
Abstract
Primary colorectal lymphoma is a rare malignancy accounting for 3% of all gastrointestinal lymphomas and 0.1-0.5% of all colorectal malignancies. Among primary colorectal lymphomas, the most common histological subtype of colorectal lymphoma is diffuse large B-cell lymphoma. We report a case of an 84-year old Caucasian female who was admitted to the hospital because of a 2 days history of altered mental status. In the emergency department the patient was found to have acute kidney injury and hypercalcemia. On physical examination a large lower quadrant abdominal mass was palpated. Computed tomography scan of abdomen confirmed the presence of a mass along the cecum and proximal ascending colon. Colonoscopy showed a large ulcerated mass and biopsy was consistent with diffuse large B-cell lymphoma. The patient underwent colectomy but refused to receive chemotherapy.
Introduction
The gastrointestinal (GI) system is a common site for secondary spread of non-Hodgkin lymphomas (NHL).1,2 However, primary involvement of the GI tract is significantly less common, representing only 10-15% of all NHLs and accounting for approximately 4% of all tumors arising in the GI system.3,4 Primary colorectal lymphomas are even rarer entities, comprising 0.1-0.5% of all colorectal malignancies and 1.4% of all cases of NHL. 5 Dawson et al. were the first to describe colorectal lymphoma in 1961. 6 Lack of specific symptoms can lead to delayed diagnosis in 35-65% of patients when surgical treatment options are either urgent or emergent.7–9 In more than half of the cases, it is clinically possible to appreciate the lymphoma as a bulky mass on a physical examination. 10 Treatment has a multidisciplinary approach with combination of surgery, chemotherapy and radiation. Due to its rarity, there is lack of randomized trials and most of the information published is based on individual case reports. Below, we present a case of 84 year old female with primary colorectal lymphoma who presented to the hospital with altered mental status secondary to hypercalcemia.
Case Report
An 84-year old Caucasian female was sent to the hospital because of a two day history of altered mental status. In the emergency department she was found to have acute kidney injury and hypercalcemia with a total serum calcium level of 17 mg/dL (normal range: 8.5-10.3). Physical examination was significant for a right lower quadrant mass measuring 10 cm at the greatest diameter. The rest of the physical examination was unremarkable. A hypercalcemia work up was initiated, which showed elevation of lactate dehydrogenase, uric acid, 1,25 vitamin D and decreased level of parathyroid hormone. The rest of the laboratory parameters were within normal limits.
Computed tomography (CT) scan of the abdomen and pelvis was performed, which showed a 12.0 cm circumferential mass along the cecum and proximal ascending colon (Figure 1). Subsequent colonoscopy demonstrated an ulcerated circumferential rigid mass at the ascending colon (Figure 2). A gross pathological specimen is shown in Figure 3. A few days later, the patient's pathology report revealed diffuse large B cell lymphoma (DLBCL) of the ascending colon. Microscopic examination of the biopsy sample revealed portions of colonic tissue which were infiltrated by the neoplasm. The neoplasm formed large sheets of cells without glandular formation or keratin production (Figures 4 and 5). The cells were monotonous with irregular nuclear membranes and prominent nucleoli with easily found mitotic activity. Immunohistochemical staining was also performed and revealed the tumor to be CD45+, CD3+, CD20+, BCL6+ and MUM1 negative (Figure 6). Lymphoid survey was negative and there was no distal organ involvement. Upon classification using the Revised International Prognostic Index (R-IPI), the patient was classified in the poor risk group with a score of 3. The patient refused to receive chemotherapy but did undergo open right hemi-colectomy with right oophorectomy and ilieocolic anastomosis. CT scan of the abdomen and pelvis was done two months later, which showed recurrent mass in the right lower quadrant for which patient underwent multiple sessions of radiation therapy. The course was complicated with radiation induced colitis and deep venous thrombosis requiring hospitalization. The patient did not receive any chemotherapy and did not undergo any additional surgical intervention.
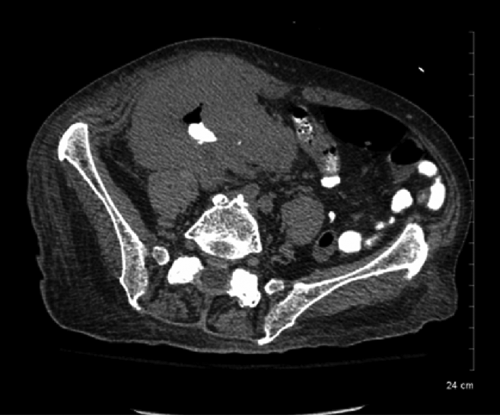
Large circumferential mass along the cecum and ascending colon measuring 12.7×7.7×12.1 cm in size with oral contrast within the lumen.

Colonoscopy-ulcerating ascending colon mass.

Surgical specimen from ascending colon showing bowel wall infiltration with tumor tissue.

Diffuse sheets of large atypical lymphoid cells with prominent nucleoli.
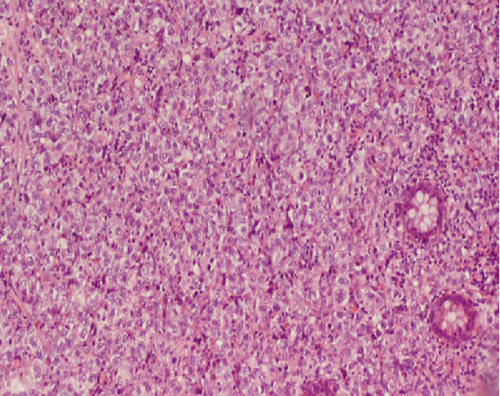
Effacement of normal colonic architecture by a diffuse infiltrate of lymphoid cells.
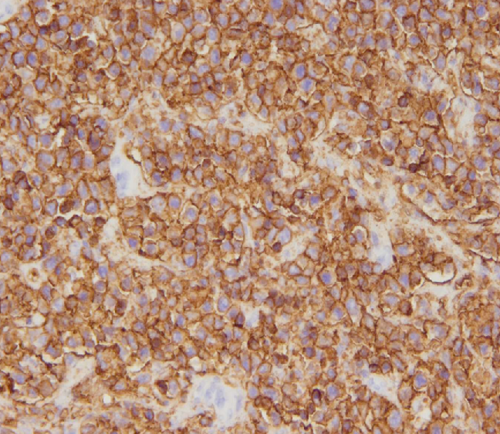
Immunohistochemistry: peroxidase staining shows the tumor cells to be positive for CD20, a pan B cell marker.
Discussion
Primary colorectal lymphoma is a rare malignancy accounting for 3% of all GI lymphomas and 0.1-0.5% of all colorectal malignancies.10,11 The stomach is the most common location of GI lymphomas (50-60%) followed by small bowel (20-30%) and colorectal (10-20%) lymphomas. 12 Cecum is the most common site of involvement for colorectal lymphomas, because of abundance of lymphatic tissue. 10 The definition of primary GI lymphomas varies among different authors. However, most classification systems refer to primary GI lymphomas as arising in any part of the GI tract, even in the presence of more disseminated disease as long as extra nodal site is predominant. 13 The most common histological subtype of colorectal lymphoma is diffuse large B-cell lymphoma. 9 Other histologies include follicular lymphoma, Burkitt lymphoma and Mantle cell lymphoma. 10
The etiology of DLBCL is unknown, but some risk factors and predisposing conditions have been identified such as immunodeficient conditions and inflammatory bowel diseases. 5 The most common symptoms are abdominal pain, weight loss and altered bowel habits. 14 Males are affected more common with the mean age of diagnosis at 55 years. 13 ,15–17 Colonoscopy with subsequent biopsy is the diagnostic modality of choice in the work up of colorectal lymphoma. CT scan or other imaging modalities can be helpful in suggesting the diagnosis and in describing tumor extension/staging, including determining extracolonic involvement.
For diagnostic purposes it is crucial to define morphology and immunophenotyping. Morphologically, DLBCL consists of large size atypical lymphoid cells with prominent nucleoli and basophilic cytoplasm that have a diffuse growth pattern obliterating colonic gland architecture (Figures 4 and 5). Immunohistochemistry and flow cytometry confirms the immunophenotype of DLBCL. Tumor cells generally express pan B cell markers such as CD20, CD19, CD 22, CD45 and CD79a (Figure 6). 18 Seventy percent of tumor cells may express BCL-6 protein; CD10 is expressed in 30 to 60% of cases and MUM1/IRF4 in present in 35 to 65% of cases. 19 CD10 expression is considered a marker of follicular derived DLBCL. Previous studies yielded contradictory results regarding the prognostic role of CD10 in DLBCL. Uherova et al. and Xu et al. showed that there is no difference between CD10+ and CD10-DLBCL in regard to IPI components (age, extranodal involvement, stage, LDH level, performance status) but CD10+ had negative impact on overall survival and treatment response.20,21 Fabiani et al. were unable to show any correlation between IPI parameters, survival and CD10 expression. 22 Most of the time DLBCL often is associated with genetic abnormalities in BCL-6 gene, which leads to an uncontrolled cell cycle.23,24
There are many prognostic systems of which the International Prognostic Index (IPI) is the main clinical tool used in the prognostication of DLBCL. 25 Gene Expression Profiling (GEP) is a new evolving approach to diagnose, classify and prognosticate DLBCL. 25 According to GEP two prognostically significant types of DLBCL have been identified. The molecular subgroups include germinal center B-cell-like (GCB) and activated B-cell-like (ABC), which are associated with different chromosomal aberrations. GCB group has better prognosis than the ACB group.26–28
In the literature the treatment of colorectal DLBCL includes chemotherapy, radiation, surgical treatment or a combination of these approaches. The CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) therapy has been the mainstay therapy for DLBCL for many years providing long term survival in 40-50% of patients. 29 Rituximab is the first monoclonal antibody approved for the treatment of DLBCL. 30 Randomized trials have shown that a combination of chemotherapy (CHOP) and rituximab results in significantly increased survival as compared with chemotherapy alone.31,32 It is important to note that addition of rituximab to CHOP regimen resulted in 10-15% increase in survival with no increased risk of side effects. 33 Furthermore, rituximab monotherapy in patients with relapsed or refractory DLBCL allows achieving complete or partial remission. 34 Revised IPI has been developed to better predict outcome in patients treated with R-CHOP (Table 1). 35 A few randomized trials investigated the role of radiation and came to the conclusion that radiation therapy is at least as effective as chemotherapy alone.36–41 Radiation therapy might not be the preferred option for the treatment of DLBCL involving the colon, because of a high risk of complications involving the small and large bowels according to Quayle et al. 41 Because of the low incidence of primary colorectal lymphoma, there are no randomized trials for surgical management. Most of the subjects in published cases underwent some sort of colon resection.
Revised international prognostic index (R-IPI).

Revised International Prognostic Index criteria: i) age >60; ii) serum lactate dehydrogenase concentration above normal; iii) Eastern Cooperative Oncology Group (ECOG, Zubrod, WHO) scale performance status ≥2; iv) Ann Arbor stage III or IV; v) number of extranodal disease sites >1.
One point is given for each of the above characteristics present in the patient, for a total score ranging from zero to five.
Conclusions
Primary colorectal lymphomas are rare malignancies. The most common histological subtype of colorectal lymphoma is diffuse large B-cell lymphoma. Due to the lack of randomized controlled trials, there is not a clear treatment algorithm for these cases. However, combination chemotherapy along with rituximab appears to be a promising treatment.