
Abstract
Primary gastric lymphoma (PGL) is the most common extranodal non-Hodgkin lymphoma and represents a wide spectrum of disease, ranging from indolent low-grade marginal zone lymphoma or mucosa-associated lymphoid tissue (MALT) lymphoma to aggressive diffuse large B-cell lymphoma. The PGL is a relatively rare cancer and easily misdiagnosed due to its unspecific symptoms of the digestive tract. The medical literature and ongoing clinical trials were reviewed on the clinical presentation, diagnosis, prognosis, prevention, and treatment of PGL. Primary gastric lymphoma is an event in the course of cancer with a variable clinical presentation and a wide differential diagnosis. Chronic gastritis secondary to Helicobacter pylori (H pylori) infection has been considered a major predisposing factor for MALT lymphoma. Magnetic resonance imaging and endoscopic ultrasonography have helped in staging of these cancers. The clinical course and prognosis of this disease are dependent on histopathological subtype and stage at the time of diagnosis. A global therapeutic approach to the cure of PGL has completely changed over the past 10 years, including innovative and conservative options to reduce treatment toxicity. Due to the rarity of PGL, many aspects of this neoplasm are still controversial. The incidence of this disease is increasing, making it necessary for clinicians to understand the clinical symptoms, workup, and treatment of these lymphomas.
Keywords
Introduction
The incidence of lymphoma has been on the rise over the past 2 to 3 decades. This increase has been observed in extranodal forms. 1,2 Extranodal forms refer principally to non-Hodgkin lymphoma (NHL) of the central nervous system (CNS), followed by gastric, intestinal, and cutaneous lymphomas. 3
The most common extranodal site of NHL is the stomach, representing between 30% and 40% of all extranodal lymphomas and 55% and 65% of all gastrointestinal lymphomas. 4 Primary gastric lymphoma (PGL) is a rare tumor, with an incidence of 4% to 20% of NHL and approximately 5% of primary gastric neoplasms. 5 The small intestine and ileocecal regions follow in frequency. 6
The PGL is more likely to occur in patients older than 50 years, but patients in the second decade of life could be also affected. 7,8 Males are 2 to 3 times more likely to develop PGL than females. 9,10 Histopathologically, almost 90% of the PGL are of B-cell lineage with very few T-cell lymphomas and Hodgkin lymphoma. 6
The marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT) type lymphoma occurs in 38% of the cases while diffuse large B-cell lymphoma (DLBCL) occurs in 59%. Other types occur rarely, such as mantel cell lymphoma, and are listed in Table 1.
Distribution of the Main Histological Types (Defined According to the Criteria in the REAL Classification) in the German Multicenter Perspective Study for Gastrointestinal NHL. (Koch et al, 2005) 11
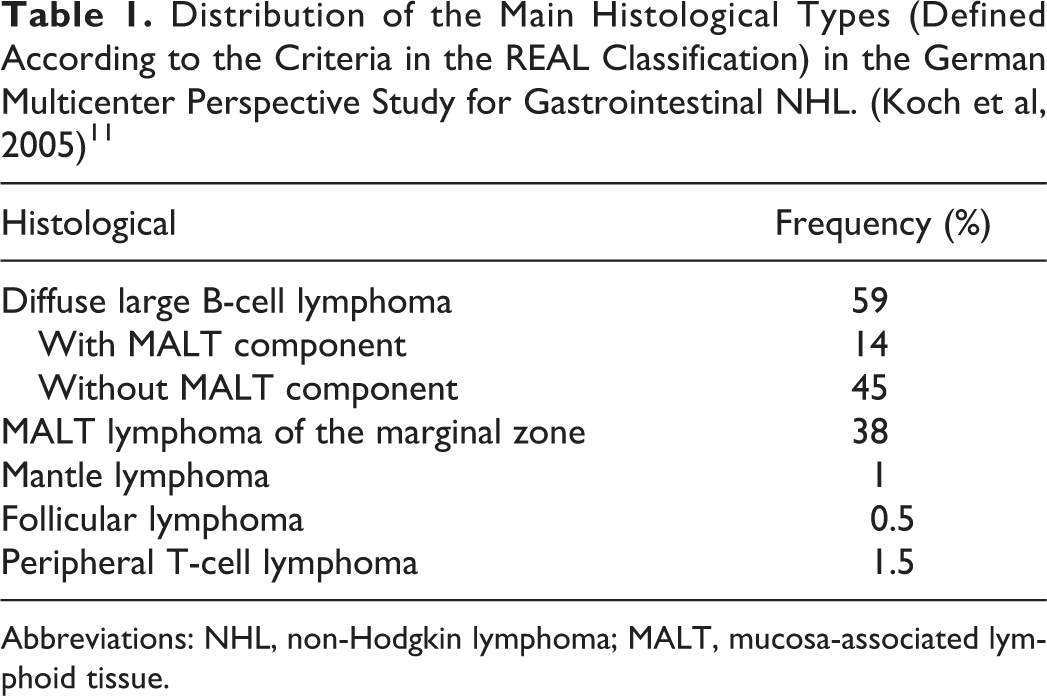
Abbreviations: NHL, non-Hodgkin lymphoma; MALT, mucosa-associated lymphoid tissue.
Many authors have described potential risk factors associated with the pathogenesis of PGL, including infection by Helicobacter pylori (H pylori), HIV, Epstein-Barr virus, hepatitis B virus, and human T-cell lymphotropic virus 1. Campylobacter jejuni (C jejuni) has also been described as an important organism implicated in the pathogenesis of MALT lymphoma, specifically of immunoproliferative small intestinal disease. 12 Other pathological conditions, such as celiac disease, inflammatory bowel disease, and immunosuppression, have also been associated with PGL. 13
In order to establish an accurate diagnosis and staging of this heterogeneous group of lymphomas, different procedures have been used, including endoscopic ultrasound (EUS), 14,15 endoscopic biopsies, computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (FDG-PET), 16 and/or molecular cancer markers.
Gastrectomy is limited to rare selected cases of PGL. There are many options in the treatment of PGL, including antibiotic therapy, H pylori eradication therapy, immunotherapy, chemotherapy, and radiation therapy. The overall prognosis of PGL is dependent on tumor characteristics and host-related factors, such as histological subtype, age, and performance status (PS). In this review, we aim to help clinicians better understand the pathology, diagnosis, and novel therapies in PGL and how these have evolved over the past 10 years.
Clinical Presentation
The initial symptoms of PGL are usually nonspecific, mimicking gastritis, peptic ulcer disease, pancreatic disorders, or functional disorder of the stomach. The physical examination is unremarkable in 55% to 60% of cases. 17 These nonspecific findings lead to a delay in diagnosis, which can be several years in certain cases. 18 The most common symptoms reported include weight loss, nausea, vomiting, abdominal fullness, and indigestion. 19 Weakness, night sweats, jaundice, fever, and dysphagia occur less frequently. Other uncommon symptoms are gastric obstruction and perforation, fever, hepatomegaly, splenomegaly, and lymphadenopathy. 20 About 20% to 30% of patients with gastric DLBCL report gastrointestinal bleeding in the form of hematemesis or melena. In some cases, physical examination findings including epigastric tenderness, adenopathy, and palpable epigastric masses can be found. 19
Diagnostic Studies
The examination of biopsy samples taken during an esophagogastroduodenoscopy (EGD) is the gold standard for diagnosis of PGL. 9 The EGD by itself cannot identify or discriminate gastric lymphoma from the more common gastric carcinomas. However, there are 3 main injury patterns that can be recognized during an endoscopic examination: ulceration, diffuse infiltration, and a polypoid mass. 21 Although these findings are not specific for PGL, EGD is an indispensable tool for the initial diagnosis and follow-up of cases as well as for obtaining multiple stomach biopsies specimens (specially antrum and corpus), duodenum, and at the gastroesophageal junction. The presence of H pylori in tissue samples obtained by EGD must also be tested in all cases through immunohistochemistry (IHC). Urease breath tests can be used as well, but serology is still the gold standard for diagnosing active H pylori infection. 22,23
Radiological procedures can be helpful to establish the diagnosis and determine the extent of PGL. Certain characteristics such as the thickness of the stomach wall, the presence of atypical ulcer deformities, obstruction, and mass effect are features suggestive but not specific for gastric lymphoma. Chest and abdomen CT scan should be done to exclude systemic disease, lymph node extension, and/or to evaluate for infiltration of the adjacent structures. Gastric wall thickening or mass lesion can be identified in 85% of cases by imaging, 5 while lymphadenopathy is reported in only 50% of them. 24
The MRI can also be used to evaluate PGL. Features on MRI associated with PGL diagnosis include irregularly thickened mucosal folds, irregular submucosal infiltration, annular constricting lesion, exophytic tumor growth, mesenteric masses, and mesenteric/retroperitoneal lymphadenopathy. 25
The EUS is an accurate technique in the evaluation of the extent and invasion of the lesion. The depth of lymphomatous infiltration and the presence of perigastric lymph nodes can be detected by EUS and are important for treatment planning. The problem of EUS is that in follow-up and restaging after treatment (chemotherapy or radiotherapy), EUS tends to overstage residual disease and cannot always differentiate between tumor infiltration and inflammatory response to therapy. 26
Due to the variable physiologic FDG activity in the stomach and its different degree of uptake in various histologic subtypes, 18F-FDG-PET/TC is not considered on its own an adequate diagnostic technique for PGL but can be used in patients with primary gastric DLBCL.
Histology and Pathogenesis
It has been observed that some histological lymphoma subtypes have a propensity to affect the gastrointestinal tract such as MALT lymphoma in the stomach; mantle cell lymphoma (MCL) in the terminal ileum, jejunum, and colon; enteropathy-associated T-cell lymphoma in jejunum; and follicular lymphoma (FL) in the duodenum. 27 However, the 2 predominant subtypes of PGL are MALT and DLBCL. 28
General Histological Characteristics
An implicated mechanism that explains the precise location of extranodal forms of lymphomas is the capacity of mature lymphocytes to recirculate between blood and lymph tissue. It has been shown that lymphocytes interact with endothelial venules, mediated by receptor molecules (lymphocytic and integrins). 23
B lymphocytes of the marginal zone are the origin of MALT lymphoma and are characterized by a cellular population that is heterogeneous with a predominant presence of small lymphocytes or monocytoid appearing lymphocytes and large cells (immunoblasts and centroblast). 29 The increase in the number of large cells in MALT lymphoma can create diagnostic challenges, suggesting a histological transformation into a DLBCL (characterized by the presence of compact aggregates or a large cell sheet-like proliferation). 30
High-grade PGL is practically always of the B-cell phenotype and are associated with an aggressive clinical presentation. An unsolved remaining question is whether all primary gastric DLBCL are derived from previous low-grade MALT lymphomas or if they appear de novo. Cytogenetics differentiate the 2 in some cases, and it is important to remember that gastric MALT lymphomas frequently have cytogenetic alterations that are different from those of typical primary DLBCL of the stomach.
There is nonspecific antigenic profile of MALT lymphomas that differentiate it from other marginal zone lymphomas. The MALT lymphomas are positive for surface immunoglobulins (Igs), for pan-B antigens (CD19, CD20, and CD79a), and for marginal zone typical antigens (CD35 and CD21). Meanwhile, DLBCL immunophenotype is different with CD45, CD5, and CD10 expression, which can be used as a prognostic indicator. 31 In some cases, detection of monoclonality in Ig heavy chain rearrangement of the lymphoproliferative disease by polymerase chain reaction (PCR) could be performed in biopsy samples. 32 However, heterogeneity in the performance and results obtained from IgH gene rearrangements has been reported (included H pylori-associated gastritis cases). The PCR for IgH gene rearrangement should be performed only when there is a lymphoid infiltrate morphologically suspicious of lymphoma, and MALT lymphoma should not be diagnosed in the absence of clear histological evidence. 33
Pathogenesis of MALT Gastric Lymphoma
Association with chronic H pylori
The literature has reported that approximately 75% of H pylori-positive gastric MALT lymphomas obtain complete remission after the eradication of these bacteria with antibiotic therapy, supporting the association between H pylori infection and the presence of MALT. 34,35 Lymphoid cells attract to gastric MALT tissue by a chronic H pylori infection. When these cells are continuously stimulated by H pylori, they can give rise to MALT lymphomas. In addition to B cells, T cells and macrophages play an important role in MALT lymphomagenesis. 36,37 Overtime, B-cell clones that still depend on antigens for growth and survival, bearing unknown mutations, will emerge. At this stage, the proliferation is monoclonal but not yet able to spread beyond the site of inflammation. With the acquisition of additional mutations, including chromosomal abnormalities, the tumor becomes antigen independent and capable of systemic spread.
In H pylori-negative gastric MALT lymphomas, the theory that infection leads to lymphomagenesis and the presence of lymphoma loses validity. Today, many feel there are various mechanisms by which pathogenesis occurs in H pylori-negative gastric MALT, including the relationship between genetic alterations (t(11;18)) and other activation pathways.
Genetic and molecular alterations
It has been postulated that MALT lymphoma arises from postgerminal center memory B cells with the capacity to differentiate into marginal zone cells and plasma cells. 38 Four recurrent chromosomal translocations have been found: t(11;18)(q21;q21), t(14;18)(q32;q21), t(1;14)(p22;q32), and t(3;14)(p13;q32).
In normal B and T cells, signals produced by the interaction of antigen with antigen receptors on the cell surface cause the protein B-cell leukemia/lymphoma 10 (Bcl-10) to bind to the MALT lymphoma-associated translocation protein 1 (MALT1). This triggers additional events that result in the activation of nuclear factor (NF)-κB, a transcription factor that promotes cell survival. 39 –41 Translocations t(11;18), t(14;18), and t(1;14) result in the activation of NF-κB through the Bcl-10/MALT1 signaling complex and in doing so enhance the survival of extranodal lymphoma cells. 42 Specifically, the t(11;18) fuses the apoptosis inhibitor 2 gene on chromosome 11 (called API2 or IAP2) with the MALT1 gene on chromosome 18. 43,44 The t(11;14)(q32;q21) fuses MALT1 with the IgH gene. The rare t(1;14)(p22;q32) fuses the coding sequence of Bcl-10 on chromosome 1 to the IgH promoter/enhancer elements. 45 These all result in overexpression of Bcl-10, which causes cellular transformation 46 and provides a survival advantage to the neoplastic B cells. Nuclear expression of Bcl-10 or NF-κB in gastric MALT, determined by IHC, is associated with resistance of gastric MALT to the antibiotic therapy, even in those tumors that lack the t(11;18). 47
The other translocation, t(3;14)(p13;q32), fuses the FOXP1 gene on chromosome 3 to the IgH gene and results in increased nuclear levels of the FOXP1 transcription factor. 48 Its function is not yet known, but tumors with FOXP1 translocation appear to transform to DLBCL more frequently, whereas those with t(11;18) do so rarely. 49
Pathogenesis of Gastric DLBCL
Gastric DLBCL is sometimes called high-grade gastric lymphoma. Compared to low-grade MALT lymphoma, high-grade gastric lymphoma is reported to be associated with a lower complete remission rate and shorter survival. It has remained unclear whether DLBCL arises de novo in the stomach or whether it transforms from low-grade MALT lymphomas. 50,51
Oncogene Bcl-6 (located on chromosome 3q27) is frequently present in the majority of extranodal high-grade lymphomas. An overexpression of this gene could explain the development of both gastric DLBCL and DLBCL developing in other sites. Bcl-6 promoter region could be altered due translocations, somatic hypermutations, or deregulating mutations. These genetic rearrangements cause an overexpression of the gene, which seems to predict a better prognosis. 52
High levels of Bcl-6 expression were detected in germinal center B-cell like (GCB) cases, independent of Bcl-6 genetic aberrations. In the rest of non-GCB lymphomas, mutations that produce Bcl-6 deregulating were correlated importantly with a high Bcl-6 expression level. However, no correlation was found between survival rates and the Bcl-6 expression level in the non-GCB cases.
On the contrary, Bcl-2 oncogene expression was reported to be significantly low in gastric than in primary extranodal high-grade B-cell lymphomas, while nuclear p53 protein expression did not differ importantly between these 2 groups. 53 In large cell gastric lymphomas, there have been no significant differences in either Bcl-2 or p53 expression profiles, independent of the evidence of an MALT component. However, in cases of large B-cell lymphomas with a low-grade MALT component, it has been reported an important downregulation of Bcl-2 and upregulation of p53 protein of uncertain clinical significance. 44
Immunohistochemistry
The novel information of the molecular heterogeneity of B-cell lymphomas, especially DLBCL, is shifting the paradigm toward more personalized evaluation and therapies. The term “double-hit” lymphomas is when c-Myc and Bcl-2 and/or Bcl-6 rearrangement is identified by cytogenetic testing or by fluorescence in situ hybridization (FISH). Other definition such as “double-protein” or “double expressor” refer to the coexpression of 2 oncogenes (MYC and Bcl-2) on a high percentage of tumor cells based on IHC staining. 54,55 Double expressor and double-hit lymphomas have prognostic implications in DLBCL, but their use in primary gastric B-cell lymphomas remains unclear. There is information in the literature about the combination of abnormalities of Myc and Bcl-2 or Bcl6 in PGL. 56 He et al have recently reported a study with 188 tissue samples of gastric lymphoma tested with FISH and IHC using a panel of biomarkers, such as c-Myc, Bcl-2, Bcl-6, CD31, CD10, Mum-1, and Ki-67. Results have shown that “double-hit” lymphomas are a rare subtype among PGL, while patients with multiple gene amplification and/or copy gains of c-Myc, Bcl-2, and Bcl-6, and “double-protein” gastric B-cell lymphomas had a poor clinical outcome. 57 In addition, patients negative for expression of c-Myc, Bcl-2, and Bcl-6 in tumor tissue but high expression of secreted protein, acid, and rich in cysteine in stromal cells may have a better prognosis than other gastric B-cell lymphomas regardless of their clinical stage and pathological types. 58 As further molecular research is conducted, a better understanding of diagnostic and prognostic markers will help provide more personalized treatment decisions in PGL.
Staging
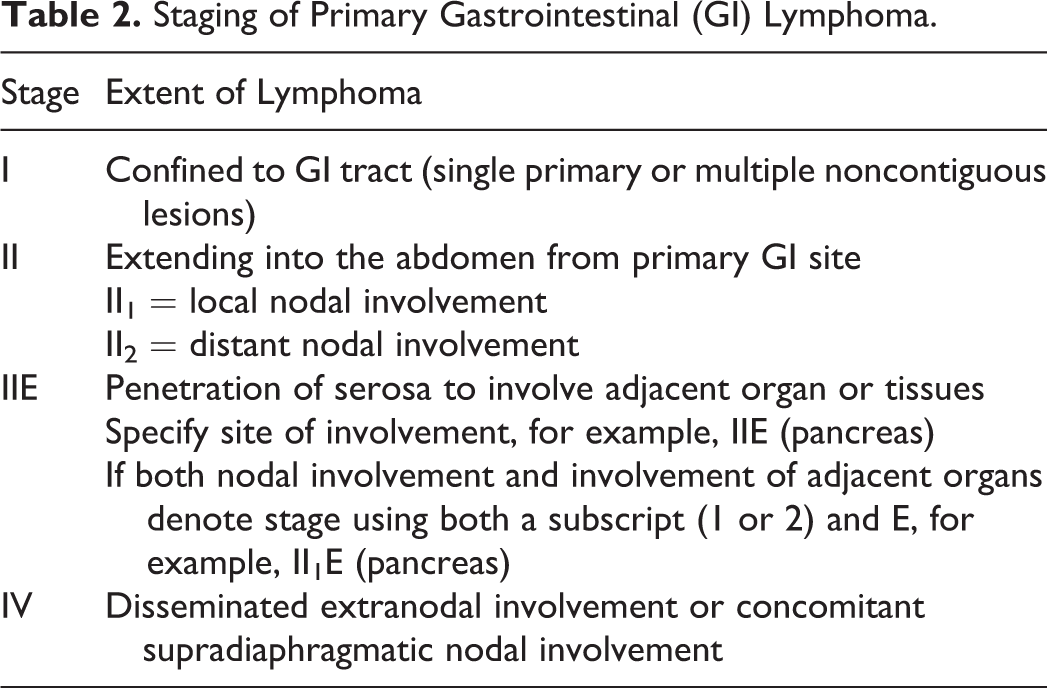
Once the diagnosis of PGL is established, the staging is essential for planning treatment and prognosis. It is also important to exclude systemic lymphoma with secondary involvement of the stomach. A few years ago, staging for gastric lymphoma was controversial with various staging system in use. After an international workgroup that was centered on staging in lymphoma, a modified Lugano staging has now been accepted as the standard in patients with PGL 59 (Table 2).
Staging of Primary Gastrointestinal (GI) Lymphoma.
The staging includes endoscopy with step biopsy in order to identify microscopic infiltration of nearby structures, including the duodenum. Total body CT scan permits assessment of nodal involvement above and below the diaphragm and extension of the tumor outside the stomach. The EUS is superior to CT scan in the detection of false-negative cases and may be employed for accurate estimation of both the depth and invasion and involvement of regional lymph nodes. Bone marrow examination helps determine the presence or absence of tumor spread. Indirect laryngoscopy is also helpful for excluding Waldeyer ring involvement, which is reported to be associated with gastric lymphoma. 4
The usefulness of a fusion PET/CT scan has been documented only for DLBCL, independent of the affected anatomic site; but a role of PET/CT is controversial in MALT lymphomas, which are frequently reported as PET negative due to their indolent behavior. Currently, for PGL, PET CT is a standard initial imaging study in DLBCL histology but not recommended in cases of MALT PGL.
In cases with DLBCL, accurate staging is necessary for the important therapeutic implications. If the disease affects beyond the stomach and regional nodes, treatment strategies can no longer be focused on local control; been systemic aggressive chemotherapy the mandatory option.
Regardless of histology, the general evaluation also involves the lactate dehydrogenase (LDH) and β-2 microglobulin serum levels, being their high levels related to bad prognosis. Routine lumbar puncture with cerebrospinal fluid analysis is mostly unnecessary unless the patient has risk factors for CNS involvement (clinical symptoms, more than 2 extranodal areas of involvement, the presence of c-Myc rearrangement, and so on). 23
Prognostic Factors
Several risk factors have been studied that may contribute to survival in patients with PGL. In previous studies, female gender, low-grade histology, good PS, and surgical resection have been reported to be associated with good overall survival. The international prognosis index (IPI) developed for DLBCL (age >60 years, advanced stage, poor PS, and elevated LDH) is commonly used and is predictive of survival in PGL. Although these clinical factors have been identified, many patients with PGL still have varying prognoses, and other factors may also contribute to prognostication in these patients. More studies are needed to further define prognostic factors in PGL.
Histological Features
In MALT lymphomas, the number of circulating large transformed B cells without overt DLBCL as a prognostic factor remains unclear. Literature reported that MALT lymphomas in the stomach with more than 1% 58 or more than 5% 60 of diffuse large blasts, but no overt DLBCL, showed a worse outcome after radiotherapy independently if the patient received chemotherapy and/or responded less often to H pylori eradication therapy.
Cytogenetic Markers
The findings of t(11;18) is directly related to resistance to antibiotic therapy. Researchers screened for the AP12/MLT fusion transcript as a direct marker for this translocation, in 10 antibiotic responsive and 12 antibiotic nonresponsive patients with gastric MALT lymphomas. The transcript was observed in 9 of 12 patients nonresponsive to antibiotic treatment but was not detected in antibiotic responsive patients. Therefore, most H pylori-associated gastric MALT lymphoma that do not respond to antibiotic therapy are associated with the t(11;18) translocation. Starostik et al showed that patients with the t(11;18) transcript usually do not transform to high-grade DLBCL as well, indicating a more indolent disease course. 61
Endoscopic Ultrasound
The EUS has been used to determine the eradication of H pylori and the outcome of MALT lymphoma treatment. Thus, patients with disease limited to the mucosa and/or submucosa will show complete remission rates of up to 100%, whereas lower remission rates will be reported in patients with a more extensive infiltration.
A New MALT Lymphoma Prognostic Index (MALT-IPI)
In September 2017, Thieblemont et al have published the results of a new prognostic index for MALT diagnosed patients. The 3 individual features maintaining the greatest prognostic significance were age >70 years, Ann Arbor stage III or IV, and an elevated LDH. This index identified 3 groups: low, intermediate, and high risk (according to the presence of 0, 1, or >2 of these factors, respectively). The 5-year event-free survival (EFS) rates in the low-, intermediate-, and high-risk groups were 70%, 56%, and 29%, respectively. The prognostic utility was retained in both gastric and nongastric lymphomas and was confirmed in the validation set, being an important tool to identify patients with MALT lymphoma at risk of poor outcomes. 62
Treatment
The strategies of treatment for gastric lymphomas are controversial, and the optimal frontline treatment regimen varies. However, treatment options depend on the histologic subtype and stage of the disease. Although there are many options in treatment approach, the majority of physicians usually follow the guidelines of DLBCL and MALT lymphoma [European Society of Medical Oncology (ESMO) or National Comprehensive Cancer Network (NCCN) guidelines] in their treatment decisions.
Treatment of Early-Stage, H pylori-Positive, Gastric MALT-Type Lymphoma
The gastric MALT-type lymphomas have an “indolent” clinical–biological behavior pattern, with a tendency to stay localized at the onset site in 70% to 80% of cases. 12 Until now, the most widely accepted initial treatment option for localized disease is the eradication of H pylori using the triple therapy based on the combination of proton-pomp inhibitors (PPI), clarithromycin with either amoxicillin or metronidazole for 10 to 14 days. 63 Similarly, levofloxacin has been used in patients whose initial triple therapy had failed. In this case, triple therapy would include levofloxacin, amoxicillin, and a PPI for 14 days. 64 Local epidemiology of the infection and the possible resistance to certain antibiotics are important information to take into account to choose the appropriate treatment regimen.
Several studies have confirmed the effectiveness of antibiotic therapy with long-term remissions in 70% to 100% of patients with localized, H pylori-positive, MALT lymphomas. However, failure in H pylori eradication is not uncommon (20%-30%), although some tumors exhibit a slow response to therapy. The time necessary to reach a complete remission varied from 3 months to more than a year. 36,65 The MALT tumors have an indolent nature, which allows physicians to continue watchful waiting before determining next treatment.
There is no evidence to justify additional treatment with chemotherapy in patients who respond to antibiotic therapy. However, evaluation of residual lymphomatous gastric infiltration with posttherapy biopsies can be difficult to interpret, and there are no a uniform criteria to define histological remission.
In order to confirm the effective H pylori eradication, the method accepted is the urea breath test. To assess MALT lymphoma remission, a first endoscopy is performed 3 to 6 months after completion of antibacterial treatment, which also allows for checking of the H pylori status histologically. Culture and susceptibility testing are particularly recommended to guide further treatment in the case of a resistant strain indicated by a persistent positive urea breath test.
The absence of standardized and easily reproducible criteria makes it difficult to compare results presented in various clinical series. For this reason, a posttreatment histological evaluation system was proposed in 2012 by the Groupe d’ Etude des Lymphomes de l’ Adulte (Table 3). In general, after antibiotics therapy, the presence of residual disease without H pylori reinfection appears to be a self-limiting phenomenon that is not necessarily associated with a tumor clinical progression.
GELA Histological Grading System for Posttreatment Evaluation of Gastric MALT Lymphoma.a

Abbreviations: GELA, Groupe d’Etude des Lymphomes de l’Adulte; MALT, mucosa-associated lymphoid tissue; MM, muscularis mucosa; LP, lamina propria; SM, submucosa; LEL, lymphoepithelial lesions.
a Reproduced from Gut, Copie-Bergman C, Gaulard P, Lavergne-Slove A, Brousse N, Fléjou JF, Dordonne K, de Mascarel A, Wotherspoon AC, 52:1656, ©2003 with permission from BMJ Publishing Group Ltd.
Treatment of Patients With H pylori-Negative Gastric MALT-Type Lymphoma
Almost 10% of MALT lymphomas are unrelated to H pylori infection, and the pathogenesis remains unclear. 66 One hypothesis is the relationship between genetic alterations (t(11;18)) and the NF-κB activation. The second one is related to an infectious cause different than H pylori, for example, infections associated with C jejuni.
Although no clear therapeutic guidelines have been established for those patients in whom antibiotic therapy results are unsuccessful or for those without the presence of H pylori at diagnosis, several studies have reported that a percentage of patient responded to antibiotic therapy. Raderer et al reported that 5 of 6 patients with H pylori-negative gastric MALT lymphoma responded to antibiotic therapy, indicating an excellent response rate of 83%. The authors also observed that most of the patients responded to antibiotic therapy between 3 and 9 months. 67 Predictive factors for patients who may not respond include multiple lesions, lesions in both proximal and distal parts of the stomach, and the presence of t(11;18). 68
The reason why antibiotic therapy is effective in H pylori-negative gastric MALT lymphomas cases is not clear, but some theories exist. One theory is that these patients were infected with bacteria other than H pylori, and the antibiotic therapy was able to eradicate these bacteria. Another explanation is that clarithromycin changes the patient’s immune system through its immunomodulatory effect. 69 Nonetheless, further studies are needed to shine some light on the mechanisms underlying why antibiotics may be helpful in H pylori gastric MALT lymphomas.
Prior to antibiotic therapy, radiotherapy was the first-line therapy for gastric MALT lymphomas. Therefore, “involved-field” irradiation (total dose of 30 Gy administered over 4 weeks) has continued to be the preferred treatment for patients with stage I and stage II MALT lymphomas without H pylori or with persistent lymphomas following antibiotic therapy. 6 A total of 97.8% of patients who were resistant to antibiotic therapy responded to radiotherapy. 70 The most common side effects of radiotherapy included anorexia, nausea, and vomiting. With a dose of 30 to 35 Gy, no delayed toxicity (such as gastric ulcers or gastrointestinal hemorrhaging) has been noted, although long-term effects of radiotherapy on the functionality and integrity of the gastric mucous membrane remain ulcear. 71
In cases of gastric lymphomas, surgery has been used historically as the initial treatment as well. However, recent data have shown that conservative therapy allows for a better quality of life, with no negative impact on survival rates. Surgery, thus, is not indicated as an initial therapy except in rare cases refractory to nonsurgical approaches and in patients presenting with severe complications, such as gastric perforation, hemorrhage, or obstruction. 17
The use of chemotherapy and immunotherapy has been reported in gastric MALT lymphoma of all stages; however, there is no evidence to indicate the most effective regimen. Patients with localized disease, who did not respond to antibiotic therapy or radiation therapy, should be considered for systemic chemotherapy.
The efficacy of various chemotherapy agents has also been reported either as monotherapy or in combinations with anti-CD20 monoclonal antibodies.
Rituximab: The use of rituximab (R) has been reported effectiveness in MALT-types and marginal zone lymphoma treatment, reaching response rates of approximately 70%.
71
Monotherapy based in R has proven activity in MALT lymphoma without important side effects in patients not eligible for high-intensity treatment.
72
The standard doses of R used in the majority of clinical trials were of 4 weekly doses of 375 mg/m2. In association with bendamustine, purine analogs, and/or alkylators, this monoclonal antibody remains an important anticancer agent in treating patients with newly diagnosed or relapsing MALT lymphoma.
Alkylating agents: Chlorambucil is probably the most studied agent in MALT lymphoma, either in monotherapy or in combination. The use of chlorambucil combined with R is active as first-line therapy for patients with disseminated MALT lymphoma or with limited-stage MALT lymphoma relapsing after local treatment or antibiotics. This combination could be an advisably treatment option for elderly patients, both with gastric or extragastric presentation, and is effective irrespective of t(11;18) status.
73
Bendamustine: R–bendamustine seems to be highly effective and well tolerated. All the results have showed that extragastric MALT lymphoma probably needs 6 treatment cycles to obtain the best outcomes.
74
Purine analogs: Cladribine and fludarabine are active drugs used in both gastric and extragastric MALT lymphomas treatment.
75
Combined with R, they are a highly active option for patients with newly diagnosed and relapsed MALT lymphoma. Due to hematological toxicity, these agents should be considering as an option for young patients, in first-line treatment. In the past years, these drugs have been gradually replaced by bendamustine. Anthracyclines: Its use might be considering in fit patients with a high tumor burden or disease with active symptoms, in which side effects might be acceptable. Should not applied as first-line treatment in most patients with MALT lymphoma who are usually asymptomatic and do not require intensive therapy.
Proteasome inhibitors: Both MALT lymphoma and multiple myeloma are characterized for the potential to produce monoclonal Igs.
76
Bortezomib remains an experimental drug in the management of this pathology. The secondary effects as polyneuropathy and hematological toxicity, limit its use in routine practice. It’s necessary for new data of different schedules and lower doses combinations.
Immunomodulators: Preliminary results have shown that lenalidomide alone or with R is active in MALT lymphoma. These results suggest that lenalidomide deserves further investigations in larger trials.
77
There is limited evidence related to the use of thalidomide.
78
The above medications are all options of treatment in patients who require treatment. However, there is no current consensus for one regimen over another for patients who did not respond to antibiotic therapy because the disease is indolent by nature, and a “watch-and-wait” strategy may be appropriate for some patients without any symptoms.
Zucca et al published in 2013 the only randomized study [International Extranodal Lymphoma Study Group 19 (IELSG 19)] designed to compare chlorambucil alone and in combination with R. In this trial, the combination of the 2 drugs resulted in improved remission quality measured by complete remission rate and translated into significantly prolonged EFS. 79 The study protocol was enhanced to add a third arm of treatment with R in monotherapy. In 2017, the 3-arm study results showed superior efficacy of the combined therapy (R and chlorambucil) in treatment of MALT lymphoma. Good results obtained in terms of EFS and progression-free survival with little added toxicity justifying the first-line use of this regimen and may define a standard regimen for treatment of patients with MALT lymphoma who are in need of systemic therapy. The lack of overall survival benefit, however, leaves open the possibility to consider the use of chlorambucil in monotherapy when treatment cost is a relevant argument and also provides evidence for the use of single-agent R to avoid the side effects and chemotherapy toxicity. 80
Treatment of High-Grade Gastric Lymphomas
The DLBCL represents the most common histological type of gastric lymphoma, 16 sometimes called high-grade gastric lymphoma. Before current multimodality therapy was established, high-grade lymphoma was recognized as a negative prognostic factor for survival, associated with lower complete remission rate and a shorter survival rate. 81 However, recent studies showed no survival differences between MALT lymphoma and DLBCL, likely because of improved treatment modalities. 16
The treatment of PGL has shifted away from surgery and toward chemotherapy regimens. Today, surgery is now limited to cases of perforation, hemorrhage, or obstruction due to the tumor, and it is no longer the cornerstone of treatment with its mortality rate reaching up to 8%. 5,82 As shown in Table 4, chemotherapy has surpassed surgery in terms of benefits and complications.
Surgery Versus Chemotherapy Complications in the Treatment of Primary Gastric Lymphoma.

The treatment of DLBCL-PGL consists of anthracycline-based chemoimmunotherapy. Clinical studies performed on nodal DLBCL offers scientific support for these regimens showing significant improvement in overall survival rates. 83 The most commonly used chemotherapeutic regimen for DLBCL of the stomach is a combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) and R-CHOP.
Coiffier and colleagues published results of a multiinstitutional randomized trial of 400 patients with nodal DLBCL, with high rates of complete response and overall survival for patients with R-CHOP compared to CHOP alone. Based on its reported therapeutic benefit in patients with nodal DLBCL, R-CHOP has been traditionally used as the frontline treatment in patients with localized gastric DLBCL. 84
Frontline chemoimmunotherapy with 3 to 4 cycles of standard R-CHOP followed by “involved-field” radiotherapy could be considered as a gold standard option for localized stages (stages I and II in the Lugano classification). 23 Advanced-stage patients (Ann Arbor stage III/IV) usually undergo 6 to 8 cycles of R-CHOP in order to obtain a complete remission rate similar to their nodal counterparts. 23 Recent studies have reported the benefits of consolidation radiation therapy after chemotherapy in nodal DLBCL 85,86 ; however, its role in PGL is controversial.
Various recent studies have exhibited possible regression (analogous to MALT lymphomas) in localized DLBCL following anti-H pylori therapy. 87 This suggests that a subset of aggressive gastric lymphoma might still contain an antigenic drive, though antibiotics could be paired with chemotherapy at the clinician’s discretion. In 2012, Ferreri et al reported the use of H pylori-directed therapy in DLBCL-PGL. Sixteen patients were enrolled and treated with antibiotics including clarithromycin, tinidazole or metronidazole, and omeprazole. H pylori eradication and tumor response were assessed at 30 and 60 days after antibiotics. All patients achieved H pylori eradication and just 1 patient required a second-line antibiotic therapy. Complete response after eradication was achieved in 8 (50%) patients, and partial remission in 3 patients. These results demonstrate that eradication, keeping chemoradiotherapy for unresponsive patients, is a fair strategy for patients with limited-stage gastric DLBCL. 88 These results need to be valid in larger prospective studies prior to broad usage.
The current recommendation is to treat with R-CHOP every 14 to 21 days for 6 to 8 cycles. Alternatively, in patients with localized PGL or those unable to complete full 6 cycles of R-CHOP, R-CHOP × 4 cycles followed by involved field radiation therapy (IFRT). There may be a role of interim PET scan in regard of decision to pursue radiation therapy, although this continues to be debated. 89 The PET CT should be done at the end of therapy, and if the patient has progressive disease, the consideration for second-line treatment (salvage chemotherapy) for DLBCL with a regimen, such as rituximab, ifosfamide, carboplatin, and etoposide or Gemcitabine, dexamethasone, and cisplatin and rituximab, followed by autologous stem cell transplantation should be considered. 90,91
Follow-Up
Regular follow-up after any treatment is needed, since diagnostic gastric biopsies cannot exclude the presence of a concomitant, aggressive DLBCL, which would require proactive therapy with curative intent. In many centers, a breath test is performed at approximately 2 months posttreatment to record successful H pylori eradication. Also, 3 to 6 months after H pylori eradication, an endoscopic examination with multiple biopsies should be done to assess lymphoma regression. Endoscopic examination should be repeated every 6 months for 2 years and then yearly to monitor histological remission. 23
For aggressive histologies, regular clinical evaluation, repeated blood counts, and hematochemistry are expected. In the end of treatment, PET CTs are used to determine a complete remission, and based on new recommendations, there are no indications for surveillance CT scans or PET CTs unless patients have new symptoms. 92,93
Future Strategies
A better understanding of the etiology and molecular aspect of PGL has provided potential new treatment strategies. Identification of cell surface antigens has led to the introduction of monoclonal antibodies such as R and radioimmunotherapy, which have led to a more targeted approach with an important effect for the overall management of lymphoma. The development of anti-CD20 second- and third-generation antibodies (ofatumumab, veltuzumab, ocrelizumab, and obinutuzumab) shows that other targeted may be useful in PGL as well in the future. Agents targeting the Bcl-2 (venetoclax), the BTK pathway (ibrutinib), and the PI3K pathway (idelalisib) are now deemed as a more biologically focused management and continue to be studied in lymphomas, including PGL.
Chimeric antigen receptor (CAR) is a genetically engineered receptor that combines a scFv domain, which specifically recognizes the tumor-specific antigen, with T-cell activation domains. CAR T-cell therapies have demonstrated tremendous efficacy against a variety of B-cell malignancies in many clinical trials (DLBCL, MCL, CLL, and FL) and could be an option for PGLs. Recent US Food and Drug Administration approval for refractory DLBCL based on the results of the ZUMA-1 study shows that CAR T-cell therapy will be used in refractory DLBCL in the future. 94,95 Clinical trials with CAR therapy are ongoing in indolent lymphomas (including marginal zone lymphoma) at this time.
Conclusions
The rarity of PGL has left many aspects of this neoplasm to remain unknown. The majority of PGL are MALT type, which can be related to H pylori infection or DLBCL. In general, MALT lymphomas are treated with antibiotic therapy to eradicate H pylori or a watch-and-wait approach that is implemented for asymptomatic cases. When another therapy is needed, it is usually R monotherapy or R-based combination therapy. Radiation therapy may also be used but may lead to more toxicity but is associated with better response rates. In cases of DLBCL, systemic chemotherapy with R-CHOP or R-CHOP like is indicated. The future will lead to more targeted therapies in PGL and also a better understanding of its pathophysiology.
Footnotes
Authors’ Note
No significant relationships exist between the authors and the companies/organizations whose products or services may be referenced in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.