
Abstract
The association between pathologic complete response (pCR) following to neoadjuvant chemotherapy (NAC) and the improved survival in breast cancer has been previously reported. The aim of this study was is to explore the expression of several biomarkers described during epithelial-mesenchymal transition (EMT) and the achievement of pCR in different molecular subtypes of breast cancer. We identified archived pathology tissue from patients with breast cancer who received NAC during the year 2014. We performed immunohistochemical analysis of vimentin, nuclear factor κB (NF-κB), epidermal growth factor receptor (EGFR), E-cadherin, estrogen receptor (ER), progesterone receptor, and Her2neu and studied the association between the expression of these markers and pCR. A Fisher exact test for categorical cofactors, an unpaired t test and a nonparametric Wilcoxon test for continuous cofactors were used. The results showed a significant expression of vimentin in triple-negative breast cancer (TNBC; P = .023). An inverse correlation between vimentin and the ER expression (P = .032) was observed. No significant association was noted for vimentin, NF-κB, EGFR, and E-cadherin was associated with pCR. This study suggests that the evaluated EMT related biomarkers are not associated with pCR after NAC chemotherapy in an unselected breast cancer population. Vimentin and NF-κB expressions were associated with TNBC and could be further explored as potential therapeutic targets in this subgroup. A prevalence of vimentin and NF-κB among Hispanic patients with breast cancer warrants further investigation as a possibly contributing to the prevalence of TNBC and adverse prognosis in this population.
Keywords
Introduction
Despite major advances in breast cancer research and treatment, breast cancer still accounts for more than 40 000 annual cancer-related deaths in the United States. 1 Moreover, in Hispanic women, breast cancer is the leading cause of cancer-related death. Hispanic patients tend to present with larger tumors, more advanced stages which lead to higher mortality rates than in non-Hispanic white (NHW) women 2 and are well represented in this study.
Breast cancer is a heterogeneous disease with different phenotypes, described per the histologic and molecular characteristic. Invasive ductal carcinoma and invasive lobular carcinoma (ILC) are the 2 main histologic subtypes of breast cancer. The main difference between these 2 histologic subtypes is the lack of membranous E-cadherin protein expression in around 90% of ILC. 3 Two of the main molecular classes of breast cancer are the luminal type and the triple-negative breast cancer (TNBC). The luminal type comprises around 70% of invasive tumors and shows positive estrogen receptor (ER) expression. The TNBC type comprises 15% of cases and shows negative ER, negative progesterone receptor (PR), negative HER2 (human epidermal growth factor receptor 2). 4 This molecular taxonomy has important clinical value. Some of the molecular phenotypes (especially HER2 and TNBC) show unfavorable prognosis and/or resistance to chemotherapy. In addition, TNBC shows a special preference for distant metastasis to characteristic tissues (lung and brain). 5 It may also suggest different mechanisms of invasion and metastasis for breast tumors. The ethnic heterogeneities related to tumor subtypes may contribute to the fact that the incidence, progression, presentation, and response to therapy are variable among different ethnic groups. 6
Recent advances in breast cancer treatment protocols lead to increasing the rates of breast-conserving therapy (BCT) and decreasing the need for complete axillary lymph node dissection. Neoadjuvant chemotherapy (NAC) has become an established treatment modality for operable breast cancer. One of the advantages of NAC is providing active systemic treatment while downstaging the cancer at presentation. Neoadjuvant chemotherapy often allows patients initially considered for mastectomy only, to be able to receive breast-conserving surgery (BCT). 7 Ethnic differences in the use, response, and outcome of NAC in operable patients with breast cancer have been noticed. Particularly, Hispanic patients with breast cancer receive more frequently NAC than NHWs, although no significant differences in tumor response including pathologic complete response (pCR) were noticed.8,9 Our group has previously reported that Hispanic American patients with breast cancer have poor risk profile than NHW. 10 However, there is a paucity of data regarding clinical response and outcome following NAC in this group, hence the focus on this study population.
The short-term target after NAC is to achieve a pCR, 11 defined strictly as the absence of invasive cancer in the breast and axillary nodes, irrespective of ductal carcinoma in situ. Achieving pCR depends on many factors including the size of the tumor, the number of chemotherapy cycles received, the hormonal status, and possibly other biomarkers. The epithelial-mesenchymal transition (EMT) of tumor cells has been suggested to be predictive of tumor response following NAC. 12
Epithelial-mesenchymal transition is defined as the loss of epithelial characteristics and acquiring a mesenchymal phenotype. Epithelial-mesenchymal transition can be associated with increased aggressiveness and invasive and metastatic potential in cancer cells. During the process of EMT, cells undergo phenotypic changes and molecular alterations representing mesenchymal differentiation. 13 This leads to cancer cells losing epithelial markers, such as E-cadherin, α-catenin, and γ-catenin, and gaining mesenchymal markers, such as fibronectin, vimentin, and N-cadherin. These changes allow the epithelial cancer cells to gain more invasiveness and metastatic capabilities. It has been reported that EMT could also play a role in drug resistance. 14 Thus, we proposed to study the potential role of EMT markers associated with NAC and tumor subtype in a group of understudied Hispanic Mexican patients with breast cancer. We designed this study to investigate the immunohistochemical (IHC) expression of several EMT-related markers including vimentin, EGFR, NF-κB, and E-cadherin.
Materials and Methods
Case selection
After obtaining Institutional Review Board’s approval of the Texas Tech University Health Sciences Center (IRB#E14049), eligible cases were identified from the Breast Care Center database over a 12 months’ period in 2014. All patients who had available histologically confirmed invasive carcinoma tissue and who received neoadjuvant therapy in the center were included and their stored tissue retrieved for prospective analysis. Data about demographics, tumor characteristics (tumor location, size, grade, TNM stage), and treatment were obtained from the patient’s medical charts and breast cancer database. We identified 32 cases who fulfilled the eligibility criteria for the study. The paraffin-embedded invasive breast cancer tissue blocks were obtained. The following markers were prospectively conducted on the pretreatment biopsy tissues using IHC stains: vimentin, epidermal growth factor receptor (EGFR), NF-κB, and E-cadherin as markers for EMT. 15
IHC staining and scoring
The histopathologic slides were microscopically reviewed in each case. The most representative tumor block was selected for the study. From the selected blocks, 4-μm-thick tumor tissue sections on a positively charged slide were subjected to IHC staining for biomarkers: vimentin, E-cadherin, NF-κB, and EGFR. All IHC reactions were performed on an automated Ventana BenchMark ULTRA immune-stainer, using an UltraView Universal diaminobenzidine detection kit (Ventana Medical Systems, Inc., Tucson, AZ, USA). 16 The staining protocol is based on the UltraView Horseradish Peroxidase Universal Multimer reaction. The protocol involving heat antigen retrieval for paraffin-embedded sections was used per the manufacturer’s instructions. Primary antibodies (Cell Marque, a Sigma-Aldrich company, Rocklin, CA, USA) were applied. All used antibodies were prediluted and were ready to use. The anti–E-cadherin rabbit monoclonal antibody (0.314 µg/mL), anti-vimentin rabbit monoclonal antibody (1 µg/mL), anti–NF-κB, and anti-EGFR rabbit monoclonal antibody (0.4 µg/mL) were used. Negative control was done using tissue sections that went through the whole process of IHC but without any primary antibody. Positive controls are shown in Table 1. The reaction was enhanced by UV copper, and the slides were counterstained by hematoxylin. The IHC expression was assessed for each antibody separately. Semiquantitative methods by 2 blinded pathologists (O.P. and S.E.) using transmission light microscopy were performed. The localization of the stain (see Figures 1 to 4) is defined as cytoplasmic/membranous for vimentin, nuclear for NF-κB (regardless of cytoplasmic staining), and membranous for EGFR and loss of membranous expression of E-cadherin. 4 The immunoreactivity for all markers except E-cadherin was scored depending on both the percentage of positive tumor cells and the staining intensity. The percentage was considered 0 if no stain was detected, 1 if <10%), 2 if 11%-50%, and 3 if >50%. The staining intensity was scored as 0 (no stain), 1 (weak staining), 2 (staining in between weak and strong), and 3 (strong staining). The final score was achieved by multiplying the 2 scores. Only the cases with a final score of 0 were considered negative otherwise were considered positive. For E-cadherin, scoring the percentage of complete loss of membranous stain in the tumor cells was scored as 0 if no loss, 1 if <10%, 2 if 11%-50%, and 3 if >50%. This scoring was based on searching the literature. 4
The primary antibodies, their clone, and positive control.

Abbreviation: EGFR, epidermal growth factor receptor.

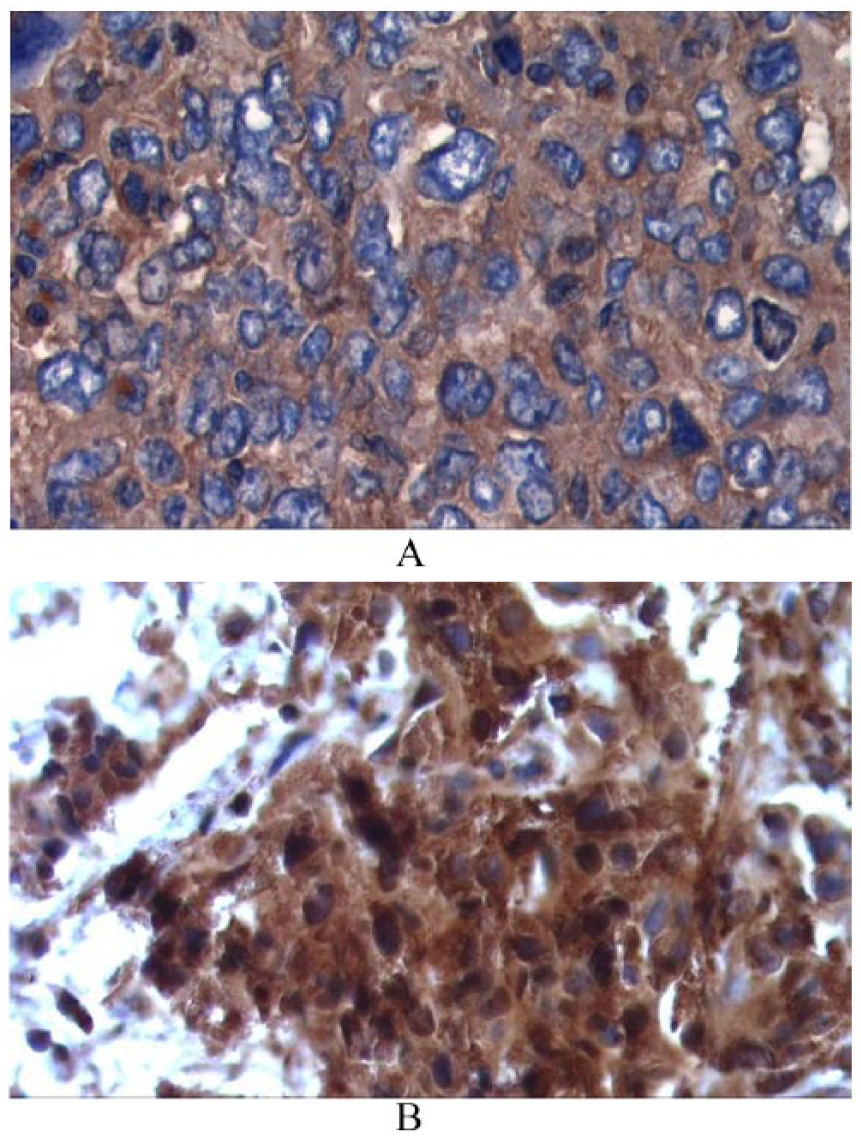
(A) Loss of membranous expression of E-cadherin in this field, which is scored as 3+. (B) Membranous staining of E-cadherin without loss of membranous expression, which is scored as 0.

(A) No membranous staining for EGFR and (B) some membranous EGFR staining. EGFR indicates epidermal growth factor receptor.
(A) Negative nuclear staining for NF-κB, regardless of cytoplasmic staining. (B) Nuclear staining of NF-κB. NF-κB indicates nuclear factor κB.

(A) Negative vimentin staining for tumor cells with positive staining of stromal cells (internal control). (B) Positive cytoplasmic staining for vimentin in tumor cells.
Hormonal status previously done on the biopsies was reassessed, and the cases were divided into 3 general groups: (ER or PR positive) and (Her2neu negative); (ER or PR positive), (Her2neu positive); and triple negative (ER negative, PR negative, Her2neu negative). The Nottingham histologic grade was used for grading and the TNM system was used for staging. The pCR was defined as absence of invasive tumor in both breast and lymph nodes.
Statistical Analysis
Categorical variables were summarized using frequency and percentages, whereas quantitative variables were summarized using mean and standard deviation (SD). The proportion of pCR along with 95% confidence interval (CI) was estimated for the entire cohort and by tumor subtypes. The ER, PR, and Her2 were combined into 3 specific groups: (ER or PR positive) and (Her2 negative), (ER or PR positive) and (Her2 positive), and (ER and PR negative) and (Her2 negative) (triple negative). Unpaired t tests were conducted to assess the differences in quantitative variables according to pCR. The Fisher exact tests were used to assess the association between categorical variables and pCR. An unadjusted logistic regression was conducted to determine effect size in association with pCR. P values were considered significant at the 5% level of significance. All analyses were conducted using a SAS V.9.4.
Results
A total of 32 patients who have received NAC at our institute were found to be eligible for statistical analysis in the study. A total of 27 patients had available postoperative tissue. The IHC expression of vimentin, EGFR, NF-κB, and E-cadherin was performed on pretreatment biopsies and when available on posttreatment ones as well. The mean age was 57.28 (SD: 13.92) years. Nine patients were stage II (28.13%), whereas 23 patients were stage III (71.88%). In all, 12 cases (37.5%) had (ER or PR positive) and (Her2 negative), 3 cases (9.38%) were (ER or PR positive) and (Her2 positive), and 11 (34.38%) were triple negative. In our study cohort, the most common EMT marker was E-cadherin positive (27, 84.4%) followed by vimentin (16, 50%) and NF-κB or EGFR (3, 9.4%).
The pCR was achieved in 13 (40.63%, 95% CI: 0.236-0.593). Of 13 achieved pCR, 5 pCR were obtained in the TNBC tumors, 3 pCR were in the ER+ only, 4 pCR were in the HER2+ only, and 1 had all positives (ER, PR and HER2+). The pCR was higher in TNBC (5, 45.45%) followed by hormonal receptor positive (ER or PR positive: 8, 38.1%). None of the markers (vimentin, E-cadherin loss, NF-κB, or EGFR) at baseline showed significant association with the achievement of pCR. Among patients with TNBC, most of the pCR had NF-κB positive, EGFR negative.
Table 2 shows distribution and comparison of pCR according to clinical and tumor characteristics. Specifically, we looked at the total final scores for vimentin, NF-κB, EGFR, and E-cadherin. No significant differences were found. A borderline significant association between PR and pCR (P = .076), with an unadjusted odds ratio of 0.111 (P = .061). Table 3 shows the association of the preselected biomarkers with tumor subtypes defined using a combination of ER, PR, and HER2 receptor. Vimentin was significantly associated with (ER and PR negative) and (Her2 negative) (P = .023). Table 4 shows the association of ER, PR, and HER2 with the same preselected biomarkers. Vimentin appeared to be significantly associated with ER-negative receptor (P = .032). The localization of the stain (Figures 1 to 4) is defined as cytoplasmic/membranous for vimentin, nuclear for NF-κB (regardless of cytoplasmic staining), and membranous for EGFR and loss of membranous expression of E-cadherin. 4
Distribution and comparison of pathologic complete response according to clinical and tumor characteristics.
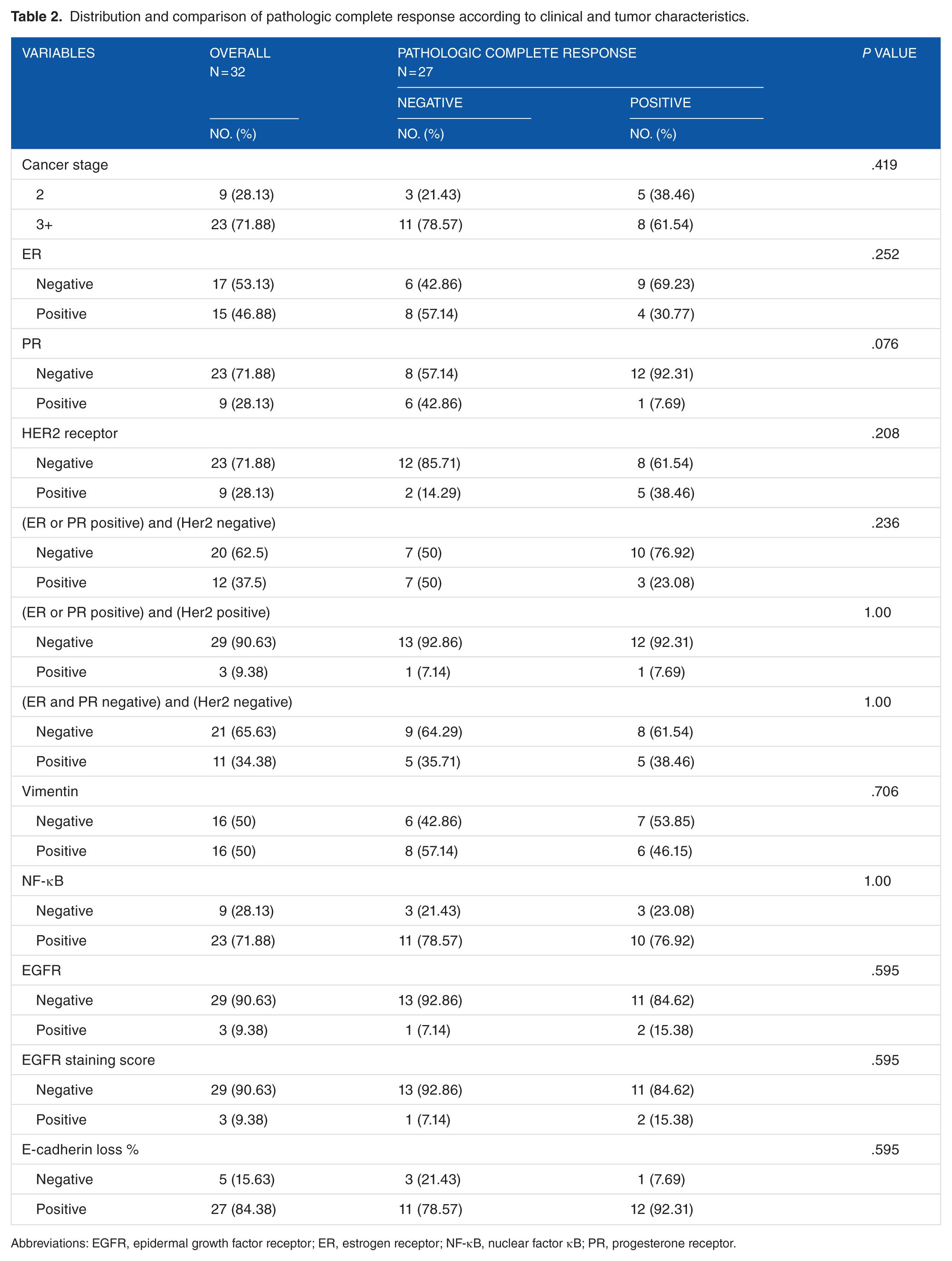
Abbreviations: EGFR, epidermal growth factor receptor; ER, estrogen receptor; NF-κB, nuclear factor κB; PR, progesterone receptor.
Association of preselected biomarkers with molecular subtypes.

Abbreviations: EGFR, epidermal growth factor receptor; ER, estrogen receptor; NF-κB, nuclear factor κB; PR, progesterone receptor.
Association of preselected biomarkers with ER, PR, and HER2 receptors.

Abbreviations: EGFR, epidermal growth factor receptor; ER, estrogen receptor; NF-κB, nuclear factor κB; PR, progesterone receptor.
Discussion
We examined the expression of IHC markers vimentin, EGFR, NF-κB, and E-cadherin in Hispanic breast cancer cases. We studied their relation to the achievement of pCR after NAC. Our study showed that vimentin is associated with TNBC. Most of the triple-negative tumors had positive vimentin and NF-κB expressions.
Vimentin is an intermediate filament protein normally expressed in cells of mesenchymal origin.17,18 However, it can also be expressed in epithelial cells if they are undergoing EMT either under physiological or pathologic conditions. Vimentin is a major component of the cytoskeleton. It regulates cell migration and controls recycling of endocytosed cell adhesion receptors as integrins to the plasma membrane. 19 In vitro studies showed that many aggressive breast cancer cell lines express vimentin, especially the basal-like breast cancer cells that may represent the clinical “triple-negative” (ER, PR, and HER2 negative) tumor type. 20 The positive correlation between vimentin expression and tumor aggressiveness is documented in several studies.6,21-23 However, other studies did not confirm this association. 24 Several studies attributed the correlation between vimentin expression and tumor aggressiveness to the lack of steroid receptors. 25 This observation was supported in our study. Vimentin is considered a canonical marker for EMT which plays a role in tumor invasive and progression. 26 Also, EMT is correlated with augmented surplus of cancer stem–like cells in neoplastic tissues which might contribute to cancer drug resistance.
The EMT has been reported to be more frequently expressed in TNBC compared with other subtypes, linked to early recurrence, metastasis, and poor outcomes in breast cancer.23,27 The EMT appears to be associated with poor survival rate in patients after taxane and anthracycline chemotherapeutic treatment. 28 Despite these findings, vimentin did not show correlation with pCR in our study. This agrees with Margeli et al 29 but could be attributed to a small number of participants. We believe that vimentin is a worthwhile biomarker to pursue in future research. There are recent experimental therapies which could target vimentin, providing a potential additional treatment options for this subset of patients with breast cancer. Some of these treatments under development are gene-regulating vimentin and EMT markers including the use of MicroRNA-138 found to be underexpressed in breast cancer with high expression of vimentin and other EMT markers. 30 Other studies proposed that treatment with phenethyl isothiocyanate is associated with the suppression of vimentin protein expression in cancer cells. 31
Among the most notable cancer molecular targets identified to date are the members of the EGFR/ErbB family belonging to a family of cell surface receptors called receptor tyrosine kinases. 32 In vitro studies have showed that the activation of EGFR promotes scattering and invasion of breast epithelial cells in 3-dimensional culture, which is associated with loss of cell polarization and other features of epithelial differentiation. 33 The EGFR overexpression in breast cancer is associated with large tumor size, poor differentiation, and poor prognosis. 34 The EGFR overexpression is observed in all subtypes of breast cancer but is frequently overexpressed in TNBC and inflammatory breast cancer, which are especially aggressive.35,36 This might be explained by the observation that the expression of EGFR is inversely related to ER status. We were not able to show that in our study due to the fact that only 3 cases had positive expression of EGFR in the tumor. A recent study by Peciak et al 37 analyzed not only the occurrence but also the level of EGFR VIII, which is an activated truncated variant of the EGFR expression in glioblastomas, prostate, breast, and colorectal tumors. All of the 43 analyzed breast cancer samples were EGFR negative. 38 In vitro analysis of epithelial ovarian cancer cell lines revealed that ligand-stimulated EGFR activated NF-κB–dependent transcription and induced secretion pro-inflammatory cytokines. 39 The role of EGFR as a predictive marker or therapeutic target in breast cancer is unclear.
Nuclear factor κB is a transcription factor acting as a central regulator in response to pathogens. The NF-κB can promote tumorigenesis via the regulation of target gene expression. The NF-κB translocates into the nucleus where it acts as a dimeric transcription factor that regulates the expression of genes influencing a broad range of biological processes including innate and adaptive immunity, inflammation, stress responses, B-cell development, and lymphoid organogenesis. 38 Tumor microenvironment, which consists of infiltrated immune cells and their secretary cytokines and/or chemokines, facilitates cancer cell motility, invasiveness, and metastatic potential.40,41 Drugs that target NF-κB have shown promising clinical outcomes. Thus, better understanding of the mechanism by which it mediates cancer cell invasion, migration, and metastasis could provide novel target therapy opportunities.
E-cadherin is a member of the cadherin superfamily encoded by CDH1 gene located on chromosome 16q22.1. 42 It is a cell adhesion and tumor suppressor protein that blocks the uncontrolled proliferation and cellular differentiation toward malignant phenotype. 43 Thus, complete or partial loss of E-cadherin expression is involved in tumor invasion and metastasis process. 44 Retrospective studies suggested that E-cadherin is a novel prognostic factor for TNBC. Previous studies showed that the loss of E-cadherin expression is a predictor for poor outcomes in terms of overall survival and disease-free survival. 45 Also, previous studies concluded that the combination of E-cadherin and Ki67 status might be a useful prognostic marker indicating the need for adjuvant chemotherapy in patients with stage II TNBC. 46
Our study has several limitations which should be considered while interpreting the study findings. The small sample size was the major limitation and restricted our analysis for adjusting the potential confounders and produced low power to detect some potential associations between EMT markers and pCR or tumor subtypes. This study did not collect follow-up data for recurrence and mortality outcome to evaluate the prognostic role of the considered markers in the study. We studied mainly Hispanic population which limits the generalizability of the findings to other ethnic groups. Despite these limitations, our study has several strengths. To our knowledge, this is the first study which provides an analysis of EMT-related markers in a Hispanic breast cancer population. The preliminary associations conducted in this study display some interesting observations including that patients who had pCR were more likely to be E-cadherin positive. The patients with TNBC were significantly more likely to have vimentin positive and NF-κB. These results possibly indicate a substantial prevalence of vimentin and NF-κB among Hispanic patients who are known to have increased prevalence of TNBC. The presence of these markers might be contributing to aggressive TNBC leading to worse prognosis in this population. These findings warrant further investigation on a large sample size using a cohort study.
Conclusions
This study adds to the body of knowledge about the biology of breast cancer specifically in Hispanic American patients and suggests that vimentin and NF-κB could be useful markers to evaluate and further explore as potential therapeutic targets in TNBC with overexpression of these markers. This study did not suggest that the evaluated EMT markers can be predictive for pCR in an unselected breast cancer population. Larger studies are needed to confirm the prognostic and predictive nature of vimentin and other EMT markers and to identify potential targeted treatments focusing on the EMT pathway.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Cancer Prevention and Research Institute of Texas (CPRIT) RP120528.
Author Contributions
ZN and SE contributed to the concept, design, data collection and manuscript writing. OP and SE performed the pathological analysis. All other authors contributed to data collection and analysis.