
Abstract
Deciduoid mesothelioma is a rare variant of the epithelioid histotype spectrum, resembling decidua of gravid uterus. It is found in the peritoneum of young women, but also in the pleura of elderly people. Histotype plasticity from epithelioid to sarcomatoid mesothelioma may be considered as epithelial-mesenchymal transition (EMT). A full autopsy was performed and mesothelioma infiltrates were analysed by immunohistochemistry. The metastasis of an epithelioid pleural mesothelioma to a hyperplastic polyp of the stomach is presented in this autopsy case. Deciduoid morphology increased during tumour progression and metastasis. The increase in eosinophilic cytoplasm correlated with the upregulation of the intermediate filament vimentin. High expression of vimentin was found in both central and superficial periglandular regions of the polyp. High vimentin expression also can occur in epithelioid rather than sarcomatoid differentiation. Thus, although vimentin is considered to be the major EMT marker, additional pathways must regulate its expression.
Introduction
Malignant mesothelioma (MM) is composed by the 2 major histotypes epithelioid and sarcomatoid; the biphasic being a mixture of both. In more detail, several subtypes or differentiation patterns are recognized, particularly for the epithelioid histotype. The most frequent epithelioid patterns are tubulo-papillary, adenomatoid (microglandular) and sheet-like, the less common ones include deciduoid, small cell or clear cell. The pleomorphic and lympho-histiocytoid subtypes are rare. Deciduoid mesothelioma is composed of tumour cells with abundant glassy eosinophilic cytoplasm, resembling decidua cells of the gravid uterus. 1 This differentiation variant is more commonly found in the peritoneum of young women but has also been reported in the pleura of elderly people.2–8 It should not be misdiagnosed as peritoneal deciduosis or florid mesothelial hyperplasia. 9 Pleural deciduoid mesothelioma is associated with asbestos exposure. The prognosis depends on the number of chromosomal losses.10–12
Mesothelial cells are derived from coelomic epithelium via mesenchymal-epithelial transition (MET), explaining the co-expression of cytokeratin and vimentin.13,14 This co-expression pattern is retained in the malignant mesothelioma. Importantly, the trans-differentiation from epithelioid to sarcomatoid histo-type may be considered as epithelial-mesenchymal transition, reflecting the histotype plasticity of this neoplasm. 15 During this reverse process in comparison to MET, the expression of cytokeratins, calretinin and podoplanin (D2-40) is often reduced, whereas vimentin expression remains mostly stable or is increased.
We here present a case of malignant pleural mesothelioma that metastasises to a hyperplastic polyp of the stomach. During the metastatic process, the deciduoid morphology and therefore the epithelioid aspect increased. Interestingly, this happened in parallel to a concomitant increase of the mesenchymal marker vimentin, favouring a regulation independent of morphologic EMT.
Materials and Methods
The patient was a 75-year-old man with a smoking history of 20 pack-years and probable occupational asbestos exposure as a precision mechanic. An epithelioid pleural mesothelioma of the left pleural cavity was initially diagnosed by video-assisted thoracoscopy. Other diseases included adipositas associated with type II diabetes and hypercholesterolemia as well as prominent arteriosclerosis with ischemic cardiomyopathy. He received platinum-based chemotherapy and local radiotherapy. Tumour progression was detected 40 months later with local relapse including infiltration of the left diaphragm and mediastinum as well as widespread mesenteric and retroperitoneal lymph node metastases. Further chemotherapy together with corticosteroids was administered. He died 51 months post diagnosis after a short hospitalisation for severe tachy-dyspnea and abdominal ileus with meteorism.
A complete autopsy was performed 8 hours after death. Tissue samples were immediately fixed in buffered formalin and subsequently cut to 4 micrometer sections after paraffin-embedding. Immunohistochemistry was performed using the avidin-biotin/peroxidase complex method and respective antibodies against vimentin, pan-cytokeratin, carcinoembryonic antigen (CEA), epithelial membrane antigen, calretinin and Ber-EP4. For electron microscopy formalin-fixed tissue was trimmed and refixed in glutaraldehyde. Thereafter it was post-fixed in 1% osmium tetroxide, dehydrated and embedded in araldite. Thin sections were counterstained with uranyl acetate and lead citrate and observed under a transmission electron microscope. Mineralogical tissue analysis was performed by energy-dispersive x-ray microanalysis.
Results
Macroscopy
At autopsy a widespread local tumour spread was found in the left pleural cavity with infiltration of the lung parenchyma and the left diaphragm with direct extension to the peritoneum, the retroperitoneum and the right diaphragm. Further there was metastasis to the right lung and pleural cavity, the heart and the pericardial sac, the liver, the pancreas and bones. Lymph node metastases included the cervico-thoracic nodes associated with facial oedema and thrombosis of the left brachiocephalic vein, abdominal nodes associated with thrombosis of the upper mesenteric and the splenic vein as well as retroperitoneal nodes associated with bilateral ureter compression. Remarkably, we found a metastasis in a pedunculated stomach polyp of 4 cm head diameter, situated at the major fundic curvature. The polyp showed a glistening and lobulated surface and on cross section a peripheral microcystic aspect and a firm core.
Microscopy
On the initial thoracoscopic biopsy, an epithelioid malignant pleural mesothelioma with infiltration of fatty tissue was diagnosed (Figure 1). No particular deciduoid morphology was noted. Immunohistochemically, tumour cells were strongly positive for pan-cytokeratin, calretinin and EMA but only weakly and focally for vimentin. Ber-EP4 and CEA were negative. However, at autopsy, several whole sections of the primary tumour in the pleura showed partial deciduoid differentiation with an increased amount of eosinophilic cytoplasm. This phenomenon was even more pronounced in the metastasis of the stomach polyp. The stomach polyp was of the hyperplastic type, consisting mostly of dilated foveolae and pyloric type glands with abundant mucous secretion, neutral on the surface and more acidic towards the inner glandular dilatations. In the central part, few glands of fundic type were discernible. There was no intestinal metaplasia or dysplasia. The mesothelioma infiltrates were predominantly found in the centre of the polyp (Figure 1), extending from there into the more superficial regions. Immunologic anti-tumour response was sparse, with few lymphocytic elements in the polyp stroma. The deciduoid morphology was recognizable in central as well as peripheral parts of the polyp, but showed varying immunohistochemical marker profiles in these two compartments: The peripheral mesothelioma cells surrounding epithelial gland structures showed focal expression of pan-cytokeratin and calretinin, whereas the central part completely lacked these markers (Figure 2). Vimentin expression was much stronger in the polyp compared to the pleura, but with equal distribution in the superficial and central compartment. Other metastases also displayed deciduoid morphology but to a lesser degree.
Epithelioid mesothelioma at diagnosis in pleura, at autopsy in pleura and at autopsy in stomach polyp. Note increasing deciduoid morphology. Hematoxylin and eosin stains, magnification 200×. Lower left: whole view of polyp stained by Periodic Acid Schiff (PAS). Note central pale areas, representing mesothelioma infiltrates.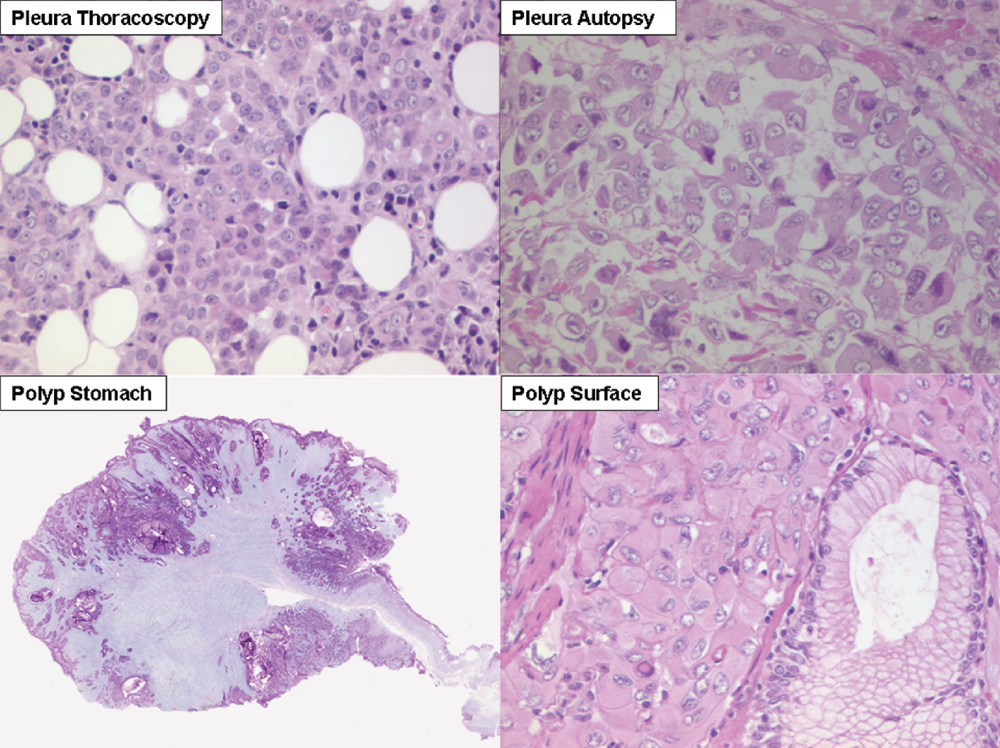
Immunohistochemistry with vimentin, pan-cytokeratin and calretinin on pleura and stomach polyp. Lower left: Pan-cytokeratin of periglandular polyp surface. Insert Pan-cytokeratin of polyp centre. Lower right: Calretinin of periglandular polyp surface. Insert: Electron microscopy of central tumour moiety. IHC magnifications 100× to 400×.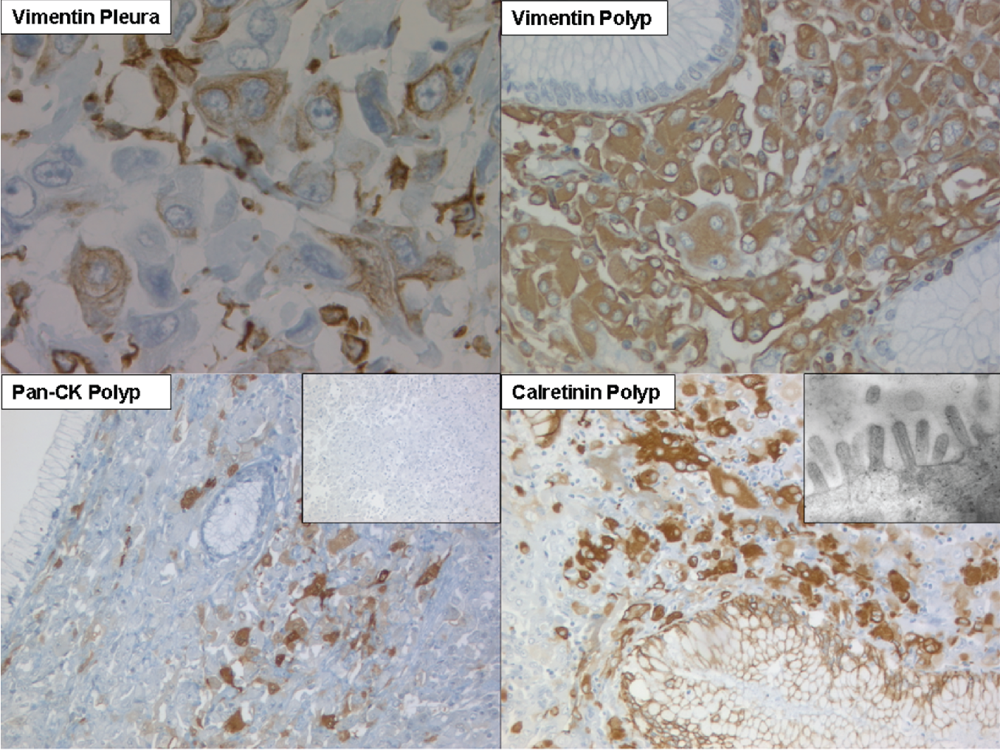
Electron microscopy and mineralogy
Electron microscopy revealed that the polyp centre was not necrotic, since the diagnostic long slender and bushy microvilli were observed in central mesothelioma infiltrates (Figure 2). Prussian-blue stained lung parenchyma sections did not reveal any ferruginous bodies. When analysing enriched lung dust, 7 ferruginous bodies per gram wet weight were found. Element analysis showed few mineral fibres, in particular titanoxide (rutil) and the amphibol asbestos crocidolite and anthophyllite. In addition, several different mineral dusts were observed.
Discussion
Deciduoid mesothelioma is a rare subtype of epithelioid mesothelioma. Tumour cells are described as having a large ovoid or polygonal eosinophilic cytoplasm, large atypical nuclei and obvious nucleoli. They abundantly produce glycogen and hyaluronic acid as well as cytokines such as interleukin-6 (IL-6) or granulocyte colony-stimulating factor (G-CSF). 16 Numerous cytosolic intermediate filaments, either dispersed or bundled, appear to be the ultrastructural basis for the deciduoid morphology. 5 We demonstrate in this study, that the amount of this particular cytoplasm can increase during tumour progression and metastasis. It is more commonly associated with an increased expression of vimentin rather than cytokeratins, since deciduoid differentiation was also found in the tumour infiltrates of the stomach polyp centre, where immunohistochemical loss of pan-cytokeratin was noted. Hyperplastic polyps are associated with various forms of chronic gastritis, particularly autoimmune and H. pylori gastritis, but have also been reported to arise after acute gastric ulceration.17,18 In general, they are viewed as regenerative lesions following mucosal injury. 19 Thus we consider two main possibilities for the development of a mesothelioma metastasis in a hyperplastic stomach polyp: i) tumour cells invade a pre-existing polyp due to chemo-attractant factors; ii) after an extensive nodal spread, a gastric wall metastasis develops, ulcerates and is followed by polyp formation. We consider the latter mechanism more likely, due to absent gastroenterological pathology in the surrounding gastric mucosa, the atypical size and location (>2 cm fundus) and the extensive tumour spread. Inflammatory reaction in the polyp was minimal, so it seems that the tumour has terminally overrun the immune system.
Hyperplastic polyps are thought to contain a highly active, oedematous and inflamed stroma and a peak proliferative activity of the epithelium in the middle compartment between the basal and superficial mucosa. This creates a local microenvironment with cytokine or paracrine factor gradients from the surface epithelium to the core of the polyp. Such gradients are potentially able to define the degree of epithelial-mesenchymal transition of an invading tumour; e.g. in non-small cell lung cancer, we have found the EMT marker protein periostin to be up-regulated in tumour cells and stroma areas immediately bordering the invasion front and the basement membrane, respectively. 20 In this case, the epithelioid marker calretinin as well as pancytokeratin were accentuated around the superficial fundic glands. Thus one may assume that if mesothelioma cells reach the polyp periphery, they enter into a more epithelial primed environment. However, the mesenchymal marker vimentin was equally distributed throughout the whole polyp metastasis and showed an increased expression level in comparison to the pleural primary. Interestingly, this went in parallel with increased deciduoid morphology.
Therefore, we conclude that, although vimentin is considered to be the major EMT marker, other factors must regulate its expression next to EMT signalling. Vimentin can very well be associated with rather epithelial or epithelioid than sarcomatoid differentiation. This constellation has been observed in several other malignancies such as renal cell, thyroid and endometrial carcinoma.
Footnotes
Acknowledgements
This case report is dedicated to Dr. William MacGee.