
Abstract
Objective
To investigate anatomical variations in the renal arteries of patients with renal cell carcinoma (RCC) using computed tomography angiography (CTA).
Methods
Patients diagnosed with RCC were evaluated using CTA prior to undergoing laparoscopic nephrectomy. Any anatomical variations of the renal arteries on the side affected by the RCC were recorded. The CTA results were compared with the observations made during surgery and those produced by conventional digital subtraction angiography.
Results
A total of 107 patients with RCC were enrolled in the study. Multiple renal arteries were found in 11 patients (10.3%). Accessory renal inferior polar arteries were the most common type of multiple renal arteries. Multiple renal arteries acting as the feeding arteries to the RCC were found in five patients (4.7%).
Conclusion
CTA can be used as part of the preoperative evaluation prior to laparoscopic nephrectomy to provide anatomical information about the presence of multiple renal arteries in the affected kidney of patients with RCC. This could help with planning the surgery and reducing surgical complications.
Keywords
Introduction
Computed tomography angiography (CTA) can accurately display the number, size, course and relationship of the renal arteries to the surrounding structures. 1 The accuracy of CTA approaches that of conventional digital subtraction angiography (DSA). 2 Several studies have investigated the preoperative evaluation of accessory renal arteries using CTA in order to determine the renal vascular anatomy in patients undergoing living donor kidney transplantation.3,4 Another study used CTA to investigate multiple renal arteries in patients with renal cell carcinoma (RCC). 5 Being able to evaluate the anatomical variation of multiple renal arteries in patients with RCC could enable surgeons to chose the most appropriate operational path before laparoscopic nephrectomy with the aim of reducing intraoperative complications from vascular injury. 6 To our knowledge, there have not been any published anatomical or radiological reports describing the anatomy prior to laparoscopic nephrectomy of different multiple renal arteries acting as the feeding arteries to the RCC.
The purpose of this study was to use CTA to investigate the anatomy of multiple renal arteries acting as the feeding arteries in RCC in order to observe: (i) the relationship between these feeding arteries and the surrounding structures; and (ii) to provide additional information that might highlight difficulties for the laparoscopic nephrectomy management.
Patients and methods
Patients
This study enrolled consecutive patients with RCC who were examined using CTA before laparoscopic nephrectomy at the Department of Urology and the Department of Oncology, First Affiliated Hospital of Henan University of Science and Technology, Luoyang, Henan Province, China between January 2008 and May 2011. Exclusion criteria for a laparoscopic approach were the presence of local organ involvement, caval thrombus or bulky regional lymphadenopathy (>2 cm). Patients that had tumours in both kidneys were also excluded.
Written informed consent was obtained from all study participants. The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital of Henan University of Science and Technology.
CTA scanning protocol
All CTA studies were performed using a 64-row multidetector CT scanner (GE LightSpeed VCT; GE Healthcare Biosciences, Milwaukee, WI, USA) using the automatic triggering system in the arterial phase. A nonionic contrast agent (60–80 ml) (iopromide [Ultravist® 300 or 370]; Schering Pharmaceutical, Guangzhou, China) plus 20 ml of physiological saline were injected through an 18-gauge cannula positioned in the antecubital vein at a flow rate of 3–5 ml/s by a dual head power injector (Liebel-Flarsheim™ CT 9000 ADV; Liebel-Flarsheim, Cincinnati, OH, USA). The monitoring point was set in the abdominal aorta, and the threshold was 100 Hounsfield units. For all patients, the arterial phase images were acquired within 25–30 s after intravenous injection of the contrast agent. The scanning parameters were as follows: 120 kV, 140 – 200 mA, 64 × 0.625 mm collimation, 0.16–0.24 pitch, 0.5 s per rotation, 250 mm field of view and 512 × 512 matrix. The scan included the entire kidney and upper pelvis including the iliac arteries.
CTA imaging reconstruction and evaluation
All CTA images were reconstructed into a slice thickness of 0.625 mm and then sent to an independent workstation (Advantage Workstation 4.3; GE Healthcare Biosciences). The reconstructed data from the arterial phase were displayed as volume rendering, maximum intensity projection and multiple planar reformations using three-dimensional rendering software version Voxtool 6.12.3 (Volume Viewer Plus; GE Healthcare Biosciences).
Two radiologists (W-H.G. and Y.H.) and two urologists (Z-W.G. and X-S.F.), who were blinded to the medical histories, reviewed all images using picture archiving and communications system workstations (Visionpacs 5.0.0; Intechhosun Company, Beijing, China). The images were evaluated particularly for the shape and position of multiple renal arteries and different feeding arteries to the RCC. The images were also used to provide additional information that might suggest difficulties for laparoscopic nephrectomy management. The final diagnosis was obtained by consensus between the two radiologists (W-H.G. and Y.H.) and two urologists (Z-W.G. and X-S.F.). The results of the CTA were compared with surgical observations or DSA findings.
DSA scanning protocol
DSA was performed by an interventional radiologist (D-S.C.) using a DSA system (Digitex Premier DAR 2400; Shimadzu, Kyoto, Japan). Angiography was performed through a right femoral arterial route puncture using the Seldinger technique with a 5-F pigtail catheter to inject 20–40 ml of iodinated contrast agent (iopromide [Ultravist® 370]; Schering Pharmaceutical) at a flow rate of 15 ml/s. The catheter was usually positioned at the level of the renal arteries. DSA images were obtained in the frontal, left and right oblique views to ensure optimal visualization of the renal arteries without superimposition.
Statistical analyses
All statistical analyses were performed using the SPSS® software package, version 12.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Pearson's χ2-test was used to evaluate the prevalence rates of multiple renal arteries in the right and left kidneys. A P-value < 0.05 was considered statistically significant.
Results
A total of 107 patients with RCC (64 men and 43 women; age range 34–81 years; mean ± SD age 56.27 ± 13.68 years) were studied with CTA before laparoscopic nephrectomy. There were 62 tumours in the right kidney and 45 tumours in the left kidney.
Among the 107 patients with RCC, 11 (10.3%) patients had multiple renal arteries on the side affected by RCC, including eight patients (12.9%; 8/62) with tumours on the right side and three patients (6.7%; 3/45) with tumours on the left side. There was no significant difference between the right and left sides (χ2 = 1.657; Pearson’s χ2-test). CTA showed double (eight patients) or triple (three patients) renal arteries originating from the abdominal aorta and feeding different kidney segments. Of these, one artery was the dominant renal artery with a larger diameter (mean ± SD diameter: the right side 5.62 ± 0.88 mm; the left side 5.83 ± 0.81 mm) originating from the aorta and entering the renal hilum. The other arteries had smaller diameters than the main renal artery, and were distinguished as either accessory renal hilar arteries or accessory renal polar arteries according to whether or not they entered the renal hilum (Figure 1).
Computed tomography angiography images of a 47-year-old woman with a renal cell carcinoma (RCC) in the left kidney showing double left renal arteries (arrows) originating from the aorta at different levels. The superior branch was the dominant renal artery that was the feeding artery for the RCC alone, and the inferior branch was an accessory renal hilar artery. Left image: posterior–anterior position volume rendering; right image: anterior–posterior position volume rendering. The colour version of this figure is available at: http://imr.sagepub.com.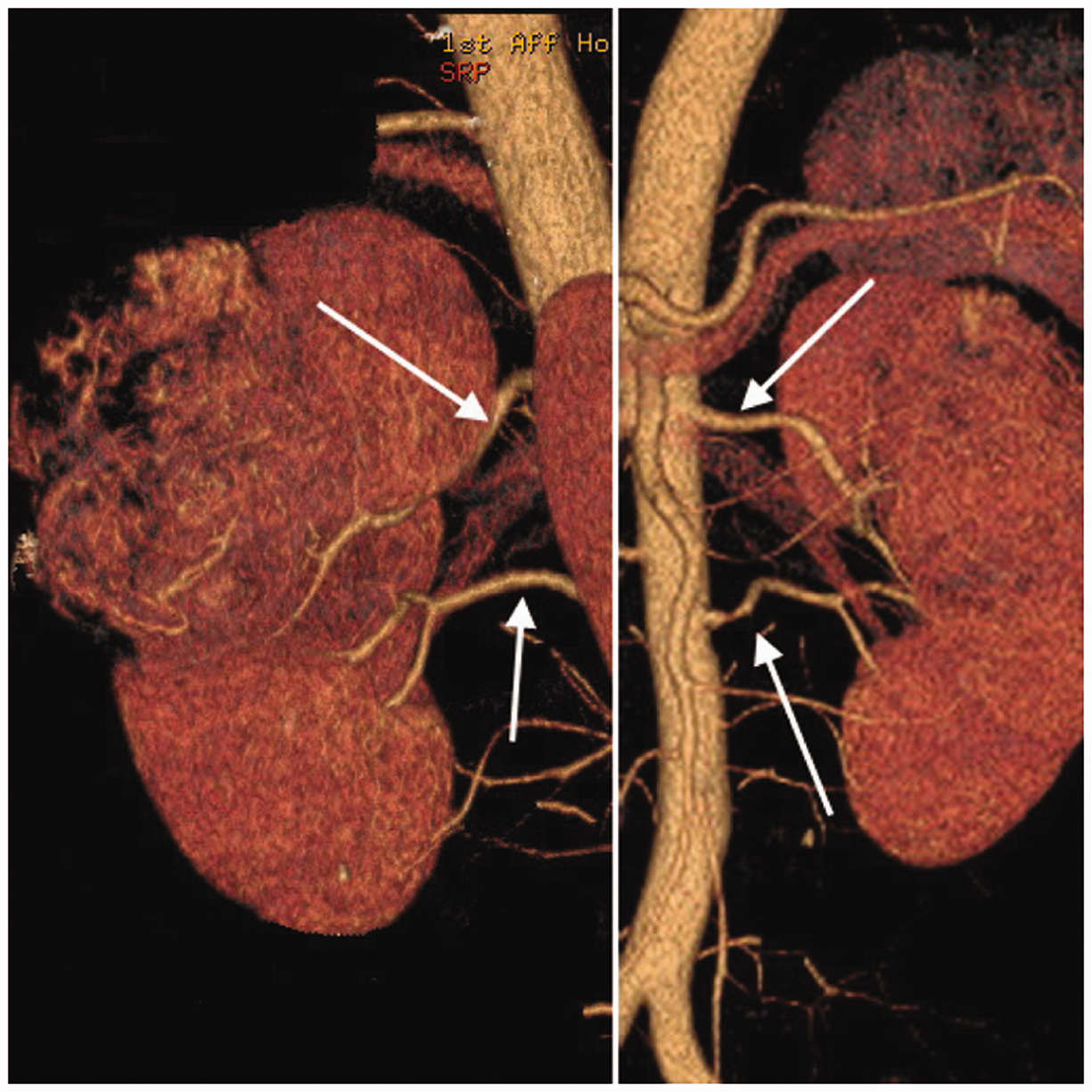
For patients with RCC in the right kidney (n = 8), there were double renal arteries in six right kidneys and triple renal arteries in two right kidneys. The two right accessory renal hilar arteries (mean ± SD diameter: 4.55 ± 1.34 mm) originated−8.9 mm to 8.6 mm above the right major renal artery and all passed posterior to the inferior vena cava (IVC). The eight right accessory renal inferior polar arteries (mean ± SD diameter: 3.00 ± 0.80 mm) originated 5.1 mm to 49.5 mm (mean ± SD: 29.44 ± 15.13 mm) under the right major renal artery. For the eight right accessory renal inferior polar arteries, 50% passed anterior to the IVC (Figure 2) and 50% passed posterior to the IVC (Figure 3). All of the variations were confirmed during surgery or as a result of DSA.
Computed tomography (CT) angiography images of a 57-year-old woman with a renal cell carcinoma (RCC) in the right kidney showing that there were three right renal arteries originating from the aorta at different levels (arrows). The intermediate branch was the main renal artery (arrow 2), which with the superior branch (arrow 1; an accessory renal hilar artery), formed the two feeding arteries to the RCC. The inferior branch was an accessory renal inferior polar artery (arrow 3), which passed anterior to the inferior vena cava. Left images: axial CT; right image: anterior–posterior position volume rendering. The colour version of this figure is available at: http://imr.sagepub.com. Computed tomography (CT) angiography images of a 53-year-old man with a renal cell carcinoma (RCC) in the right kidney showing that there was an accessory renal inferior polar artery (arrows) that passed posterior to the inferior vena cava. Upper image: axial CT; lower image: anterior–posterior inclined position maximum intensity projection.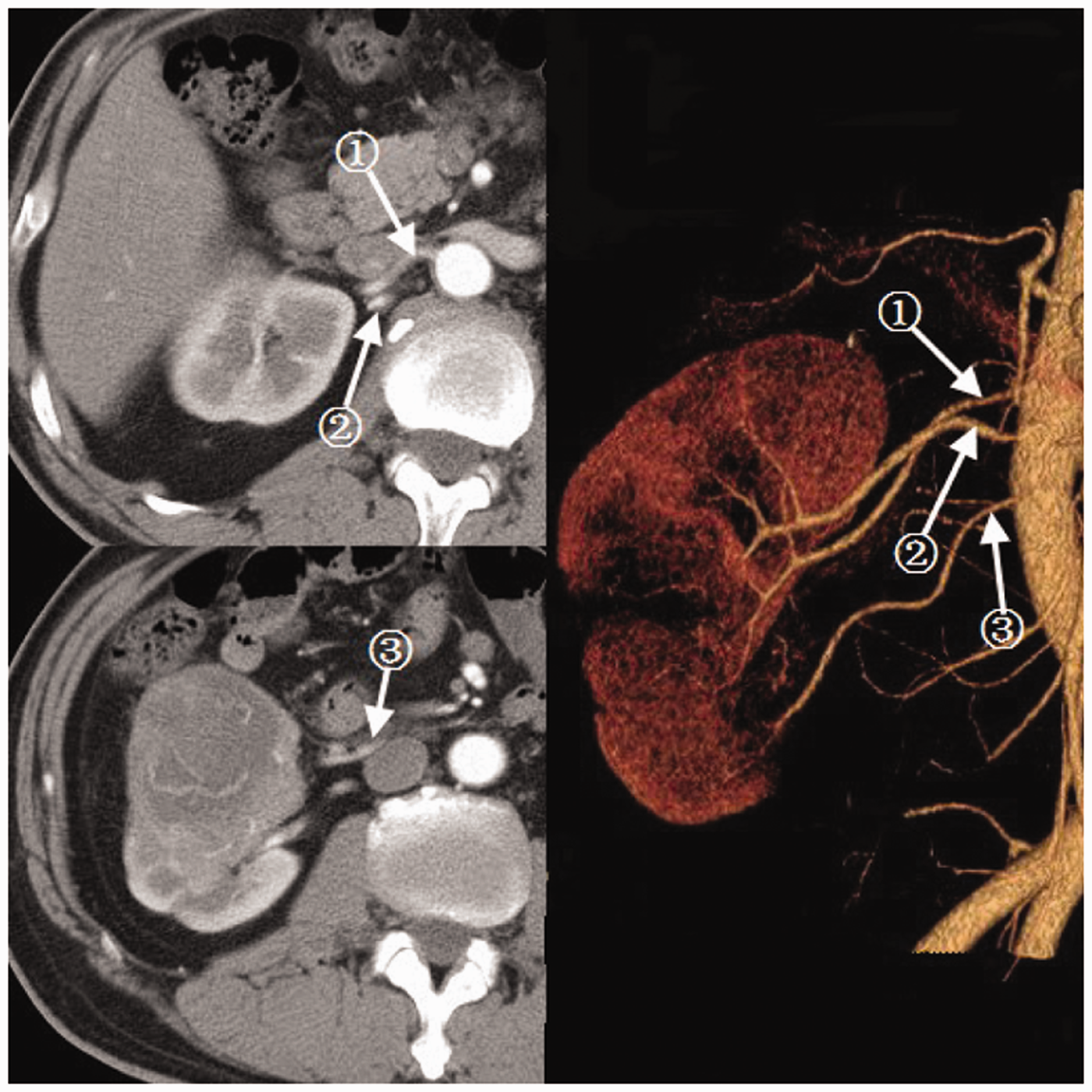

For patients with RCC in the left kidney (n = 3), there were double renal arteries in two left kidneys and triple renal arteries in one left kidney. The one left accessory renal hilar artery (diameter: 4.85 mm) originated 12 mm under the left major renal artery. The one left accessory renal superior polar artery originated 21.4 mm above the major renal artery that was incorrectly identified by CTA as a lumbar artery but confirmed as an accessory renal superior polar artery during surgery (Figure 4). The two left accessory renal inferior polar arteries (mean ± SD diameter: 3.07 ± 1.07 mm) originated 42.1 mm to 43.0 mm (mean ± SD: 42.55 ± 0.64 mm) under the left major renal artery.
Computed tomography angiography (CTA) images of a 65-year-old man with a renal cell carcinoma (RCC) in the left kidney showing that there was an accessory renal superior polar artery originating from the aorta 21.4 mm (arrows) above the major renal artery that was incorrectly identified by CTA as a lumbar artery but confirmed as an accessory renal superior polar artery during surgery. Upper image: anterior–posterior position volume rendering; lower image: anterior–posterior position maximum intensity projection. The colour version of this figure is available at: http://imr.sagepub.com.
One or two of the multiple renal arteries were also the feeding arteries of the RCC in five patients (4.7%; 5/107), which was 45.5% (5/11) of the total cases with multiple renal arteries associated with the RCC. There were three patients in which the RCC was supplied by a dominant renal artery plus an accessory renal hilar artery or an accessory renal polar artery (Figures 2 and 5); the RCC in one patient was supplied by an accessory renal hilar artery alone; and the RCC in one patient was supplied by an accessory renal inferior polar artery alone (Figure 6). Among these, four patients were confirmed by laparoscopy nephrectomy and one patient was confirmed by DSA.
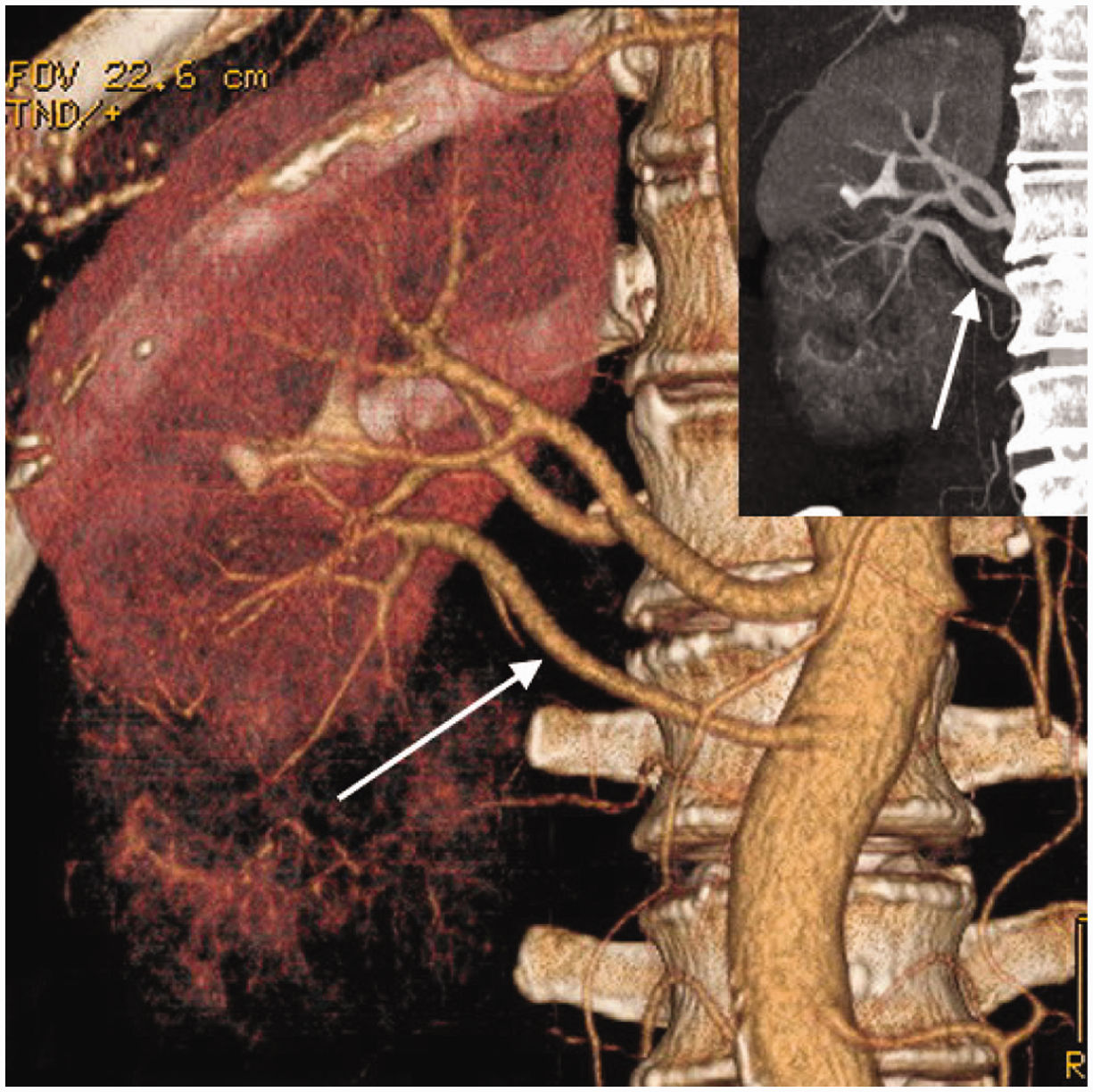
Computed tomography angiography images of a 75-year-old woman with a renal cell carcinoma (RCC) in the right kidney showing there was a smaller accessory renal inferior polar artery (arrow marked ‘A’) originating from the aorta and feeding part of the RCC (arrowhead). In the digital subtraction angiography image (inset), the part of the RCC supplied by the smaller accessory inferior polar artery was not stained with contrast agent (arrow). The colour version of this figure is available at: http://imr.sagepub.com. Computed tomography angiography images of a 54-year-old man with a recurrent renal cell carcinoma (RCC) in the right kidney following radical nephrectomy for RCC in the left kidney showing that there was an accessory renal inferior polar artery (arrows) originating from the aorta acting as the only feeding artery to the tumour. The maximum intensity projection image (inset) shows the part of the RCC supplied by the smaller accessory renal inferior polar artery. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
Each kidney is usually supplied by a single renal artery (70%) arising from the abdominal aorta at the level of the lumbar 2 vertebral body and each renal artery divides into four or five branches supplying different kidney segments.7,8 Renal artery variations including their number, source and course are very common.1,2 The variations can be divided into two groups: (i) multiple renal arteries; (ii) early branching of the renal artery. Multiple renal arteries constitute the most common renal artery variation, and they are distinguished as either a hilar artery (accessory renal artery) or a polar artery (aberrant renal artery) according to whether or not the artery enters the renal hilum; these renal artery variations can be seen in up to 25% of the normal population.2,8,9 Since the development of invasive interventions such as renal transplantation, interventional radiological procedures and urological surgery, an awareness of the possible variations of the renal arteries has been helpful for planning surgical procedures.1,3 The number of arteries, their sizes, and the locations of their origins on the aorta can be directly visualized using CTA, which can help surgeons make the most appropriate therapeutic decisions and provides useful preoperative information that can be used to plan the surgical procedures.1,3,9–11
RCC is the most common malignant tumour of the kidney, accounting for 85–90% of adult malignant renal tumours. 12 CT with a dynamic contrast enhancement protocol is an accurate method for the preoperative evaluation of RCC, providing exact tumour stage, which is the most important factor affecting the prognosis and survival of patients.13,14 Observing the tumour blood vessel morphology using CTA prior to laparoscopic nephrectomy could help to identify renal artery variations in the affected kidney, such as abnormal feeding arteries to the tumour. In this current study, multiple renal arteries associated with the presence of RCC were found in 11 patients (10.3%). This prevalence rate was lower than the rates found in normal groups included in previous studies that investigated renal artery variations, which might have been due to the fact that this current study investigated only the kidney that was affected by RCC and did not include any variations in the contralateral kidney.8,9,15,16 This current study found that there was no significant difference between the right and left kidneys, which is not in accordance with a previous report. 8 To our knowledge, multiple renal arteries acting as feeding arteries to the RCC have not been described in the anatomical or radiological literature. In this current study, multiple renal arteries acting as feeding arteries to the RCC were found in five patients (4.7%). A dominant renal artery, an accessory renal hilar artery or an accessory renal polar artery, alone or in combination, were observed to act as the feeding artery to the RCC.
Compared with open nephrectomy, the laparoscopic procedure offers advantages for the patient such as less time spent in hospital, reduced postoperative pain and less time spent convalescing. 17 Laparoscopic nephrectomy, including laparoscopic radical nephrectomy and laparoscopic partial nephrectomy, is widely used in the treatment of RCC. 18 Preoperative evaluation of the vasculature supplying the kidneys using CT aims to identify any abnormal structures that might affect the surgery and to minimize the incidence rate of surgical complications. 15 Prior knowledge of any renal artery variations, especially abnormal tumour-feeding arteries, is very important for planning the laparoscopic approach and surgical strategy. Whether undertaken as a transperitoneal laparoscopic nephrectomy or as a retroperitoneal laparoscopic nephrectomy, these types of less invasive surgeries must conform with established open surgical oncological principles. 17 Robson et al. 19 state that there should be sequential control of the renal arteries and veins before tumour manipulation in order to avoid cancer cell release into the systemic circulation as a result of intraoperative damage to the tumour.
For transperitoneal laparoscopic nephrectomy, with its broader operational view than that provided by retroperitoneal laparoscopic nephrectomy, the vessel variations can be easily identified during surgery. In this situation, preoperative evaluations using CTA focus on finding variant renal arteries that originate from the aorta at a greater distance than normal in order to identify the path taken by the artery and its relationship with the surrounding structures. Prior knowledge of any renal artery variations on the side affected by the RCC could help to determine where to make the surgical incision, and how to ligate the arteries easily and decrease the occurrence of intraoperative blood loss and other postoperative complications. For retroperitoneal laparoscopic radical nephrectomy, it is more important to undertake preoperative evaluations using CTA because the operational view and space are limited and there are fewer clear anatomical landmarks. 20 Prior knowledge of the starting locations and the pathways of multiple renal arteries is very important for planning laparoscopic nephrectomy. In this current study, the pathways taken by the accessory renal hilar arteries of the right kidney were unchanged, with all of them lying posterior to the IVC. In contrast, the pathways of the accessory renal inferior polar arteries of the right kidney were changed, with half passing anterior to the IVC and the rest passing posterior to the IVC. If the RCC tumour is small (<4 cm) and occupies an anatomically favourable position, then it may be removed by laparoscopic partial nephrectomy. Multiple renal arteries and the feeding arteries to the RCC must be confirmed in order to reduce the risk of intraoperative haemorrhage, segmental ischaemia and postoperative hypertension.21,22
A number of other factors can increase the difficulty of the laparoscopic nephrectomy. For example, in this current study, there was one case with congenital ureteral variation, two cases with renal vein variation, 11 cases with tumour thrombosis of the renal veins, and 19 cases with tumours located in the renal hilar or affecting the renal hilar structure. These factors should be explored further in a future study.
In conclusion, multiple renal arteries associated with RCC and variant renal arteries acting as feeding arteries to the RCC are not uncommon. The preoperative evaluation of the vascular morphology of the kidneys using CTA can provide accurate and important anatomical information. Prior awareness of any anatomical variations can help surgeons to plan the most appropriate surgical strategy in order to avoid any vascular complications during laparoscopic nephrectomy.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research was supported by a grant from the Plan for Henan Health Technology Innovation Talent Project and the Luoyang City Technology Bureau Scientific and Technological Projects.