
Abstract
Osteoarthritis is a chronic degenerative joint disorder characterized by articular cartilage destruction and osteophyte formation. Chondrocytes in the matrix have a relatively slow turnover rate, and the tissue itself lacks a blood supply to support repair and remodeling. Researchers have evaluated the effectiveness of stem cell therapy and tissue engineering for treating osteoarthritis. All sources of stem cells, including embryonic, induced pluripotent, fetal, and adult stem cells, have potential use in stem cell therapy, which provides a permanent biological solution. Mesenchymal stem cells (MSCs) isolated from bone marrow, adipose tissue, and umbilical cord show considerable promise for use in cartilage repair. MSCs can be sourced from any or all joint tissues and can modulate the immune response. Additionally, MSCs can directly differentiate into chondrocytes under appropriate signal transduction. They also have immunosuppressive and anti-inflammatory paracrine effects. This article reviews the current clinical applications of MSCs and future directions of research in osteoarthritis.
Introduction
Aging is becoming a major public health issue worldwide. In older adults, osteoarthritis (OA) is a common chronic degenerative joint disorder involving mostly weight-bearing joints such as the knees and hips. OA patients may suffer from joint pain, joint stiffness, limitations in the range of motion, and joint inflammation (51). In more than 10% of American adults, clinical OA decreases quality of life. Additionally, OA is the fourth most common cause of hospitalization and the most common reason for total knee and hip joint replacement surgeries (79). Risk factors for susceptibility to OA include age, gender (greater risk for females), ethnicity, bone density, estrogen replacement therapy, genetics, and nutrition. In addition, local biomechanical factors including obesity, joint injury, joint deformity, participation in sports, and muscle weakness have been reported to worsen OA symptoms and increase the rate of progression (36).
OA is characterized by the degeneration and destruction of articular cartilage and changes in subchondral bone with osteophyte formation. Pathological changes associated with OA include phenotypic changes in the cells of the superficial layer of the articular cartilage, chondrocyte hypertrophy, and apoptosis (123).
The current medical treatments for OA cannot effectively reverse its progression. Additionally, pharmacological treatments such as acetaminophen, nonsteroidal anti-inflammatory drugs, opioids, topical analgesics, corticosteroids, and hyaluronic acid can only provide symptomatic relief (98), though glucosamine and chondroitin sulfate have shown some protective effects (69). Pharmacological therapies for pain control are more effective when combined with nonpharmacological interventions. Interventions for OA include exercise and the use of bracing and footwear (36).
Despite pharmacological treatment, total joint arthroplasty of the knee, hip, and glenohumeral joint is the most effective treatment, and it can restore joint function to near normal (98). Other treatments such as osteochondral transplantation, autologous perichondral and periosteal grafts, and autologous chondrocyte implantation may not be applicable in OA because the cartilage defects are often too large (36,41,114).
In a recent study, one compound called kartogenin was shown to stimulate mesenchymal stem cells (MSCs) in cartilage to differentiate into chondrocytes, leading to improvements in damaged joints when given at early stages of the disease. The authors showed that differentiation occurs at the diseased joint, and systemic exposure was minimal (54). Thus, small molecules appear to be useful tools for selectively modulating gene transcription in cells and whole organisms and, in this case, have provided new insights into chondrocyte biology that may lead to novel therapies for the treatment of this degenerative disease (54,57).
This review article focuses on stem cell-based therapeutic challenges for cartilage repair in OA. We also explore the current clinical applications of MSCs and future directions of research in OA.
Stem Cells
Stem Cell Therapy
Stem cell therapy provides a permanent, biological solution, and regardless of their source, all stem cells, including embryonic, induced pluripotent, fetal, and adult stem cells, have some degree of potential for regenerative medicine (29,61). Stem cell therapy induces chondrogenic differentiation of stem cells. Therefore, the transplanted cells have to be able to survive in a diseased joint. Catabolic factors such as the presence of interleukin-1α (IL-1α) or tumor necrosis factor-α (TNF-α) in osteoarthritic joints inhibit the chondrogenic differentiation of stem cells, thereby impairing chondrogenesis. Both downregulation of inflammatory cytokines and introduction of chondrocytes are needed to repair diseased joints (55).
Embryonic Stem Cells and Induced Pluripotent Stem Cells
The capacity of stem cells to differentiate and self-renew is also important in regenerative medicine. Embryonic stem cells (ESCs), induced pluripotent stem cells (iPSCs), and mesenchymal stem cells (MSCs) are candidates for stem cell therapy. After extensive research on human ESCs (hESCs) and iPSCs in recent years, almost all cell types of the human body can now be derived from hESCs and iPSCs. The advantages of hESCs and iPSCs in deriving human cells are their capabilities with regard to self-renewal and characteristic pluripotency (30). Although human cells may be derived from many other human stem cell lines, hESCs are the best option for tissue engineering and regenerative medicine for treating many diseases, including Parkinson's disease (PD), amyotrophic lateral sclerosis (ALS), spinal cord injury (SCI), stroke, cardiovascular diseases, diabetes, hematopoietic diseases, liver diseases, and lung diseases (58).
Although iPSCs are superior to ESCs because of their potential for customization for individuals, the limitations of both hESC- and hiPSC-derived cells are the risk of teratoma formation and immunogenicity (105). Mouse embryonic fibroblasts (MEFs) are the most commonly used feeder layers for maintaining hESC growth (2). However, this hESC culture method has been questioned because nonhuman cell components can limit clinical applications in humans. The clinical applications of new methods for maintaining hESCs and hiPSCs, such as feeder-free, serum-free methods, and coculture with other cells of human origin, are also limited by their tumorigenicity (88,128).
Mesenchymal Stem Cells
Recently, various MSCs including bone marrow-derived MSCs (BM-MSCs), umbilical cord blood-derived MSCs (UCB-MSCs), human umbilical cord MSCs (hUC-MSCs), adipose tissue-derived stem cells (ADSCs), muscle-derived stem cells (MDSCs), and dental pulp stem cells (DPSCs) have been used for chondrocyte regeneration. The Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy defined three criteria for identifying human MSCs. First, MSCs must be plastic adherent when maintained in standard culture conditions. Second, MSCs must express CD105, CD73, and CD90, but not CD45, CD34, CD14 or CD11b, CD79α or CD19, and HLA-DR surface molecules. Third, MSCs must differentiate to osteoblasts, adipocytes, and chondroblasts in vitro (32).
Resident MSCs in Joints
MSCs can be found in both synovial and solid joints, which mainly develop from mesoderm. The fact that MSCs can be isolated from synovial membrane, meniscus, ligaments, fat pad, and cartilage of the synovial joints suggests that MSCs play an important role in the maintenance and function of these tissues (31,59,94,101,127). These MSCs are capable of self-renewal and trilineage differentiation. Additionally, synovial MSCs have greater clonogenicity and chondrogenic capacity compared to BM-MSCs (64). Studies have also shown that synovial MSCs can repair cartilage in a rabbit model of OA (48). Nevertheless, synovial MSCs are difficult to extract, and studies are limited. Therefore, no clinical trials have been performed in humans.
Our previous study of isolated infrapatellar fat pad MSCs (IFP-MSCs) found that these cells had greater chondrogenic potential than other sources of MSCs (31). IFP-MSCs are another source of MSCs located in the joints (33,126). Owing to the orthotopic localization and practical accessibility, infrapatellar fat pad stromal cells (IFPSCs) have attracted interest as a potential source of cells for the repair of focal cartilage defects in the knee (56,62,73,126).
Molecular Insight Into Chondrogenesis (Fig. 1)
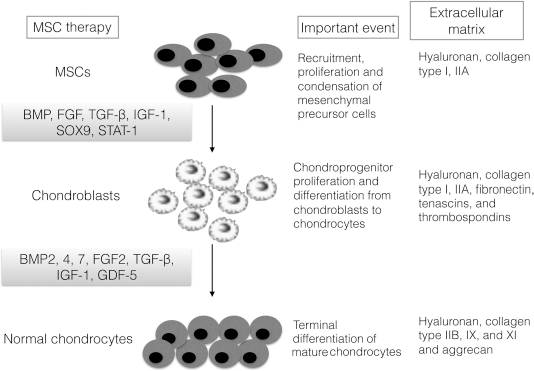
Summary of the key stages of chondrogenic differentiation from MSCs, including the transcription factors involved and expression of ECM component in each stage.
Chondrogenesis begins with the recruitment, migration, and proliferation of chondroprogenitors from MSCs in the early phase of embryonic skeletogenesis (83). The extracellular matrix (ECM) is composed of hyaluronan, collagen type 1, and collagen type 2A1 (Col2a1) (91). Interactions between progenitors and ECM allow progenitor cells to differentiate into chondrocytes and to synthesize cartilage-related ECM such as collagen type IIB, IX, and XI and aggrecan (20). Sox9, a marker of early chondrogenic cells, is essential for the expression of Col2a1, Col11a2, and cartilage-derived retinoic acid-sensitive protein (CD-RAP) (70).
The transforming growth factor-β (TGF-β) superfamily is important for chondrogenesis (12). Bone morphogenetic protein (BMP) is essential for chondrogenic differentiation via the canonical smad pathway and via targeting of Sox9, Col2a1, and Runx2 (21,99). Mitogenactivated protein kinase (MAPK), p38, and ERK1/2 are also linked to regulation of chondrogenesis (13).
The Notch pathway also has a role in early chondrogenesis, and Notch signaling is essential for initial chondrogenic differentiation of MSCs (46).
During chondrogenesis of MSCs, Col10a1 expression causes hypertrophy (46). Strategies known to prevent hypertrophic changes during MSC differentiation include parathyroid hormone-related peptide (PTHrP) or fibroblast growth factor-2 (FGF-2), which are known to downregulate Col10a1 (60).
Therefore, ensuring appropriate chondrogenic differentiation and matrix synthesis by MSCs is essential for avoiding fibrocartilage formation or ossified hypertrophic cartilage.
MSCs, TGF-β, and Cartilage Repair
Interplay between TGF-β and a disintegrin and ADAMTS (a member of the metalloproteinase with thrombospondin motifs family) can modulate the repair response in OA conditions (Fig. 2). The roles of resident MSCs in cartilage or bone in human patients with OA and animals modeled with OA and in cartilage repair may be related to TGF-β and ADAMTS5 (86). ADAMTS5 is the major aggrecanase involved in the degradation of mouse cartilage (42,100). Lack of ADAMTS5 activity resulted in decreased joint fibrosis and cartilage erosion (71). Deletion of ADAMTS5 activity mediated a transition from TGF-β1-stimulated fibrosis to chondrogenesis (113). The dual effect of TGF-β on chondrogenesis was noted when associated with ADAMTS5. TGF-β induced fibrosis in the presence of ADAMTS5 with phosphorylation of Smad2 and Smad3. On the contrary, TGF-β induces chondrogenesis in the absence of ADAMTS5 with phosphorylation of Smad1, Smad5, and Smad8 (113). MSCs may be involved in all of these effects, thus suggesting that MSCs have a role in maintaining healthy joints and in the onset of disease.

The TGF-β signaling pathway. The schematic describes the modulation of TGF-β1 signal transduction through ALK5-fibrogenic pathway and the ALK1-chondrogenic pathway. In the presence of ADAMTS5, ALK5/Smad2/3 signaling is fibrogenic. In the absence of ADAMTS5, ALK1/Smad1/5/8 occurs and promotes chondrogenesis. ALK1 and 5: TGF-β1/TGF-βRII/activin receptorlike kinase 1 and 5.
MSCs, TGF-β, and Bone Pathology
Proliferation of mesenchymal progenitor cells has been associated with osteophyte formation (11). MSC-like cells in the periosteum could respond to TGF-β by phosphorylation of Smad2 and Smad3 and promoting endochondral ossification (11,111). Osteophyte formation might represent another consequence of inappropriate recruitment and activation of MSCs in response to the OA milieu (3,111). Besides ADAMTS5, the ratio of activin-like kinase (ALK1/ALK5) and the relationship between ALK1 and MMP13 (hallmark for OA) also play important roles in chondrocyte behavior. TGF-β can activate ALK5 receptor/Smad2/3 (fibrogenesis) as well as the ALK1 receptor/Smad1/5/8 (chondrocyte differentiation) in chondrocytes. Nevertheless, increased ALK1 expression or an increased ALK1/ALK5 ratio in the cartilage of a mouse model of aging and OA would increase MMP13 expression and cause an OA-like phenotype (10).
MSC Therapy in Joint Repair
The major therapeutic mechanisms of MSCs in OA include their direct differentiation into chondrocytes and their paracrine effects (85). However, MSCs are preferred not only because of their ability to differentiate into a chondrogenic lineage under defined culture conditions but also because they may modulate the immune response (25,90,125). Among various kinds of MSCs, BM-MSCs and ADSCs (27,31) are abundant and can be isolated from adults at risk for OA. Another potential cell source for treating OA are hUC-MSCs. Next, we will discuss the potential of BM-MSCs, ADSCs, and hUC-MSCs for OA treatment, respectively.
Bone Marrow Mesenchymal Stem Cells
The Most Common MSCs
The most common and effective source of MSCs for treating cartilage damage has been bone marrow (4,95,97,130). BM-MSCs can be collected without causing tissue defects by drilling into the bone and aspirating the bone marrow (116). The major harvest sites are the iliac crest, tibia, and femur. Intra-articular injection of MSCs is the most common method for treating OA.
The Attachment of MSCs to Cartilage Lesions
After MSCs are injected into the joint, only a few cells adhere to defective articular cartilage and contribute to cartilage regeneration. However, the molecular mechanisms remain elusive. β-1 integrin was shown to play a key role in MSC attachment to defective cartilage and may pave the way for improved MSC-based therapies in the future (133).
Human Serum Albumin and BM-MSCs in OA
Despite intra-articular injection of steroids and hyaluronic acid, human serum albumin (HSA) was recently used as an anti-inflammatory and pain relief agent in OA patients. The HSA could inhibit peripheral blood mononuclear cells (PBMNCs) and T-cell lines from releasing cytokines (96). This inhibitory activity was lost after HSA dialysis, implicating low molecular weight components of HSA in the inhibitory activity (6).
As result of these findings, the low molecular weight fraction (<5 kDa) of HSA (LMWF5A) is under development as a therapeutic for OA of the knee. In a clinical trial, 329 randomized patients received intra-articular injections of LMWF5A, which resulted in a significant (42.3%) reduction in pain that was observed 4 weeks postinjection (5). In an in vitro experiment, BM-MSCs exposed to LMWF5A exhibited a phenotype with diffuse intracellular F-actin, pronounced migratory leading edges, and filopodia-like projections. Additionally, LMWF5A promoted chondrogenic condensation in “micromass” culture, accompanied with the upregulation of collagen 2A1 mRNA. Furthermore, the CXCR4–CXCL12 axis was significantly regulated during migration and homing. After treatment with LMWF5A, the patient synovial fluid became conducive to stem cell infiltration, self-renewal, and differentiation, as revealed by proteomic analysis. In conclusion, the LMWF5A treatment may prime stem cells for both mobilization and chondrogenic differentiation (7).
Early Use of Mesenchymal Stem Cells
A series of studies by Wakitani and colleagues used BM-MSCs to treat articular cartilage defects (66,118–121). They first reported use of MSCs to repair cartilage damage in humans in 1998 (119). In 2002, the same authors conducted a comparative case study in which BM-MSCs were seeded into gel and collagen sheets and transplanted into patients to treat OA in the knee (118). The transplanted group showed significant improvement in functional recovery and muscle strength compared to the control group. The authors then published comprehensive results on the safety, effectiveness, and long-term effects of MSC transplantation for cartilage repair (121). Their results showed that BM-MSCs are an effective and safe way of treating cartilage defects. During the follow-up period, no tumor formation or infection was noted. Nevertheless, the progression of cartilage destruction could not be reversed in all cases of OA patients (64).
Clinical Trials
In human clinical studies, BM-MSCs are the most commonly used cells for treating OA (15,18,34,103,112). After transplantation of autologous BM-MSCs into diseased knees, the clinical symptoms of pain and decreased walking ability reportedly improved significantly, and cartilage defects were repaired by fibrocartilage (119). Transplantation of BM-MSCs or implantation of autologous chondrocytes can both improve patients' quality of life. In an in vitro study, age reduced overall cell yield and adipogenic potential of the MSC population, while osteogenesis and clonogenicity remained unchanged. This indicates the importance of age as a factor when designing cell-based therapies for patients (8). Patients younger than 45 years reportedly have better outcomes with autologous chondrocyte implantation. However, age has not been reported to make any difference in BM-MSC transplantation (80). Nevertheless, harvesting bone marrow from the iliac crest, tibia, and femur is a painful and invasive procedure that may involve complications and morbidity.
Adipose Tissue-Derived Stem Cell Transplantation
Differentiation Capability
ADSCs can differentiate in vitro into adipogenic, chondrogenic, myogenic, and osteogenic cells (27,31,132). However, the potential for both osteogenesis and chondrogenesis of ADSCs may be inferior compared with BM-MSCs (50). Moreover, in contrast to procurement of BM-MSCs and MDSCs, autologous ADSCs are much easier to obtain by simple liposuction because of the abundance of adipose tissue in the human body (35).
Immunomodulation
Like BM-MSCs, ADSCs also have immunosuppressive properties and do not provoke in vitro alloreactivity of incompatible lymphocytes, and they have been reported to suppress mixed lymphocyte reactions and a lymphocyte proliferative response to mitogens (87). ADSCs reportedly suppress graft-versus-host disease (GVHD) after allogeneic transplantation (129). Interferon-γ (IFN-γ), IL-10, hepatocyte growth factor (HGF), prostaglandin E2 (PGE2), TGF-β1, indoleamine 2,3-dioxygenase (IDO), nitric oxide, leukemia inhibitor factor (LIF), and kynurenine may contribute to the immunosuppressive effects of ADSCs (17,19). Therefore, ADSCs may be considered a good alternative to BM-MSCs for cell transplantation (52,81).
Paracrine Effect
The MSCs have been proposed as a trophic mediator for tissue repair (14). Recent reports have suggested that injected ADSCs indirectly stimulate the secretion of bioactive factors such as cytokines and growth factors (22,39,63,102,104). Intra-articularly injected ADSCs could home to synovium and secrete paracrine factors that have chondroprotective effects, but one study showed that there were no ADSCs found in articular cartilage (65). Paracrine factors produced by ADSCs were suggested to reduce TNF-α and MMP-13 production in articular cartilage and enhance chondroprotective effects (65).
Preclinical Experiments
Much experimental investigation into the therapeutic potential of MSCs was accomplished by treating surgically created chondral or osteochondral defects in small animal models and treating them with MSCs (75,116,117). Nevertheless, such tissue engineering approaches frequently involved the use of scaffolds of different types and yielded variable and unimpressive results. A more direct and successful approach was developed in the treatment of posttraumatic OA in goats (78). In these studies, resection of the anterior cruciate ligament combined with complete medial meniscectomy in the suppressed joint resulted in substantial joint degeneration, with cartilage fibrillation, osteophyte formation, and subchondral sclerosis typical of advanced OA. Intra-articular delivery of MSCs then elicited a meniscal repair response that resulted in clinical improvement in cell-treated joints compared with controls, with evidence of cartilage protection. Implanted MSCs were detected at the surface of the regenerated meniscus and at other synovial surfaces within the joint, but not in articular cartilage (78).
The intra-articular injection of MSCs into the knee joints has been tested in a variety of preclinical disease models such as mice (24), rabbits (106), rats (47), guinea pigs (92), sheep (1), dogs (44), horses (39), and minipigs (45). In these models of surgically induced OA, MSC therapy inhibited OA progression. As well as surgically induced OA, collagenase-induced OA in mice was also modulated by intra-articular injection of ADSCs, with cartilage protection and reduced synovial thickening accompanied by an anti-inflammatory response (104).
Furthermore, fully understanding the mechanisms of improvement using cell-based therapy for OA is essential for future clinical applications. Several mechanisms have been proposed. The transplanted MSCs not only repair or reform tissue but also influence host cell behavior via paracrine effects (78). Moreover, the regenerative actions of the transplanted human MSCs in the injured rat knee joint activated a series of genes including Indian hedgehog (IHH), parathyroid hormone-like hormone (PTH), and BMP2, which resulted in upregulation of type II collagen in the cartilage of the injured knee (47).
Studies using experimental animal models of OA have shown that autologous ADSC transplantation significantly improves clinical, functional, and pathological aspects of the disease (9,44,68,77,104,106,107,109,115, 124,131). Furthermore, xenogeneic ADSC transplantation has not been reported to cause any inflammatory or allergic reactions (93,108).
Clinical Trials
Recent clinical trials have shown that, after intra-articular injections of ADSCs into osteoarthritic knees, the functional score and pain of the diseased knee joints significantly improved without the occurrence of adverse events (82). Cartilage defects have been shown to be repaired by hyaline-like articular cartilage (53,62). In a magnetic resonance imaging (MRI) study, patients with hip osteonecrosis and knee OA were treated with autologous MSC injections in conjunction with hyaluronic acid, platelet-rich plasma, and calcium chloride and had a significantly improved functional score, alleviated pain, and also significantly increased cartilage thickness (84).
Human Umbilical Cord Mesenchymal Stem Cells (hUC-MSCs)
In recent years, hUC-MSCs have received much attention as a potential cell source for tissue engineering and regenerative medicine (25,26,30). hUC-MSCs can be isolated from various areas within the umbilical cord, including the subendothelial layer, perivascular zone, Wharton's jelly, umbilical cord lining, and the whole umbilical cord (25). hUC-MSCs also meet the minimum criteria of plastic adherence, immunological profile, and differentiation potential (32). The many advantages of using hUC-MSCs in tissue engineering and regenerative medicine are the avoidance of ethical issues, a painless harvesting process, few embryonic features, high cell proliferation, wide differentiation potential (28), hypoimmunogenicity (26), and nontumorigenicity (122). Because umbilical cords develop from epiblasts in the embryonic stage, they have some embryonic features (37,38). Therefore, hUC-MSCs have become a promising cell type for regenerative medicine in addition to adult MSCs and ESCs/iPSCs.
hUC-MSCs in OA Research
hUC-MSCs highly express hyaluronic acid, sulfated glycosaminoglycans (GAGs), and collagen (110), which resemble native cartilage. Cartilage regeneration is reportedly high during the chondrogenic differentiation process of hUC-MSCs (23,74). Additionally, persistent expression of an immune-related molecule (CD276) in undifferentiated hUC-MSCs and hUC-MSC-differentiated chondrocytes indicates that hUC-MSCs are immune privileged, which is a feature that is maintained even after they differentiate (67). Three-dimensional culture systems such as nanofibrous scaffolds (40), collagen hydrogels (16), and polycprolactone (PCL)/collagen nanoscaffolds (38) enhanced the propensity of hUC-MSCs to differentiate into chondrocytes. In nanoscaffolds, hUC-MSCs can express more GAG, Sox9, Col2a1, and cartilage oligomeric matrix protein (COMP) compared to BM-MSCs (38). Poly(lactide-co-glycolide) (PLGA) is approved by the FDA and has been used in ligament, tendon, cartilage, and bone regeneration. Experiments have also shown that hUC-MSCs seeded in PLGA scaffolds facilitated cartilage regeneration in a rabbit model with a chondral defect (72).
hUC-MSCs in Clinical Translation
In multiple sclerosis (MS) patients, hUC-MSCs have shown good regeneration capability and tolerable side effects over a 4-year period (49). In a report of hUC-MSCs administered to a patient with MS and in another patient with chronic myeloid leukemia (CML), remarkable effects on the diseases were observed (43).
In summary, hUC-MSCs are easily derived and are sufficiently abundant to meet the demands of tissue engineering and regenerative medicine. Their advantage over other MSCs is that they can be used in translational medicine. In the near future, the use of hUC-MSCs is expected to yield many advances in regenerative medicine (89).
Approaches in Patients with OA
As of September 28, 2015, a search of clinicaltrials.gov with the search terms “mesenchymal stem cell” and “osteoarthritis” yielded 41 studies. Table 1 shows that several of these clinical trials were under way during 2015. All nine of the trials listed on the clinialtrials.gov website from 2014 to 2015 addressed treatment of knee OA. Most studies have involved the use of cultured and expanded autologous MSCs from bone marrow, adipose tissue, and umbilical cord. Most technical approaches involve intra-articular injection to deliver the cells directly into the synovial fluid compartment without using a scaffold. Most studies are in stage I/II, and the testing area distributions are all around the world. Currently, the most common approach is the scaffold-free approach, which indicates that investigative MSC therapy for OA has moved away from early principles of tissue engineering that involved cells, scaffolds, and growth factors. This approach is simpler in terms of technical delivery and regulatory approval compared to multicomponent interventions.
Clinical Trials of Osteoarthritis Treatments Performed During 2014–2015

BM-MSCs, bone marrow stem cells; ASCs, adipose stem cells; hUC-MSCs, human umbilical cord mesenchymal stem cells; PRP, platelet-rich plasma.
Conclusions and Future Prospects
OA is associated with progressive and irreversible destruction of joint tissues. However, a clear mechanistic origin of the disease remains elusive. Figure 3 shows the three major ways to recruit MSCs for articular cartilage repair: first, direct intra-articular injections of MSCs; second, surgical implantation of MSCs containing biomaterials; and third, produce microfractures of the diseased joints to directly recruit endogenous MSCs from underlying bone marrow. Nevertheless, a single therapy usually only brings a short-term effect (64).

Recruitment of stem cells for articular cartilage repair. (a) Direct intra-articular injections of stem cells in suspension. (b) Implantation of cells with biomaterials. (c) Microfracture: directly recruiting MSCs from the underlying bone marrow.
For cartilage regeneration, chondrogenic differentiation of MSCs raises the risk of hypertrophy and ossification of MSCs, and it remains to be seen whether such events occur in discongenic differentiation strategies. Such risks may be decreased through careful selection of the MSC source, one of which is hUC-MSCs. Careful tailoring of treatment regimens to patients' needs is also critical for a successful treatment outcome.
For treating OA, MSC therapy has a dose-dependent effect, and larger quantities of cells are more effective. As for ADSCs, liposuction provides a sufficient number of cells without the need for in vitro expansion, which saves both time and cost (53). Therefore, future research and clinical trials of combination therapies of high-dose ADSCs, chondrocytes, appropriate biomaterial scaffolds, growth factors, and medical and surgical interventions to form hyaline cartilage and repair damaged joints are needed (76).
As in other cellular therapies evaluated in 2015, clinical applications have been limited. An emerging database from phase I and II trials will shed further light on the therapeutic utility of intra-articular delivery of MSCs. Approaches involving either autologous or allogeneic cells may provide an effective treatment for OA.
Footnotes
Acknowledgments
The authors sincerely thank the Buddhist Tzu Chi General Hospital for the financial support (Contract Nos. TCRD 103-26, 103-27, 104-08, TCRDI 104-01-03). Ted Knoy is appreciated for his editorial assistance. The authors declare no conflicts of interest.