
Abstract
Type 1 diabetes mellitus (T1DM) is a form of early onset diabetes mellitus characterized by the autoimmune destruction of insulin-producing cells (IPCs), resulting in hyperglycemia and abnormal glucose metabolism. There are currently no treatments available capable of completely curing the symptoms associated with the loss or functional defects of IPCs. Nonetheless, stem cell therapy has demonstrated considerable promise in the replacement of IPCs with immunomodulatory functions to overcome the defects caused by T1DM. Adipose-derived stem cells (ADSCs) are particularly suitable for use in cell transplantation therapy, especially when seeking to avoid the ethical issues and tumorigenic complications commonly associated with embryos or induced pluripotent stem cells. Cell-based treatments have demonstrated therapeutic advantages and clinical applicability of ADSCs in T1DM, ensuring their suitability for transplantation therapy. This manuscript focuses on the benefits and possible mechanisms in a T1DM-relevant model and displays positive results from finished or ongoing human clinical trials. We also discuss and hypothesize potential methods to further enhance the therapeutic efficacy of these efforts, such as a humanized rodent model and gene therapies for IPC clusters, to meet the clinical applicability of the standard.
Keywords
Introduction
The World Health Organization estimated the global prevalence of diabetes at 381.3 million people in 2013, increasing by 4.4% per annum (41). Among these patients, 10% have type 1 diabetes mellitus (T1DM). At present, exogenous insulin injections, hormone substitution, and oral hypoglycemic agents are the main treatment options; however, these methods only deal with the symptoms or condition of the patient and cannot be considered a cure for diabetes (26,58). Once diagnosed with diabetes, most patients require continuous medication or insulin to control the syndrome and prevent deterioration of the condition (75). This can have a direct effect on the daily life of the patients and place a heavy burden on the health care community. In addition, the availability of resources is very limited, and organ transplantation has a high failure rate, which necessitates nonspecific immunosuppression therapy to determine the reliability of insulin independence (12). Therefore, better treatment strategies are necessary for treating the disease.
Stem cells have a self-renewal ability and can be induced to differentiate into specialized cells (20,52,61,95). These unique properties allow stem cells to be regenerative, thereby regenerating cells, tissues, and organs and potentially bringing endless hope for patients (114). Cell-based therapies have been used to generate functional insulinproducing cells (IPCs), modulate immune dysfunction, and restore β-cell functionality in animal models (45,46,120). Previous studies have also demonstrated that stem cell therapy can be applied as an attractive treatment option, with effective differentiation into IPCs to treat insulin-dependent symptoms (50,117). The benefits of stem cell transplantation manifest in immunomodulatory and anti-inflammatory actions, paracrine signaling, transdifferentiation, and the facilitation of angiogenesis (3,11,22,24,84,101). These combined effects can successfully complement β-cells and their function.
Unlike embryonic stem cells, in which their procurement and use are deemed controversial (28), adult autologous stem cells are particularly suitable for use in cell transplantation therapy (69). This treatment also avoids the adverse effects of immunosuppression associated with allotransplantation (57). Adipose-derived stem cells (ADSCs) are widely available, and their isolation from the abdomen, limbs, and face is only slightly invasive (18,21,74,80). These cells exhibit high levels of stem cell-associated antigens and good proliferation and differentiation potential (37,38). They lack human leukocyte antigen (HLA)-DR expression and have been successfully implanted in immunocompetent mice without the requirement of immunosuppressive drugs (67,111).
ADSCs have been used in animal models of diabetes as well as a number of human clinical trials (phase I/II) (110). Extensive clinical trials of ADSCs have been performed, and a number of these have entered phase III (39). This article focuses on the current progress of ADSCs in T1DM animal models and human clinical trials. In addition, the present study investigates various therapeutic mechanisms that may play a role with ADSCs and examine their clinical applicability. We also share a number of recent insights that have enhanced the feasibility of using ADSCs for the treatment of diabetes.
ADSCs
ADSCs are a type of mesenchymal stem cell (MSC) present within adipose tissue, which have a strong proliferative capacity, multiple differentiation potential, and low immune rejection response (6,94). ADSCs can be induced to differentiate into multiple lineages, such as cartilage, bone, fat, nerve, muscle, and other cells (121). Cell surface molecules of ADSCs have been uncovered, including the presence of cluster of differentiation 9 (CD9), CD10, CD13, CD29, CD44, CD49d, CD49e, CD54, CD55, CD71, CD73, CD90, CD105, CD106, CD146, CD166, and STRO-1, and the absence of CD11c, CD11b, CD31, CD34, CD45, CD80, major histocompatibility complex class II, and HLA-DR surface proteins (19,115). Compared with other MSCs, ADSCs enable a longer incubation time and high proliferative capacity, making the adipose tissue a good source of autologous stem cells (122). In addition to the clinical treatment of organ neuropathy, there are many application potentials in tissue engineering and regenerative medicine (63). Developmental plasticity and its therapeutic potential in recent years have triggered much related research.
ADSCs present no safety issues with respect to the genetic and epigenetic instability of the amplified cells (90), immune response (8), and tumorigenicity (78). ADSC surface markers (such as CD73 and CD90) change as a result of prolonged incubation (90). However, this phenotypic alteration is not due to changes in the chromosomes or lethal mutations on DNA, as verified by single-nucleotide polymorphism genotyping. More reports have emphasized that cellular activity is not obviously aberrant after in vitro amplification procedures, and no safety issues have been found to arise after transplantation into animal models (23, 39,83,90). With regard to human trials, patients receiving stem cell transplants as a treatment also did not display any serious adverse reactions (89). In addition, culturing ADSCs with xeno- and serum-free reagents can enhance the safety and quality of the transplanted cells (85). Therefore, in vitro differentiation of ADSCs leads to no safety issues, such as microbial threats, cytotoxicity, unstable biological activity, genetic or epigenetic instability, tumorigenicity, or immune responses.
ADSCs serve multiple functions and therapeutic potentials depending on the differentiation capability of endodermal, mesodermal, and ectodermal progenitors, upon in vitro induction (82). ADSCs have been explored in several functional lineages, including osteoblasts (87), chondrocytes (59), myocytes (72), endothelial cells (77), hepatocytes (68), and neuronal cells (66). Animal models have demonstrated the therapeutic benefits of ADSCs as cell replacement therapy and cell repair functionality (10,60). ADSCs have also been used to treat injury via intravenous administration or in situ injection for the direct recovery of transplanted cells that would subsequently differentiate in vivo and display functional integration (43,116). Repair molecules, such as neurotrophic factors (1), chemokine receptors and ligands (109), immunomodulatory factors (25), inflammatory regulators (31), and antioxidant factors (86), are excreted from transplanted ADSCs. The therapeutic capacity of ADSCs is widely used in a number of clinical trials for the treatment of various human diseases, including amyotrophic lateral sclerosis, depressed scar, multiple sclerosis, perianal fistulas, Crohn's disease, coronary arteriosclerosis, liver cirrhosis, fecal incontinence, limb ischemia, and diabetes (17,39, 66,71,97). Thus, these results prove that ADSCs can be used in human clinical applications because they are highly secure and have therapeutic potential in regenerative medicine.
Types of Diabetes
Diabetic patients have high blood sugar, a metabolic disease characterized by the absolute or relative lack of insulin or insulin resistance, which leads to a series of clinical syndromes (44). In addition, genetics play a major role in diabetes susceptibility (32,35,40). Diabetes is also a systemic vascular disease in which metabolic abnormalities cause the accumulation of glucose, resulting in complications, including chronic microvascular disease (98), such as retinopathy (100), kidney disease (96), and neuropathy (5), as well as the macrovascular disease atherosclerosis (29). There are many types of diabetes, which can be divided into four categories depending on the etiology: T1DM, type II diabetes mellitus (T2DM), gestational diabetes, and others (112).
In T1DM, IPCs are missing owing to an autoimmune response caused by autoreactive T-helper 1 (Th1) cells attacking pancreatic β-cells (7,102), and the progression of T1DM is enhanced by macrophages, dendritic cells, natural killer cells, and lymphocytes (62). Th1 effector CD4+ T-cells and proinflammatory cytokines such as interferon-γ, interleukin (IL)-2, and tumor necrosis factor (TNF)-α play a relevant role in immune response processing (11,42,91). Of these, the regulatory components of autoimmune processes include CD4+CD25+forkhead box P3-positive regulatory T-cells. The β-cell antigens that drive the immune response are normally expressed, whereas the destructive capabilities are caused by the cytokine immunoregulatory circuits (103). In addition, the genetic and environmental factors involved in the protective histocompatibility locus antigen lead to cell death (79,118). Pancreatic β-cells are the only cells that secrete insulin; therefore, the complete obliteration of these cells leads to an absolute lack of insulin production, resulting in diabetes (105). Susceptibility to this disease is determined by a strong genetic background; however, environmental factors, although not fully understood, are thought to trigger the initial injury (28). Despite the rescue, intervention is not enough to prevent long-term complications, often including vascular degeneration, blindness, and kidney failure.
The major feature of T2DM is insulin resistance, which occurs following the adverse reactions of metabolic homeostasis, inflammation, and the immune response (112). T2DM is associated with reduced pancreatic β-cells, mainly because of cell apoptosis, an effect of high blood sugar, high cholesterol, and insulin resistance (93). With a reduction in pancreatic β-cells and progression of insulin resistance, the relative lack of insulin production thus results in diabetes. Although the cause of T1DM and T2DM differs, inadequate amounts of insulin production to maintain normoglycemia is a similar feature between the two diseases (103). Gestational diabetes mellitus is similar to T2DM, with the combination of a lack of insulin production and response, due to uncoordinated hormone secretion during pregnancy (70,76). Other unusual types of diabetes may be caused by cystic fibrosis, hemochromatosis, surgical causes, and drug causes (4).
Relevant Animal Model
A rational and improved animal model, to mimic the main pathological mechanisms and symptoms, is required for scientists to investigate the molecular mechanisms and potential therapeutic effects of cell-based therapy (16). Up to now, most ADSC-based treatments for T1DM have involved nonobese diabetic mice (NOD) and streptozotocin (STZ)-induced diabetic rodents as animal models (11,55). A commentary by von Herrath et al. describes important diabetes models of T1DM, including NOD rodents such as NOD H-2k, NOD DQ8, and NOD H-2g7 strains (Table 1) (113). Depending on the characteristics of genetic heterogeneity and susceptibility to autoimmunity, the NOD rodent is the major model of the T1DM preclinical research. In addition, STZ-induced rodent models are widely used for generating hyperglycemia and destroying IPCs, resulting in typical syndromes such as polyphagia, polydipsia, and polyuria (104). Although the mechanism underlying the development of diabetes differs between NOD autoimmune and STZ-induced models, both can still create symptoms similar to those of T1DM, such as insulin dependency, hyperglycemia, and impaired metabolism (56). The author indicated that STZ treatment could prevent and even reverse the autoimmune destruction of pancreatic islets in NOD mice. This paradoxical phenomenon, also described by Rayat et al. (92), may be attributed to protective mechanisms in which STZ alters islet-specific cell antigens or directly affects the immune system of NOD mice.
The Applications of ADSCs in STZ-Induced and NOD-Deficient Relevant Models

Abbreviation: STZ, streptozotocin; NOD, nonobese diabetic; N.M., no measurement; udADSCs, undifferentiatiated adipose-derived stem cells; SCID, severe combined immunodeficient; VEGF, vascular endothelial growth factor; TEMPI, tissue inhibitor of metalloproteinase 1; CD54, cluster of differentiation 54; MHC, major histocompatibility complex; MSC, mesenchymal stem cell; TNF-α, tumor necrosis factor α; IL-1β, interleukin-1β; MAPK, mitogen-activated protein kinase; Th1, type 1 T helper; Tregs, regulatory T-cells; Sca1, stem cell antigen 1; Pdx1, pancreatic and duodenal homeobox 1; GCK: glucokinase; Isl-1, islet-1; Pax4, paired box 4; Glut2, glucose transporter 2; NeuroD1, neuronal differentiation 1; SST, somatostatin, TNF, tumor necrosis factor; Hnf3b, hepatocyte nuclear factor 3β; TCF2, transcription factor 2; Sox17, sex-determining region Y-box 17; Ngn3, neurogenin 3; Nkx2.2, NK2 homeobox 2; Oct4, octamer-binding transcription factor 4; Rex1, reduced expression protein 1; SCF, stem cell factor.
Therapeutic Effects
Many studies have shown that ADSC treatment of these animal models of T1DM can effectively alleviate syndromes of diabetes (31,65). Previous results have shown that transplantation of cells, including undifferentiated and differentiated IPCs, can be conducted via intravenous, intraperitoneal, peritoneal cavity, and renal capsule administration. The current information with regard to the application of ADSCs in rodent relevant models is summarized in Table 1. To investigate the potential therapeutic capability of MSCs in T1DM, the intravenous administration of autologous undifferentiated ADSCs (udADSCs) (immunotyping: CD29+, CD44+, CD34-, CD45-) was conducted in STZ-induced Sprague–Dawley rats (64). The report clearly highlighted reduced fasting blood glucose levels, increased expression of insulin, and improved islet injury over 4 months. A similar study (31) indicated that the administration of udADSCs (immunotyping: CD29+, CD90+, CD34-, CD31-, CD45-, CD13-) can recover the levels of glucose, cholesterol, triglycerides, urea nitrogen, and creatinine as well as increase the levels of insulin. The authors also demonstrated that the renal damage induced by STZ was alleviated through ameliorating oxidative stress; decreasing TNF-α, IL-1β, and IL-6 cytokine levels; and inhibiting the mitogen-activated protein kinase signaling pathway. ADSCs therapy reduced the inflammation of cell infiltration and improved pancreatic expression of insulin and pancreatic duodenal homeobox 1 (Pdx1). Another study (11) using udADSCs (immunotyping: CD105+, CD90+, CD44+, CD73+, CD45-, CD11c-, CD11b-, CD34-) for treating NOD (H2-Ag7) mice by intraperitoneal injection displayed the amelioration of diabetes pathogenesis by attenuating the Th1 immune response.
However, the intravenous administration of udADSCs raises targeting and uncontrolled cell division uncertainties, which may result in reduced therapeutic effects and the risk of tumorigenicity. To overcome the issues of ambiguous cell fates and the performance of IPCs, the in vitro control of stem cell differentiation is a promising strategy for improving the potential therapeutic capacity. ADSCs were immunotyped and then further differentiated into IPCs for transplantation. An ongoing study (49) conducted an in vitro differentiation procedure to generate IPCs by transducing the transcription factor Pdx1, which is important for pancreatic β-cell differentiation. The researchers reported significantly decreased blood glucose levels and increased survival after tail vein injection of Pdx1-transduced ADSCs [immunotyping: paired box 6 (Pax6), Nk2 homeobox 2], wherein they expressed insulin and C-peptide. A similar approach (65) also displayed the treatment of T1DM with Pdx1-transduced ADSCs (immunotyping: Pdx1, insulin, glucagon, neuronal differentiation) transplanted under the renal capsule, leading to recovered blood glucose and improved glucose tolerance.
To prevent islet rejection, there is a potential to generate neoislets for xenografts without immunosuppressants using autologous ADSCs differentiated into IPC clusters. With regard to the survival and therapeutic efficacy of transplanted, artificial IPC clusters, two studies (22,119) have systematically addressed blocking the Fas and TNF death pathways. As a method to support the microenvironment required for transplanted neoislets, Karaoz et al. (51) performed IPC cluster transplantation with MSCs to coat and protect the neo-islets for increasing the number of IPCs and their therapeutic performance. Transplanted IPC clusters still survived for 50 days postxenograft, along with the production of insulin and C-peptide. Thus, methods using differentiated IPCs or clusters are available as an alternative source of islet cell replacement therapy in T1DM.
Immunomodulatory
T1DM is a disease of autoimmune dysfunction targeting IPCs in the pancreatic islets, primarily caused by genetic predisposition or environmental factors (54). To replenish adequate IPCs and reestablish the balance of immunity, cell-based therapy is a main strategy, ameliorating hyperglycemia of early onset autoimmune diabetes (11,34,48,64). Our knowledge of the immunological basis for the pathogenesis is incomplete, so the therapeutic potential of the current cell-based treatments is inadequate (2,33,108). However, ADSCs showed a remarkable ability of immunosuppressive properties, indicating promising therapeutic applications (88). Bassi et al. (11) demonstrated that three intraperitoneal injections of ADSCs can reverse hyperglycemia in 78% of diabetic NOD mice, characterized by increased insulin, amylin, and glucagon-like peptide 1 levels. The recovery of early onset diabetes occurred through restraining the CD4+ Th1-biased immune response as well as enhancing the regulatory T-cells near the pancreatic lymph nodes. These results (11) are the first direct evidence for ADSCs in balancing the autoimmune response, while MSCs have been widely investigated for their immunomodulatory properties in cellular transplantation (9).
Clinical Trials
Potential treatment options of T1DM and insulin replacement therapies have been utilized in patients with immune disorders (Table 2), while the ongoing human clinical trials can be found at http://clinicaltrials.gov/. In 2008, Trivedi et al. (107) displayed a clinical report, approved by the institutional review board, describing the safety and effectiveness of intraportal administration of IPCs (immunotyping: Pax6, islet 1, Pdx1) combined with hematopoietic stem cells into five insulinopenic T1DM patients (2M:3F) without xenogeneic materials. Over a mean 2.9-month follow-up, the five patients exhibited a 30–50% decrease in their insulin requirements and displayed a high level of C-peptide expression. The same group of authors (110) reported a continued study using more patients (11; 7M:4F) and showed effective therapy with relatively simple techniques. Recently, the researchers (27) finished another nonrandomized, openlabeled clinical trial using the infusion of in vitro generated PCs into 10 insulinopenic T1DM patients (9M:1F). These three human clinical trials demonstrated successful alleviation of T1DM symptoms without adverse safety issues, thereby illustrating the potential clinical applicability of ADSCs.
The Current Human Clinical Trials of ADSCs in T1DM Patients
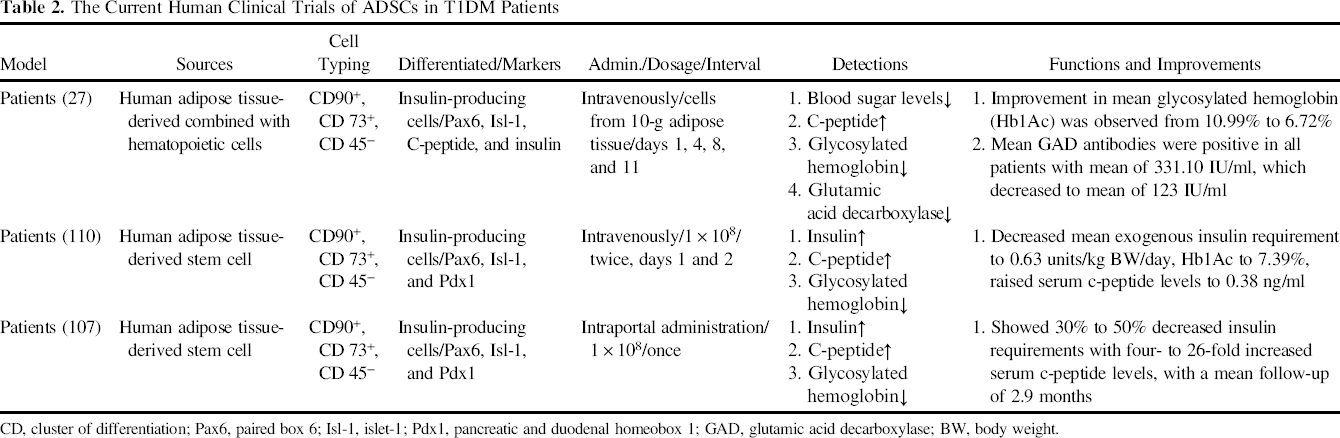
CD, cluster of differentiation; Pax6, paired box 6; Isl-1, islet-1; Pdx1, pancreatic and duodenal homeobox 1; GAD, glutamic acid decarboxylase; BW, body weight.
Discussion and Future Expectation
Various studies using ADSCs recruited from the fat tissues present potential therapeutic capability in T1DM, and safety analysis has been performed for cytotoxicity, immune response, and tumorigenicity. The results showed that ADSCs would have better clinical applicability, since the neoplasm may occur when using autologous MSCs in NOD mice (33,106). Alternatively, recent reports have highlighted the therapeutic potential of ADSCs for congenital causes or acquired factors of diabetes. However, these studies show that the transplantation of not only undifferentiated ADSCs but also differentiated IPCs limited therapeutic ability in partial recovery of syndromes of diabetes with a short effective period. Despite decades of research in rodent models, no therapy or prophylaxis of T1DM has been successfully translated from rodents to humans (15). The major difficulty may be the inability of transplanted stem cells to live long enough in vivo somewhere near the injured pancreas or the inability for proper functional integration of IPCs in response to the physical environment. Thus, there is a requirement for a more effective diabetes therapy, and ADSCs may fill that requirement.
Humanized Rodent Model
The pathogenesis and potential therapeutic capacity of ADSCs in T1DM have been explored; however, considerable differences exist between the immune system and islet components of rodent models and humans (53). Therefore, rodent models may lead to false-positive investigations, leading to a deviation in evaluating the therapeutic effects as well as limiting the human clinical trial results. To mimic the human immune system and islet environment, a more relevant animal model is worth considering because the main cause of T1DM is the autoreactivity against the islet (30). Despite the autoimmunity and islet differences of rodent animals, an advancement has been proposed by transplanting human immune systems into severe combined immunodeficient (SCID) mice (15). The concise idea is to implant a human immune system into genetically modified SCID rodents, the immunodeficient mice recombination activating gene 1 (rag1null) or rag2null, or the genetically mutant interleukin 2 receptor y (IL-2rγ) common chain mouse (15,99). Thus, a humanized animal model provides a preclinical bridge between in vivo studies and the clinical setting to facilitate novel discoveries with regard to the possible pathogenesis and therapeutic possibilities in T1DM (53).
Gene Therapies
Many studies have demonstrated that gene therapy can be successfully applied to treat T1DM and facilitate the transplantation of IPCs integrated in the form of surrogate cells (36). The performance of IPCs as cell replacement and regeneration for treating T1DM may enhance cell survival and function. Pdx1-transfected cell-based therapy was first explored by Ferber et al. (32) as an in vivo attempt to produce surrogate IPCs that can express β-cell-related genes and relieve hyperglycemia. The molecular mechanism of Pdx1 is to regulate reporter activity of genes such as insulin, glucose transporter 2, and neurogenin 3, which function as transcription factors that decide cell fate (14). Lin et al. (65) and Kajiyama et al. (49) also used Pdx1-transduced ADSCs for transplantation into T1DM and showed stable engraftment in the pancreas and recovery of pancreatic function. In addition, the factors controlling the proliferation or transdifferentiation of IPCs generated from other pancreatic cells include hepatocyte growth factor (HGF), glucose-dependent insulinotropic peptide, Pax4, and liver receptor homolog-1 (73). The survival signal pathway commonly targets nuclear factor κ-light-chain-enhancer of activated B-cells and B-cell CLL/lymphoma, while HGF and Pax4 promote transdifferentiation as well as IPC survival and function (73). The performance of stem cells may be enhanced via gene-transfected IPC transplantation in vivo, which can secrete factors to control the cell fates of endogenous pancreatic cells. In summary, gene therapies could be used for manipulating a feasible treatment for the improvement of ADSC-differentiated IPC transplantation.
Coculturing with Pancreatic Islets
Researchers have recently demonstrated that ADSCs possess angiogenic, anti-inflammatory, and paracrine-related immunomodulatory functions (13,64,81). These findings suggest that ADSCs may play various supporting roles facilitating the survival of pancreatic islets and increasing the viability and functionality of grafts. This study developed a microchip-based method for engineering viable and functionally potent islets via coculturing with ADSCs in concave microwells (47). Our results demonstrate that ADSC-exposed islet spheroids have enhanced viability and insulin secretion capabilities and maintain blood glucose levels for prolonged periods following in vivo xenotransplantation of microfiber-encapsulated spheroids. Coculturing primary islets with ADSCs may therefore help mediate cell shortages and enhance the clinical applicability of cell transplant treatments.
Footnotes
Acknowledgments
This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212–113002), CMUBH R103–012, and CMUBH R103–007.