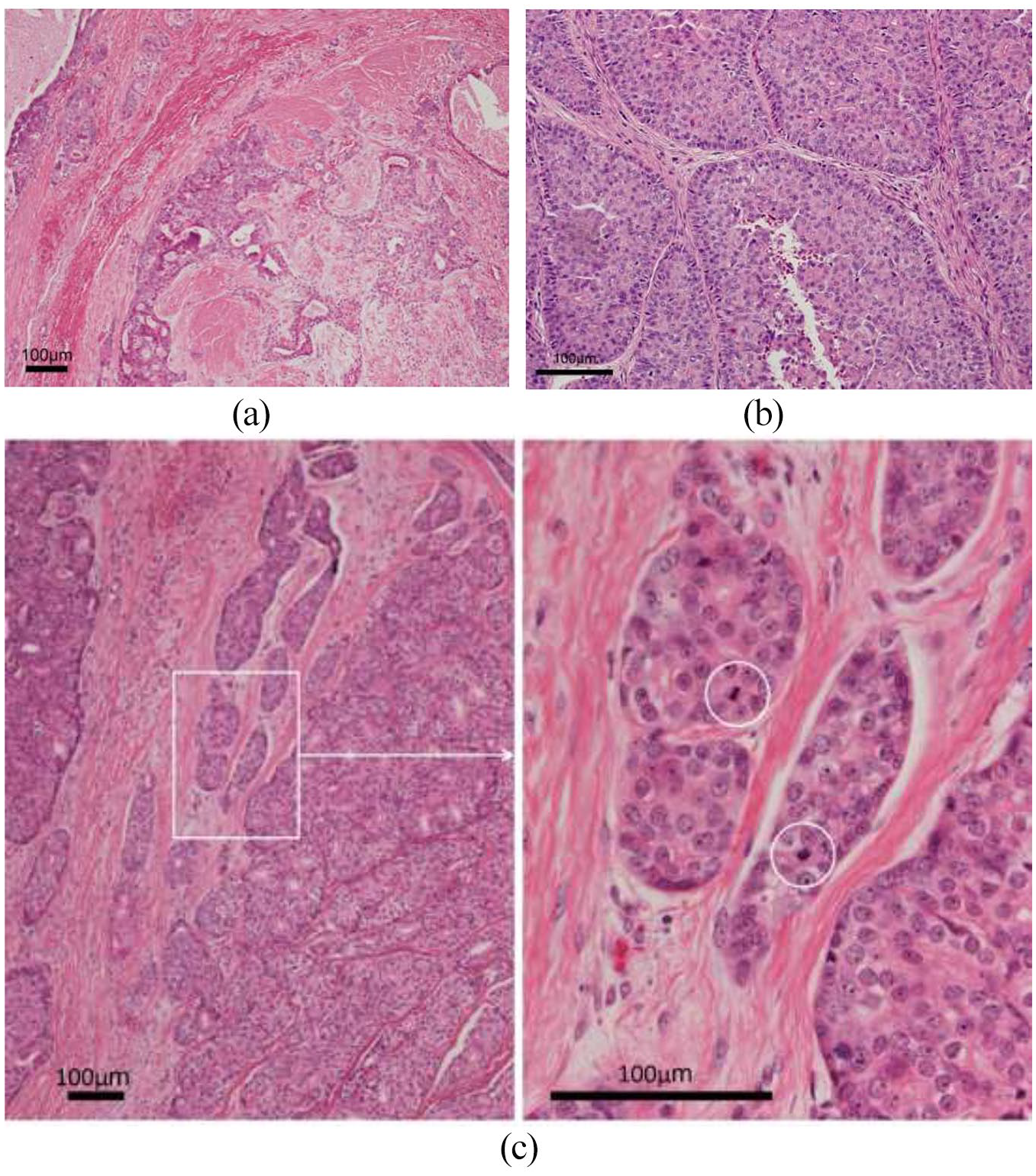
Photomicrographs of a hematoxylin and eosin-stained tissue section revealing: (a) tumor infiltration into the surrounding tissue (4× field of view). (b) Palisading of tumor cells (10× field of view). (c) Tumor showing solid growth pattern and mitotic figures (4×, 20× field of view).
In 2021, since a tumor recurred in the nasal septum and maxillary sinus with bleeding, paranasal computed tomography with contrast effect showed the tumor in the left maxillary sinus and its recurrence in the orbital floor (Figure 2(a)). Therefore, we resected it by partial maxillary resection using Weber–Ferguson incision. The tumor infiltrated the orbital floor bone (white arrow), as in the last operation (Figure 2(b)). The histopathological findings showed malignant atypical cells and stroma infiltrations (Figure 3(a)), and the Ki-67 labeling index was 25% (Figure 3(b)). Tumor cell membranes were diffusive and positive for epidermal growth factor receptor (EGFR) (Figure 3(c)). The tumor cells were negative for p53 (Figure 3(d)) and B-cell lymphoma-2 (bcl-2) (Figure 3(e)). Currently, the patient is undergoing postoperative radiotherapy.

Computed tomography (CT) and intraoperative view in 2021: (a) paranasal CT finding in 2021: CT revealing the tumor in the left maxillary sinus and orbital floor and (b) intraoperative view showing partial maxillary resection using a Weber–Ferguson incision; the tumor infiltrates the orbit (white arrow).
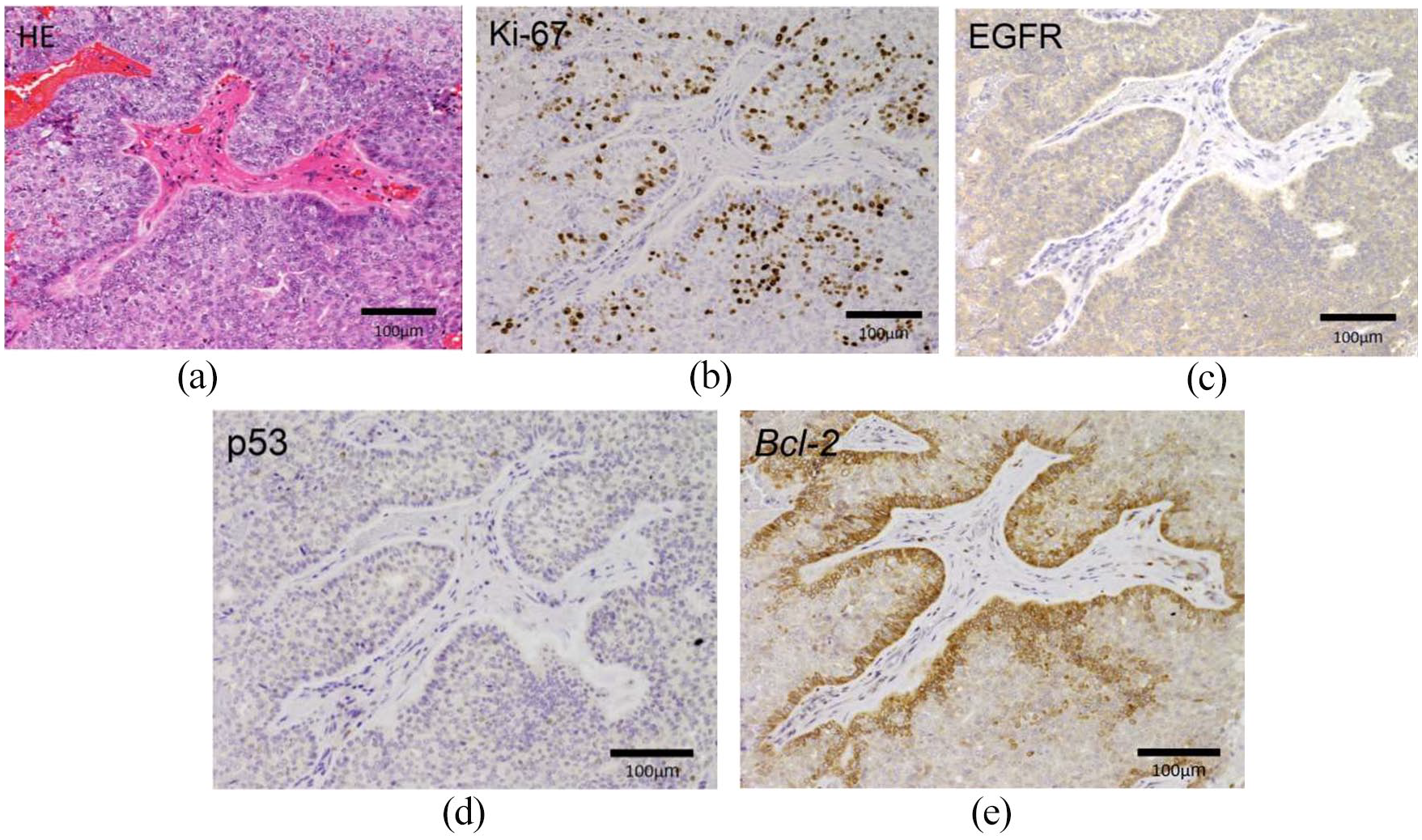
Immunohistochemical findings: (a) hematoxylin and eosin–stained sections (20× field of view). (b) Ki-67 labeling index is 25% (20× field of view). (c) Epidermal growth factor receptor is positive in the tumor cell membrane (20× field of view). (d) p53 is negative in the tumor cells (20× field of view). (e) B-cell lymphoma-2 is negative in the tumor cells (20× field of view).
Discussion
The incidence of malignant salivary gland tumors is approximately ⩽3%, 5 with nearly 90% of such tumors developing in the parotid gland.1,5 The incidence of palatal BCACs as malignant tumors in the minor salivary glands ranges from 0.26% 6 to 1.2%. 7 BCAC commonly occurs in people aged approximately 60–70 years with similar frequency in men and women. 1 Cuthbertson et al. have reviewed 72 cases of BCACs arising in the minor salivary glands and reported that the palate was the most common location with a high local recurrence rate (41%). Among 72 cases, only seven had BCACs localized in the nasal cavity and sinuses. 8 To our knowledge, only three cases of BCACs arising from the maxillary sinus have been reported so far;2,3 thus, BCAC in the maxillary sinus is extremely rare.
Two distinct cell populations are apparent in BCAC. The predominant cell type has small, round- to ovoid-shaped elements. The nucleolus is dark and hyperchromatic. The other cell type has larger elements and a clear or slightly eosinophilic cytoplasm. 2 A palisading pattern is observed in tumors, and the tissue structure of these tumors is similar to that of benign BCAs. Depending on the dominant tumor patterns found in the tissue, tumors are structurally classified into solid, tubular, trabecular, or membranous. 1 The solid type is the most common and was observed in our case. The possible differential diagnoses include BCA, adenoid cystic carcinoma, small-cell carcinoma, and metastatic basal cell carcinoma, with the primary tumor originating from the skin. The differentiation of BCACs from BCAs is based on invasive proliferation into the nerves, blood vessels, and surrounding tissues, necrosis, mitotic figures, and anisonucleosis.4,9 Invasive proliferation into the nerves and blood vessels is observed in 25%–35% of BCAC cases. 10 Both BCACs and BCAs differentiate into myoepithelial cells, making it impossible to differentiate these tumors based on immunohistochemical findings alone. However, Nagao et al. 5 have reported that higher cell proliferation rates (>4 mitotic counts/10 high-power field or 5% of the Ki-67 labeling index) and apoptosis with increased p53 and EGFR expression and a loss of bcl-2 expression are markers for diagnosing BCACs. We performed immunohistochemical analysis for the specimen obtained during the last operation; the tumor cells were only immunoreactive with EGFR. Results for p53 and bcl-2 were negative. The Ki-67 labeling index was 25% (excluded p40-positive peripheral cells of the tumor). These findings coincided with BCAC; however, the most important diagnostic factor for distinguishing BCAC from BCA was the infiltrative growth pattern. Although BCAC is histopathologically classified as low-grade adenocarcinoma, BCAC arising in the minor salivary glands has local recurrence, distant metastasis, and mortality rates of 71%, 21%, and 29%, respectively. 10 The first-line treatment of BCAC is wide local excision with safety margins. Biopsy alone might not be able to correctly diagnose small salivary gland tumors originating from the paranasal sinuses; hence, treatment may require multiple operations, similar as in our case. As there was no invasive evidence of tumor in the pathologic finding of 2017 and 2016, we had to diagnose BCA. Malignant tumors in the maxillary sinus may easily infiltrate the orbit because the orbital floor bone separating the two structures is thin. It might be BCAC from the onset because the border site tissue might not be resected by surgery. Therefore, ensuring that the tumor is completely resected with a good operating field (e.g. Weber–Ferguson incision) is important because malignant transformation may have occurred since the initial surgery. When BCACs invade the orbit, eyeball preservation is not possible during extended resection. Expectedly, the problem of facial configuration and some patients are reluctant for surgery. We think that it is very likely to be the relapse of stump about tumor which we resected in 2021. It is unclear whether radiation therapy has a role in managing BCAC; however, it can be effective if the surgical specimen margin is close or has local recurrence. 11 Sarath et al. 12 have reported a patient with an inoperable maxillary BCAC who favorably underwent radiotherapy, followed by chemotherapy. Furthermore, successful local control and quality-of-life maintenance have been reported with radiotherapy alone. 13 Originally, it was considered preferable to perform postoperative radiotherapy; however, patient consent was not obtained in 2019. Since the lack of radiotherapy might lead to a second recurrence, currently, we strongly recommend radiotherapy.
Conclusion
We present a rare case of BCAC arising from the maxillary sinus of the minor salivary glands. Our case is a typical case of the difficulty in pathological diagnosis, in which the tumor was diagnosed twice (as a BCA before a BCAC was rendered). The Weber–Ferguson incision effectively enabled easy partial maxillectomy, and adjuvant radiotherapy has been used successfully for invasive tumors and local recurrences.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Japan Society for the Promotion of Science KAKENHI (grant no: 20K09721 to S.I.).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.