
Abstract
Renal cell carcinoma (RCC) accounts for 3% of all cancers in adults. The indications for Radiofrequency Ablation (RFA) for renal carcinomas include T1a (tumor 4 cm or less, limited to the kidney), elderly patients, renal impairment, comorbidities, poor surgical candidate, and multiple bilateral renal masses. We retrospectively reviewed medical records, specifically investigating the indications, complications and outcomes of RFA and nephrectomy for treatment of RCC in a tertiary medical center with a predominantly Hispanic patient population. Forty-nine patients with RCC were evaluated. Nine patients had RFA, 9 had partial nephrectomy and 31 had radical nephrectomy. All patients among the 3 groups had stage T1N0M0 RCC at diagnosis. Tumor recurrence was observed in 2 (22%) patients that had RFA, one (11%) patient that had partial nephrectomy and no patients that had radical nephrectomy. One patient had recurrence of the tumor at the opposite kidney pole from the initial RFA site 4 years later. This particular patient did not have any tumor recurrence at the site of the initial RFA. A second RFA was performed on the recurrent tumor with no recurrence upon subsequent follow up visits. The second patient had recurrence of the RCC on 1 year follow that was discovered to be sarcomatoid RCC, which is an aggressive type with a poor prognosis. Our results support the clinical utility of RFA in patients with stage T1 RCC who are poor surgical candidates or those with reduced renal function. The clinical utility of RFA as an equally effective approach when compared to partial nephrectomy in patients with stage T1 RCC that meet strict indications for the procedure. The treatment choice should be individualized and based on the characteristics of the renal tumor such as size, location and histological type of RCC. We conclude that RFA presents a safe treatment choice for patients with RCC if long term follow up is maintained.
Introduction
Approximately 64,000 cases of renal cell carcinoma (RCC) were diagnosed in the United States in 2013. 1 RCC accounts for 3% of all cancers in adults, more commonly seen in males and in the sixth to eight decade in life. 2 RCC originates within the renal cortex and accounts for 80-85% of all primary renal neoplasms. The detection rate of RCC has increased in recent years due to increased use of cross sectional imaging. The majority of incidentally diagnosed RCC tends to be small with a low histological grade and decreased incidence of metastasis. 3 Surgical intervention has been the mainstay therapy for patients without metastatic RCC. Treatment usually consists of a radical nephrectomy or other renal sparing options such as partial nephrectomy or ablative techniques. The current census is that smaller renal tumors of ≤4 cm (T1a) are more appropriately treated with minimally invasive procedures of thermal ablation or partial nephrectomy to preserve renal function and avoid the unnecessary complications of surgery. Radical nephrectomies have been shown to have a higher incidence of chronic kidney disease and increased morbidity and mortality. In recent years, radiofrequency ablation (RFA) has emerged as a safe and effective treatment option for small renal tumors with good oncological outcomes. 4
Principles of Radiofrequency Ablation
Radiofrequency ablation delivers a high-frequency (460-500 kHz) alternating current into the tumor by means of a radiofrequency ablation electrode. Electrodes can be placed directly into the tissue either laparoscopically or percutaneously through the use of ultrasound, computed tomography (CT), or magnetic resonance guidance. The concept of RFA is the transfer of alternating monopolar radiofrequency electrical current through needle electrodes into target tissue that results in ionic agitation, heating, and eventual desiccation with subsequent coagulative necrosis.5,6 Irreversible cell damage is time and temperature dependent. Temperatures ranging from 45-50°C cause a denaturation of cellular enzymes and damage membrane channels. 7 Coagulative temperatures (55-100°C) result in structural protein denaturation, vascular congestion, and irreversible cell damage. 7 Another effect of these high temperatures is microvascular and arteriolar occlusion that leads to ischemic injury of the tissue. The necrotic tissue is eventually resorbed through fragmentation and phagocytosis that transforms the tissue into avascular scar.
RFA has several advantages compared to partial or radical nephrectomy, including preservation of kidney function, decreased morbidity and minimal duration of postoperative recovery.8,9 Percutaneous RFA is less invasive and can be done safely under moderate sedation. Nephron sparing treatment can postpone or avoid the need for dialysis in the future. However, it is viewed as an attractive option to avoid the morbidity associated with surgery and offer an effective curative treatment option. The indications for RFA of renal tumors include stage T1a (defined as a tumor 4 cm or less, limited to the kidney), elderly patient, renal impairment, multiple comorbidities, poor surgical candidate or multiple bilateral renal masses. Contraindications to RFA include central or hilar tumors, acute illness or infection, unstable cardiovascular status, poor life expectancy, metastasis and irreversible coagulopathy.
Several factors affect the outcome of RFA: tumor size and location; tissue impedance; ablation time; as well as the amount of energy delivered and surface area of the electrodes. 10 RCC that are less than 3 cm are excellent for ablation and can be treated in a single session. However tumors between 3.0-3.5 cm in diameter may require multiple ablations and sessions. The efficacy is 90% for RCC smaller than 3 cm but lowers steadily as the tumor size increases. Current RFA systems produce a diameter of local necrosis of 1 to 5 cm around the tumor in a single treatment. 11 Larger tumors will require multiple overlapping ablations. Several studies have demonstrated that the large tumor size is prognostic for recurrence after RFA. 12
Tumor location can also affect the ablation results. RCC are described as being either exophytic, central or mixed based on the location.
11
Exophytic tumors are described as extending beyond the renal parenchyma and thus being in contact with the perirenal fat. Central tumors are defined as tumors that extend into the renal sinus but not peripherally into the renal parenchyma. Mixed tumors are tumors comprised of components in the renal parenchymaand involving the perinephric fat. Tumors that are exophytic are almost always treated successfully in only one RFA session.
13
Centrally located tumor poses a more difficult challenge for successful ablation. Centrally located renal tumors are located near large vessels that do not favor temperature rise to therapeutic levels because of heat dissipation.12,14 Therefore, centrally located tumors have a higher rate of tumor recurrence. In large or centrally located RCCs preablation embolization of the tumor could reduce tumor vascularization and increase success of ablation. RFA is a novel minimally invasive therapeutic approach that can be offered to patients with small renal tumors or have significant comorbidities precluding surgical resection.14,15 Veltri
The objective of this research study was to determine if the tumor recurrence was significant among the different treatment modalities of RFA, partial or radical nephrectomy for stage T1 RCC. If tumor recurrence was observed, then further investigation was done to determine which influential factors favor tumor recurrence. RFA is an attractive option in the management of RCC; however there is limited medical in the investigation of the outcomes of the RFA versus partial or radical nephrectomy in the treatment of stage T1 RCC. There is also a scarcity of data on the treatment of RCC in predominantly Hispanic patients.
Materials and Methods
A retrospective medical chart review was performed on all patients diagnosed with RCC that had either radiofrequency ablation, partial or radical nephrectomy for RCC between the period of January 1, 2008 through December 31, 2012 at the Texas Tech University Health Sciences Center (TTUHSC) of El Paso, Texas and its affiliated hospital, University Medical Center (UMC) of El Paso. The research study was approved by the institutional review board (IRB) of TTUHSC of El Paso, Texas. Only patients that had with histologic confirmation of RCC and a post-treatment follow-up of with radiographic imaging were considered. We identified a total of 49 patients with histologically confirmed RCC. Of these 49 patients, 9 had RFA, 9 had partial nephrectomy and the remaining 31 patients had a radical nephrectomy. The data collected pertained to patient demographics, laboratory tests, indications and type of therapy (RFA, partial or radical nephrectomy), operative or post-operative complications and tumor recurrence. Percutaneous renal biopsy of the renal tumor was performed to establish the histopathological diagnosis of RCC before treatment. Tumors were staged according to the American Joint Committee on Cancer TNM system. Renal tumor location was classified as exophytic, central or mixed. All patients were evaluated by an oncologist and were referred for evaluation to interventional radiology for RFA or urologist for a partial or radical nephrectomy. The RFA approach was done percutaneously whereas the partial or radical nephrectomy was performed laparoscopically or as an open procedure. The decision of which therapeutic surgical approach to use was based on tumor size, location, clinical judgment of the urologist and patient preference.
Radiofrequency Ablation Procedure
Radiofrequency ablation procedure was performed under Monitored Anesthesia Care (MAC) sedation and local anesthesia. Tumors were imaged prior to RFA using contrast-enhanced computed tomography (CT) (Figure 1A,B). Percutaneous RFA was performed using CT guidance for tumor visualization to guide probe placement. RFA treatment sessions were performed with impedance controlled pulsed current from a 200 W RF 3000 generator (Boston Scientific, MA, USA). RFA was performed with a varying size (3, 3.5 or 4 cm) umbrella-shaped multi-tines needle electrode (LeVeen CoAccess RFA needle electrode, Boston Scientific, MA, USA), selected to match the size of the tumor. A 15-gauge LeVeen radiofrequency needle tines was inserted under CT-guidance from a posterior percutaneous approach and into the center of the tumor. The RF electrodes were inserted into the tumor through the normal renal parenchyma to minimize the risk of hemorrhage and tumor seeding.

Axial (A) and sagittal (B) images from a contrast enhanced computed tomography demonstrate a 1.3 cm exophytic mass extending from the cortex or the upper pole of the left kidney into the adjacent perinephric fat (Green Arrows). Axial (C) and sagittal (D) images obtained 2 yr and 2 months post ablation demonstrate scaring in the renal cortex and adjacent perinephric fat without residual or recurrent enhancing mass (Blue Arrows).
During RFA, the number of overlapping ablations was dependent on the size and shape of the tumor. The timing of individual ablation was impedance controlled, which depends on the tissue vascularity and resistance. RCC target tissue cell death is achieved via tissue desiccation and consequently loses its ability to conduct current, hence the rise in the impedance. The term
Partial or Radical Nephrectomy
Partial nephrectomy involves the complete removal of a localized renal tumor. This approach maintains the normal renal parenchyma. Several advantages of partial nephrectomy compared to radical nephrectomy includes the preservation of renal function, reduced risk of chronic kidney disease, and the avoidance of unnecessary aggressive approach for small renal masses. 9 Radical nephrectomy includes the removal of the tumor bearing kidney and has been the usual approach for localized RCC in patients with a normal contralateral kidney.
Follow Up
Patient follow-up after RFA and nephrectomy included periodic history and physical, chest radiograph, contrast-enhanced abdominal CT (Figure 1C,D) or MRI, serum chemistries, and liver function tests. These studies were obtained at 6 months, 12 months, and yearly thereafter. The follow-up routine was every 3 to 6 months for each patient that had a nephrectomy but varied only according to the surgeon's preference and imaging findings. The clinical outcome was assessed based on follow up imaging studies to evaluate for recurrence of the RCC. Tumor recurrence was defined as local tumor progression described by the appearance of tumor enhancement on contrast enhanced CT imaging or magnetic resonance imaging (MRI). Tumor recurrence could be present at same or another portion of the kidney or even metastasis to other organ systems. Disease-free survival (DFS) describes the proportion of patients with no disease at last follow-up including both locally recurrent disease and evidence of metastases.
Statistical Analysis
Most results were expressed as mean or percentage. Descriptive statistics such as means and percentages were used for continuous and categorical data respectively. Data were described using appropriate summary measures. Categorical variables were compared across three treatment groups using Fisher's exact test while normal continuous measures were compared using one way analysis of variance (ANOVA). Non normal variables were compared using Kruskal Wallis test. In the
Results
A total of 49 patients were diagnosed and treated for stage 1 RCC with either radiofrequency ablation, partial or radical nephrectomy (Table 1). Of these 49 patients, 9 (18.5%) had RFA, 9 (18.5%) had partial nephrectomy and the remaining 31 (63%) patients had a radical nephrectomy with an overall mean age of 53, and 67% males. Thirty-nine (80%) patients were Hispanic, 9 (18.5%) Caucasian and 1 (2.5%) Asian. Most common comorbidities were hypertension (47%) and diabetes (22%). Further univariate and multivariate statistical analysis of variables across the three groups: RFA, partial nephrectomy and radical nephrectomy (Tables 2–4)
Patient demographics and tumor characteristics.

RCC, renal cell carcinoma
Univariate analysis: comparison of continuous and categorical variables across the three groups: radiofrequency ablation, partial nephrectomy and radical nephrectomy.
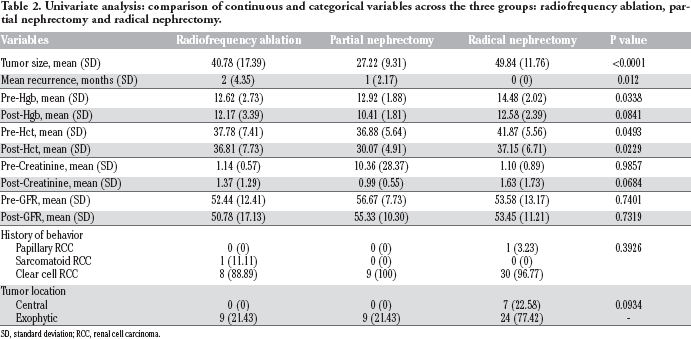
SD, standard deviation; RCC, renal cell carcinoma.
Comparison of changes in pre and post measures between three treatment groups.

SD, standard deviation.
Multivariable analysis: baseline cofactors associated with different treatment groups in multivariable analysis.

OR, odds ratio; CI, confidence interval.
Radiofrequency Ablation
Nine of the 49 patients had radiofrequency ablation of the RCC based on strict indications for the procedure (Table 5). These patients had a mean age of 51 with 5 males and 4 females. Seventy-eight percent of the patients were Hispanic and 22% were Caucasian. Most common comorbidities were hypertension (67%) and diabetes (22%). Eight patients had histopathological confirmation of clear cell RCC and one patient with sarcomatoid RCC. The size of renal tumor for those patients that underwent RFA was established by CT imaging. These stage I (T1N0M0) RCC had an average tumor size of 3.6 cm with all being exophytic in location. No operative or post-operative complications occurred. Indications for RFA included stage 1 RCC (90%), renal insufficiency (30%) or a poor surgical candidate (40%). Two (22%) patients had recurrence of the RCC at follow up. One patient had recurrence of the tumor at the opposite kidney pole from the initial RFA 4 years later. This particular patient did not have any tumor recurrence at the site of the initial RFA. A second RFA was performed on the recurrent tumor with no recurrence of this upon subsequent follow up visits. The second patient had recurrence of the RCC at their 1 year follow that was discovered to have sarcomatoid RCC, which is an aggressive type with a poor prognosis.
Patient demographics, tumor characteristics and clinical outcome of those that had radiofrequency ablation.
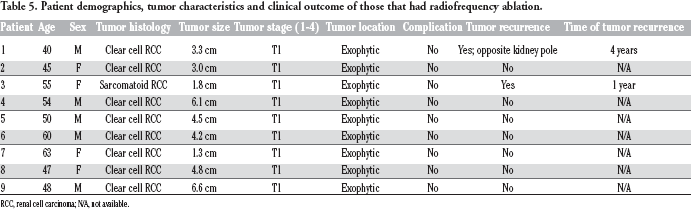
RCC, renal cell carcinoma; N/A, not available.
Partial or Radical Nephrectomy
The 9 patients that had a partial nephrectomy for stage 1 RCC, had a tumor size ranging from 1.5×1.3×1.0 cm to 2.5×2.5×2.0 cm. The size of the renal tumor in those patients that underwent a surgical intervention was established on pathological examination. All of these patients had histopathological confirmation of clear cell RCC and were exophytic in location. Three (33%) patients that underwent a partial nephrectomy had a significant amount of postoperative bleeding. Only one (11%) patient had local recurrence of the RCC at the 1 year follow up.
The remaining 31 patients that underwent a radical nephrectomy for their stage 1 RCC, had a tumor size ranging from 2.2×2.0×2.0 cm to 7.0×7.0×5.0 cm. Thirty patients had histopathological confirmation of clear cell RCC and one had papillary RCC. Twenty-four (77%) patients had an exophytic tumor and 7 (23%) had a centrally located tumor. Of these 31 patients, 4 (13%) had renal insufficiency, 12 (39%) had a significant amount of postoperative bleeding, and 1 (3%) had neuropathic pain after the nephrectomy. No patients had any postoperative infections or injury to surrounding abdominal structures. No patients had recurrence of the tumor that were stage 1 RCC and underwent a radical nephrectomy.
In a comparison, the tumor recurrence for stage 1 RCC in the RFA group was 22% compared to 11% for partial nephrectomy and 0% for radical nephrectomy. The 22% recurrence rate for RFA is considerably higher than previous studies. However, considering the observation that in one patient had recurrence of the tumor at a site other than at the initial ablation site and the other patient had an aggressive sarcomatoid RCC, the recurrence rate could be considered much lower.
Discussion
Partial nephrectomy is a nephron sparing surgery that is the gold standard in the treatment of RCC. 17 However, complication rate has been described to be as high as 30%.17,18 In comparison, the complication rate is lower in patients treated with RFA for RCC. Complications from renal RFA are primarily due to thermal damage to adjacent structures due to the small size of the kidneys. Hemorrhage is the most commonly reported complication following RFA of renal neoplasms. 19 Thermal energy from the RF electrode can damage any segment of the proximal renal collecting system that can lead to ureteral stricture and hydronephrosis. 19 Renal infection following RFA is rare. Neuropathic pain is a commonly reported side effect resulting from thermal irritation to nerves residing on the anterior surface of the psoas muscle, and can result in muscle pain and sensory disturbances. 19 Tumor seeding of the electrode tract is rare.
In 2005, Gervais
Psutka
Olweny
Conclusions
Our study represents a series of mostly Hispanic patients with renal cell carcinoma and their tumor and demographic characteristics. The major limitations of our research study are that it is a retrospective design and a small number of patients that received RFA compared to those that had a partial or radical nephrectomy. Having a small number of patients limits the statistical power of our results. Future research studies should be prospectively designed with strict indication criteria for RFA and long term follow up in these patients with RCC. This will help further define the efficacy of this therapy option versus other management alternatives. Despite these study limitations, our results support the clinical utility of RFA in patients with stage T1 RCC who are poor surgical candidates or those who have reduced renal function.
The clinical utility of RFA as an equally effective approach when compared to partial nephrectomy in patients with stage T1 RCC that meet strict indications for the procedure. Tumor recurrence after RFA was 22% compared to 11% for radical nephrectomy, but further investigation provides an interesting discovery that could change indications for RFA. Sarcomatoid RCC is a very aggressive tumor with a poor prognosis and no current studies have investigated the utility of RFA among the histological type of RCC. We suggest that the every RCC should be histologically confirmed and possibly excluding the aggressive types of RCC from undergoing RFA. The other patient with tumor recurrence had recurrence of the tumor at a site other than at the initial ablation site, therefore we can exclude this as an actual recurrence of the RCC that was ablated.
The treatment choice should be individualized and based on the characteristics of the renal tumor such as size, location and histology. The procedure is tolerated well and may be performed as an outpatient without the need for general anesthesia. Long-term results are lacking, with 5-year data needed for comparison with results from surgical resection. 28 RFA will continue to assume an increasingly greater role in management of RCC as more oncologic outcome studies are performed in support of this procedure. Those most likely to have a successful outcome with the least number of treatments are those with small exophytic located tumors with histological confirmation of clear cell RCC. We conclude that RFA presents a safe treatment choice for patients with RCC if long term follow up is maintained. The tumor recurrences can be treated safely and effectively with repeated RFA.