
Abstract
Human adipose-derived stem cells (hADSCs) are a promising source of autologous stem cells for personalized cell-based therapies. Culture expansion of ADSCs provides an attractive opportunity for liver cirrhosis patients. However, safety and stability issues can pose big challenges for personalized autologous stem cell products. In the present study, we addressed whether the commercial production program could provide a consistent product for liver cirrhosis therapy. We collected adipose tissue from three human donors by lipoaspirate and isolated ADSCs, which were expanded in culture to reach 1 × 10 8 cells (an approximately 1,000-fold expansion) within four passages. We then examined their morphology, chromosome stability, surface markers, and differentiation ability after culture. Next, we explored their therapeutic potential using a rat model of thioacetamide-induced liver cirrhosis. Culture-expanded ADSCs were injected intrahepatically, and their biodistribution was tracked by immunohistochemistry using an antibody against human mitochondria. Finally, we tested for tumor development by subcutaneously injecting a 100-fold dose range of cultured ADSCs into immunocompromised mice. Taken together, we find that culture expansion of autologous ADSCs is a potentially suitable stem cell product for personalized cell-based therapy for patients with liver cirrhosis.
Introduction
Liver cirrhosis occurs as a result of various chronic liver injuries, which may be caused by viral infection, alcohol abuse, or administration of drugs or chemicals 1 . Liver cirrhosis is characterized by accumulation of excess collagens and other extracellular matrix (ECM) proteins, which may lead to severe hepatic dysfunction. It causes significant morbidity and mortality2,3. Liver transplantation is the most effective method for treating end-stage cirrhosis, but its application is limited owing to a lack of donors as well as immune rejection 4 . Currently, the most effective treatment for liver cirrhosis is stem cell therapy5–8.
Adipose-derived stem cells (ADSCs) are similar to bone marrow-derived mesenchymal stem cells (BM-MSCs) but are much more abundant and easier to harvest. The yield from 1 g of adipose tissue is approximately 5,000 to 20,000 stem cells, whereas the yield from 1 ml of BM-MSCs is only 2% to 20% of ADSCs, which makes ADSCs a promising alternative cell source for treating liver diseases 9 . ADSCs have the ability to self-renew and differentiate into various cell types, including osteogenic, adipogenic, neurogenic, myogenic, chondrogenic, and hepatic lineages10,11. Moreover, ADSCs can fuse with endogenous hepatocytes and have a paracrine proliferative effect on hepatocytes12–16. Previously, we showed that transplanted ADSCs differentiate into albumin- and α-fetoprotein-secreting liver-like cells 1 week after transplantation 7 . These results suggest that ADSC transplantation may facilitate recovery from chronic liver damage 7 . Despite these advantages, obtaining a sufficient quantity of ADSCs for autologous transplantation is problematic. According to a report by Lin et al. 17 , the yield of ADSCs from 1 g of fat is approximately 5,000 cells. Therefore, for one average dose (i.e., 1 × 108), 20 kg of fat tissue would be needed to produce a single dose of ADSCs without culture. To address this problem, we developed a protocol for ADSC isolation and expansion.
Before culture-expanded stem cells can be used for clinical trials, they should be evaluated with regard to (i) the isolation, identification, and expansion process and (ii) the validation phase, including all quality controls for cell characterization, function, potency, and safety. In addition, good tissue practice (GTP) guidelines should be used to (i) define the distinct biological characteristics of the cells; (ii) verify their stability throughout the storage, thawing, and shipping processes; and (iii) ensure the quality assurance and control of the components. To apply culture-expanded ADSCs to human stem cell therapy, we thus examined their morphology, ability to differentiate, molecular expression profile, and stability in culture, as well as their biodistribution, toxicity, and tumorigenicity after transplantation in rats and mice.
Materials and Methods
Isolation and Culture of Human ADSCs
Adipose tissue (2–5 g) was harvested from the subcutaneous fat of the abdominal wall by lipoaspiration during abdominal surgery from healthy donors. All donors gave written informed consent. Human fat tissue (2–5 g) was placed in Ca2+/Mg2+-free phosphate-buffered saline (PBS) and immediately transferred to the laboratory. Human adipose tissue was removed from the transport medium, placed in a Petri dish, and cut into small pieces (1–2 mm3) in the presence of Ca2+/Mg2+-free PBS. The tissues were dissociated with 0.1% collagenase I (Gibco, Carlsbad, CA, USA) and incubated for 60 min at 37°C. After enzymatic digestion, the resultant cells were collected and cultured in keratinocyte serum-free media (SFM; Gibco) supplemented with 10% fetal bovine serum (FBS; HyClone, Logan, UT, USA), N-acetyl-
Differentiation of Culture-Expanded ADSCs
Adipogenic Induction
ADSCs were seeded in a six-well plate at 1 × 105 cells/well and grown to 70% confluency in keratinocyte SFM-based medium (Gibco) containing 10% FBS, N-acetyl-
Osteogenic Induction
ADSCs were seeded, cultured, and induced as described above. The differentiation medium was DMEM containing 10 mM β-glycerophosphate (Sigma-Aldrich), 0.1 μM dexamethasone, 0.2 mM ascorbic acid (Sigma-Aldrich), and 2 mM
Chondrogenic Induction
ADSCs were seeded and grown to 70% confluency as described above. Differentiation was induced using the differentiation kit (Lonza, Walkersville, MD, USA) according to the manufacturer's instructions. Cells were cultured for 21 days with medium changes every 3 days. Chondrogenic differentiation was detected by staining with Alcian blue (Lifeline Cell Technology LLC).
Characterization of ADSC Surface Phenotype
Trypsinized ADSCs were suspended in 500 μl of PBS containing 5% FBS (HyClone). Cells were incubated with the indicated antibody conjugated with fluorescein isothiocyanate or phycoerythrin 20 . Antibodies against CD14, CD29, CD44, CD45, and human leukocyte antigen (HLA)-ABC were obtained from Dako (Carpinteria, CA, USA). Antibodies against CD34, CD73, CD90, and HLA-DR were from Becton Dickinson (Franklin Lakes, NJ, USA). ADSC surface markers were characterized using a flow cytometer (FC500; Beckman Coulter, Brea, CA, USA).
Genetic Stability of Culture-Expanded ADSCs
Array Comparative Genomic Hybridization (aCGH) Assay
Genomic DNA was fragmented by heating at 98°C for 15 min. Labeling reactions were performed with 1 μg of fragmented DNA and an Agilent SureTag Genomic DNA Labeling Kit (Agilent Technologies, Santa Clara, CA, USA) according to the manufacturer's instructions in a volume of 26 μl with a modified dNTP pool containing 120 μM each of deoxyadenosine triphosphate (dATP), deoxyguanosine triphosphate (dGTP), and deoxycytidine triphosphate (dCTP); 60 μM deoxythymidine triphosphate (dTTP); and 60 μM of either Cy5-dUTP (for the experimental sample) or Cy3-dUTP (for the reference) (PerkinElmer, Boston, MA, USA). Labeled targets were subsequently cleaned up using an Amicon Ultra 30K column (Millipore, Billerica, MA, USA). DNA from donor 1 whole blood was hybridized against DNA from late culture cells (P4, P8, P10, and P12). Experimental and reference targets for each hybridization were pooled and mixed in 110 μl of hybridization mixtures of 5 μl of human Cot-1 DNA (Invitrogen) and 11 μl of Agilent blocking agent in 1× hybridization buffer. Before hybridization to the array, the hybridization mixtures were denatured at 98°C for 3 min and incubated at 37°C for 30 min. To remove any precipitate, the mixture was centrifuged at ≥14,000× g for 1 min, and the supernatant was transferred to a new tube. The labeled and denatured DNA target was then hybridized to a SurePrint G3 Human CGH 4 × 180K microarray (G4449A; Agilent Technologies) at 65°C for 40 h. The arrays were then washed in 0.5× SSC/0.005% (w/v) Triton X-102 (Sigma-Aldrich) (wash 1) at room temperature for 5 min, followed by 0.1× SSC/0.005% Triton X-102 (wash 2) at 37°C for 5 min.
After drying, hybridized arrays were scanned on an Agilent DNA microarray scanner at 535 nm for Cy3 and at 625 nm for Cy5 at a resolution of 2 μm. Scanned images were analyzed by the Feature Extraction Software v.10.5.1.1 (Agilent Technologies), an image analysis and normalization software used to quantify signal and background intensity for each feature and substantially normalize the data by the linear normalization method. Data analysis was performed using DNA Analytics v.4.0.81 (Agilent Technologies).
Endotoxin Test
Limulus amebocyte lysate (LAL) assay is a quantitative method to detect gram-negative-derived endotoxin in a solution. LAL is an aqueous extract of blood cells (amebocytes) from the “horseshoe crab,” Limulus polyphemus. The rate of reaction depends on the concentration of endotoxin present.
The Pyrochrome® LAL kinetic chromogenic assay (CapeCod, East Falmouth, MA, USA) was used to determine the presence of endotoxin in cell biological production. Samples were diluted using LAL reagent water. A series of five endotoxin standards (10, 1, 0.1, 0.01, and 0.001 EU/ml) were generated using control standard endotoxin (CSE; 10 ng/vial). A 96-well plate loaded with 1:1 ratio of samples and Pyrochrome® reconstitution reagent was placed in an absorbance microplate reader (BioTek, Winooski, VT, USA), shaken for 10 s, and the assay was carried out at 37°C for 2 h. A measurement filter of 405 nm was used. The test system was set up using the Gen5 software (BioTek). The concentration of endotoxin present in the sample was calculated from reaction time using a standard curve, where the rate of color change was directly proportional to the amount of endotoxin present. The high and low points in a valid standard curve determine the lower and upper levels of endotoxin that can be detected. The endotoxin test is in compliance with the US Pharmacopoeia (USP).
Sterility Test
The test for sterility is carried out under aseptic conditions. Fluid thioglycollate medium (FTM) is primarily intended for the culture of anaerobic and aerobic bacteria. Soybean casein digest medium (SCD) is suitable for the culture of both fungi and aerobic bacteria.
The sterility testing method was performed by both direct inoculation with 1 ml of direct inoculum for each tryptone soy broth (TSB) and FTM medium (15 ml), with FTM incubated at 30°C–35°C and TSB incubated at 20°C–25°C. Media were observed daily for 14 days. If a sample was turbid by visual inspection, it was contaminated by microorganisms. If a sample was clear by visual inspection, it was aseptic. The sterility test is in compliance with the Chinese Pharmacopoeia and USP.
Mycoplasma Test
Mycoplasma is a prokaryotic organism that is a frequent and occult contaminant of cell cultures. Because of their small size, mycoplasmas can pass through filters used to prevent bacterial and fungal contamination and potentially spread to all the cultures in a laboratory. Mycoplasmas are specifically detected by amplifying a highly conserved rRNA operon or, more specifically, a 16S rRNA coding region in the mycoplasma genome.
A half milliliter of cell culture suspension or cell biological production was lysed by incubation at 95°C for 10 min and centrifuged for 5 s at 13,000 × g. The DNA of each sample was extracted using Microsart® AMP Extraction kit (Minerva Biolabs, Berlin, Germany) according to the manufacturer's instruction.
The quantitative real-time polymerase chain reaction (qRT-PCR) was set up in accordance to the instruction leaf let of the Microsart® ATMP Mycoplasma kit (Minerva Biolabs). All necessary solutions for the qRT-PCR, including the internal control DNA and the positive control DNA, were provided in the kit. In each qRT-PCR, the positive and negative controls were processed in parallel with the tested samples to identify possible false-negative results and contamination. Thermal profiles were as follows: for single-step qRT-PCR the denaturation, annealing, and elongation temperatures and times used were 95°C for 30 s, 55°C for 30 s, and 60°C for 45 s, respectively, for 45 cycles, using an Eco™ Real-Time PCR System (Illumina, San Diego, CA, USA). The presence of mycoplasma DNA in the sample is indicated by an increasing fluorescence signal in the FAM™ channel (Cq <40) during PCR.
Thioacetamide-Induced Liver Cirrhosis Animal Model
Thioacetamide-induced liver cirrhosis animal model was examined at a good laboratory practice (GLP) facility at Dong Hwa University Animal Center with the approval of the Institutional Animal Care and Use Committee (IACUC). Thioacetamide (Sigma-Aldrich) was injected intraperitoneally at 200 mg/kg into 8-week-old male Wistar rats (n = 90; Lasco, Taipei, Taiwan) every 3 days for 60 days. After the final injection on day 60, rats were randomly divided into three groups: ADSC treated (n = 30), normal (n = 30), and sham (n = 30). After transplantation, five rats per group were euthanized on weeks 1, 2, 4, 8, 16, and 24. Liver tissue was collected for cell tracking using immunohistochemical staining with a human mitochondria antibody (1:200 dilution; Millipore).
Transplantation of ADSCs
Culture-expanded ADSCs were resuspended in normal saline using a 29-gauge syringe at a concentration that would yield a dose of 5 × 106 cells/kg in a 600 μl volume. For each rat, the suspension was divided between two syringes for injection at two sites in the liver parenchyma (x's in Fig. 3A). The needles were inserted deeply into the parenchyma and slowly withdrawn, pausing at three different depths for 15 s each at the injection site to release 100 μl of suspension. The middle of the liver parenchyma was used for analysis. These procedures were performed following GTP guidelines of both the US and Taiwan FDAs18,19.
Immunohistochemistry
Sectioned liver samples were deparaffinized and processed using the InnoGenex immunohistochemistry kit (HC-2409–06; InnoGenex, San Ramon, CA, USA). A primary antibody against human mitochondria (1:200 dilution; Millipore) was used. Bound primary antibody was detected by serial addition of biotinylated secondary antibody, horseradish peroxidase (HRP)–streptavidin conjugate, and diaminobenzidine substrate (Thermo Fisher Scientific, Waltham, MA, USA). The antigen-positive area appeared brown in color under micros copic observation.
Tumorigenicity and Toxicity Test
Tumorigenicity and toxicity were examined at a GLP facility at the China Medical University Animal Center with the approval of the IACUC. Six-week-old BALB/c-nu nude mice (n = 30, male) were purchased from BioLASCO Taiwan Co., Ltd. (Taipei, Taiwan) and kept for 1 week. Test groups were divided into low-, medium-, and high-dose groups receiving 1 × 106/kg (i.e., 2.5 × 104/100 μl of saline per mouse), 1 × 107 kg (i.e., 2.5 × 105/100 μl of saline per mouse), and 1 × 108 kg (i.e., 2.5 × 106/100 μl of saline per mouse) of ADSCs, respectively. To compare tumor formation, negative (human fibroblast 1 × 106/kg, i.e., 2.5 × 104/100 μl of saline per mouse) and positive [human glioblastoma (GBM) 84,011 × 106/kg, i.e., 2.5 × 104/100 μl of saline per mouse] control groups were also prepared. Each group had six mice.
Cells were injected subcutaneously, and animals were observed twice a week for 24 weeks for clinical symptoms and the presence of tumors. At the end of 24 weeks, the mice were sacrificed, and tissues were removed. Tumor dimensions were measured using a caliper, and tumor size was calculated using the equation (length × width 2 )/2.
Results
Isolation of ADSCs
ADSCs were isolated from three donors (two males, one female) with an average age of 54 ± 3.60 years and an average body mass index of 16.45 ± 1.20. The average number of live ADSCs isolated was 1.48 × 105 ± 1.5 × 104 cells/g tissue. There was no clear correlation between the number of ADSCs isolated and donor age. Donor characteristics and ADSC information are presented in Table 1.
Characteristics of Human Donors and the Genetic Stability of ADSCs
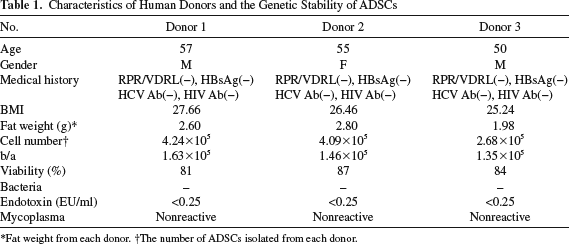
Fat weight from each donor.
The number of ADSCs isolated from each donor.
Morphology of Culture-Expanded ADSCs
ADSCs were expanded in culture 103-fold over four passages and were examined by phase-contrast microscopy (Fig. 1A–C).

Multilineage differentiation of culture-expanded ADSCs from three donors. Morphology of adipose-derived stem cells (ADSCs) from three donors. (A–C) Oil red O staining of adipocytes after 14 days of induction. (D–F) Alkaline phosphatase staining of osteocytes after 14 days of induction. (G–I) Alcian blue staining of chondrocytes after 21 days of induction. (J–L) Magnification: 100×. Scale bars: 100 μm.
Differentiation of Culture-Expanded ADSCs
ADSCs from all three donors were evaluated for their ability to differentiate into adipocytes, osteoblasts, and chondrocytes in culture after exposure to appropriate differentiation media. At 14 days of induction, culture-expanded ADSCs contained large Oil red O-positive lipid droplets in the cytoplasm (Fig. 1D–F). In addition, they exhibited alkaline phosphatase staining representing calcium deposition, and their morphology changed from spindle shaped to cuboid (Fig. 1G–I). At 21 days of induction, Alcian blue staining was visible in the cytoplasm (Fig. 1J–L). These data show that culture-expanded ADSCs had the ability to differentiate into a variety of cell types.
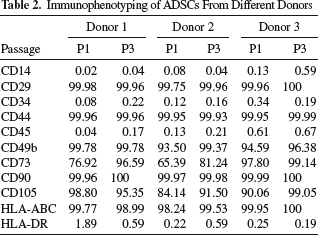
Immunophenotyping and Genetic Stability of Culture-Expanded ADSCs
ADSCs from all three donors were immunolabeled for surface protein expression and examined by flow cytometry. The ADSCs were positive for CD29, CD44, CD90, and HLA-ABC, but were negative for CD34, CD45, and HLA-DR (Table 2). Next, in order to understand the genetic stability of ADSCs during proliferation, we analyzed the aCGH at different passages. No chromosomal abnormality was observed up to passage 12 (Fig. 2). Cell viability was evaluated on an automatic cell counter and was found to be >90% before cell transplantation (data not shown). To minimize the risk of contamination, we followed the GTP guidelines of both the US and Taiwan FDA when producing ADSCs. No evidence of bacteria, fungi, or mycoplasma was observed before cell transplantation (Table 1). These results indicate that culture expansion is a feasible approach to large-scale production of ADSCs for transplantation.
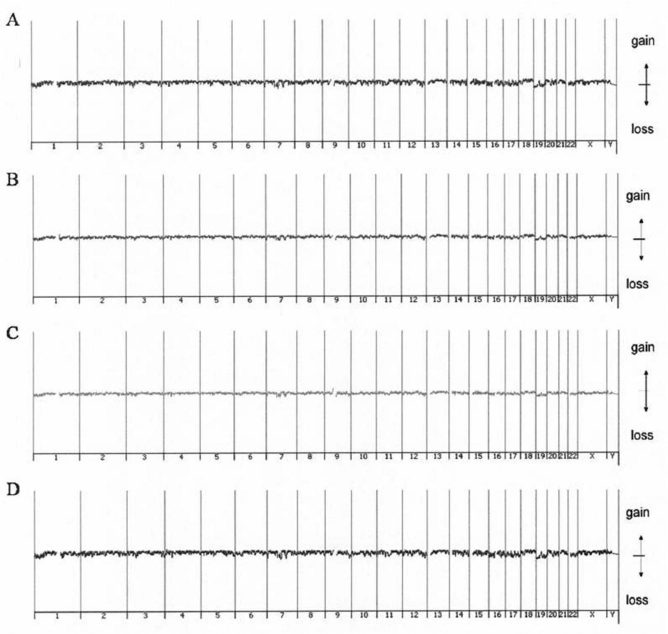
Stability of culture-expanded ADSCs. Representative patterns in genome-wide array comparative genomic hybridization of donor 1 at passages 4 (A), 8 (B), 10 (C), and 12 (D). The ideograms show that no chromosomal anomalies were detected in the culture expansion process.
Immunophenotyping of ADSCs From Different Donors
Intrahepatic Transplantation of ADSCs in Rats with Liver Fibrosis
In order to examine the possible recovery of the liver after treatment by intrahepatic transplantation of ADSCs (Fig. 3A), we evaluated the fibrosis score using Masson's trichrome stain for collagen. We found that collagen accumulation was significantly decreased after 2 weeks of treatment (fibrosis grades 1–2) (Fig. 3B–E). This result suggests that it is feasible to treat liver fibrosis by intrahepatic transplantation of ADSCs.

Efficacy of ADSC transplantation in a thioacetamide-induced liver cirrhosis animal model. Thioacetamide-induced rats were treated with ADSCs from donor 1 by intrahepatic injection at two sites (indicated in dark gray; A). Masson's trichrome stain was performed at 1 week (B), 2 weeks (C), 4 weeks (D), and 8 weeks (E) after injection. Magnification: 400×. Scale bars: 200 μm.
Biodistribution of Transplanted Cells
In order to determine the biodistribution of ADSCs after injection, liver specimens were paraffin embedded, and histological sections were stained with anti-human mitochondria antibody to track the cells (Figs. 4 and 5). ADSCs were retained within the liver (Fig. 4) and spleen (Fig. 5) and were not detectable in the heart, lung, pancreas, or kidney. The signal decreased progressively over time and was no longer detectable in the liver or spleen of any rats by 24 weeks (Figs. 4F and 5L).

Cell tracking and kinetics after liver engraftment. Thioacetamide-induced rats were treated with ADSCs from donor 1 by intrahepatic injection. Immunohistochemical staining was performed with anti-human mitochondria antibody at 1 week (A), 2 weeks (B), 4 weeks (C), 8 weeks (D), 16 weeks (E), and 24 weeks (F) after injection. Magnification: 400×. Scale bars: 200 μm. The black arrows are pointing to the transplanted ADSCs.

Biodistribution of ADSCs after transplantation. Thioacetamide-induced rats were treated with ADSCs from donor 1 by intrahepatic injection. Immunohistochemical staining was performed with anti-human mitochondria antibody at 1 week (A, D, G, J, M), 8 weeks (B, E, H, K, N), and 24 weeks (C, F, I, L, O). Magnification: 400×. Scale bars: 200 μm. Rats were divided in three groups of five animals each. The black arrows are pointing to the transplanted ADSCs.
Tumorigenicity and Toxicity in Animals
The tumorigenicity of ADSCs was conducted by injecting male nude mice and examining them for 24 weeks. In the positive control group (injected with GBM8401 cells), the tumor size became excessive at 24 weeks after transplantation (Fig. 6A). In the ADSC treatment group, no tumor formation was detected over the course of the experiment in any of the three dose groups (Fig. 6A). There was no significant difference in body weight among the five treatment groups (Fig. 6B), and no clinical or behavioral abnormality was observed. These results indicate that ADSCs injected at a dose of up to 1 × 108 cells/kg did not induce tumors.

Tumorigenicity in animals. Tumor volume in male BALB/c-nu mice inoculated subcutaneously with three different doses (1 × 106, 1 × 107, and 1 × 108 cells/kg, represented as 1×, 10×, and 100×, respectively) of ADSCs from donor 1, human fibrosis (negative control), or human glioblastoma (GBM8401) cells (positive control). Tumor size (A) and body weight (B) were measured for 24 weeks. Error bars represent standard deviation.
Discussion
Using MSCs to treat liver disease is an intriguing prospect for regenerative medicine. The major challenge is ensuring an adequate quantity and quality of MSCs. In an earlier study, we obtained MSCs from Wharton's jelly 8 , bone marrow 20 , and adipose tissue 7 . ADSCs have multiple advantages for cell therapy applications. In 2005, Strem et al. reported that the BM-MSCs constitute 0.001% to 0.004% of nucleated cells in the bone marrow 21 . In contrast, ADSCs represent ~2% of nucleated cells in lipoaspirated fat 15 . On average, 1 g of fat contains ~5,000 ADSCs, whereas 1 ml of bone marrow contains 100 to 1,000 BM-MSCs 17 . In addition, clinical samples of bone marrow can only be obtained in limited quantity, whereas adipose tissue is usually available in abundance17,22. Finally, the safety of the tissue isolation procedure is another important consideration. In 1999 and 2000, there were no deaths resulting from 66,570 liposuction procedures, and the rate of serious adverse events was only 0.068% 23 . Thus, adipose tissue offers a better source for obtaining the quantity of MSCs needed for personalized therapy in liver disease patients.
Even with this increased yield, the demand for ADSCs generally exceeds their availability for personalized therapy. The current stem cell transplantation dosage for clinical use is 1 × 10 8 ADSCs24–26. According to the report by Lin et al. 17 , 20 kg of fat tissue is needed to isolate this number of ADSCs. This will be a daunting challenge for the liver disease patient, even for healthy people.
To overcome the problem of demand, we previously developed a culture expansion system for ADSCs 7 . Using this system, the ADSCs from lipoaspirates can be expanded 103-fold after four passages (requiring 14 days). Culture-expanded ADSCs maintain their characteristics, including their ability to differentiate, independent of donor age 7 . Moreover, this culture expansion system has been successful in providing adequate quantity and quality of ADSCs in liver cirrhosis patients 24 .
In preclinical trials for liver disease, ADSCs have shown different improvements in liver function7,27,28. It seems therefore not surprising that the methods of isolation, expansion, culture conditions, growth factor supplements, and cell density at plating are likely to impact the therapeutic effect of ADSCs 29 . This study used a commercial process to manufacture ADSCs. Different from the laboratory process, a commercial process must be compliant with current GTP (cGTP) requirements, under the Code of Federal Regulations, Title 21, part 1271, established by the FDA18,19. In this study, we analyzed three healthy volunteers, all of them without infection of rapid plasma reagin (RPR), hepatitis B virus, hepatitis C virus, or human immunodeficiency virus (HIV) (Table 1). Our commercial process was used successfully and reproducibly to isolate ADSCs from the donors. After culture expansion, the ADSCs kept their characteristics and immunophenotyping profile.
For autologous ADSC manufacture, the primary source for ADSC isolation might be an important impact of their future therapeutic potential. Rennert et al. showed that ADSCs from diabetic mice do not have the capacity for soft tissue neovascularization and wound healing 30 . In contrast, our recent clinical trial used the same protocol to produce ADSCs from liver cirrhosis patients 24 , and preliminary results indicate that these ADSCs have the same characteristics as ADSCs from healthy volunteers (unpublished results). This suggests that treatment of liver cirrhosis patients may indeed be possible with ADSCs from an autologous donation.
Recently, there have been some reports of stem cell transplantation as treatment for patients with liver cirrhosis. Suk et al. compared the one-time or two-time injection of 5 × 107 BM-MSCs through the hepatic artery in patients with alcoholic cirrhosis 31 . They showed that autologous BM-MSC transplantation improved histologic fibrosis and liver function. However, two-time BM-MSC transplantation in comparison with one-time BM-MSC transplantation was not associated with improved results in fibrosis quantification and Child–Pugh score 31 . Qi et al. made a system review and meta-analysis of stem cell transplantation from various human tissue sources in cirrhosis patients. This report suggested that liver function could be improved, including prothrombin time (PT), aspartate transaminase (AST), Model for End-Stage Liver Disease (MELD), and Child–Pugh score, with no associated procedure-related complications. However, these benefits were attenuated over time 32 . These findings pointed out that optimal interval of transplantation, transplant rout, and dosage should be elucidated in the future.
This is a preclinical study evaluating the effect of autologous ADSCs after culture expansion under commercial processes. The first in-human trial is ongoing in Taiwan (ClinicalTrials.gov Identifier: NCT02297867) and will enroll six patients with alcoholic cirrhosis 24 . Detailed studies are needed to explore the optimal therapy protocol, including best administration route and optimal cell dose, and taking into account safety considerations as well as efficacy objectives. Given the huge population of liver disease patients who have been infected with hepatitis B or hepatitis C virus, virus-infected subject groups should also be included in future studies.
In conclusion, our study demonstrates that commercial processes for the production of autologous ADSCs may provide an attractive clinical option for the treatment of liver cirrhosis. ADSCs prepared by this process can reach clinical requirements and comply with regulatory guidelines that ensure safety and quality.
Footnotes
Acknowledgment
The authors declare no conflicts of interest.