
Abstract
Neurological disorders such as muscular dystrophy, cerebral palsy, and injury to the brain and spine currently have no known definitive treatments or cures. A study was carried out on 71 children suffering from such incurable neurological disorders and injury. They were intrathecally and intramuscularly administered autologous bone marrow-derived mononuclear cells. Assessment after transplantation showed neurological improvements in muscle power and a shift on assessment scales such as FIM and Brooke and Vignos scale. Further, imaging and electrophysiological studies also showed significant changes in selective cases. On an average follow-up of 15 ± 1 months, overall 97% muscular dystrophy cases showed subjective and functional improvement, with 2 of them also showing changes on MRI and 3 on EMG. One hundred percent of the spinal cord injury cases showed improvement with respect to muscle strength, urine control, spasticity, etc. Eighty-five percent of cases of cerebral palsy cases showed improvements, out of which 75% reported improvement in muscle tone and 50% in speech among other symptoms. Eighty-eight percent of cases of other incurable neurological disorders such as autism, Retts Syndrome, giant axonal neuropathy, etc., also showed improvement. No significant adverse events were noted. The results show that this treatment is safe, efficacious, and also improves the quality of life of children with incurable neurological disorders and injury.
Keywords
Introduction
Pediatric neurological disorders include a large group of heterogeneous diseases, of which some are known to be genetic. This group of disorders includes muscular dystrophy, cerebral palsy, and injury including spinal cord injury. These neurological conditions arise from dysfunction of the nervous and musculoskeletal system that lead to impaired movement and abnormal muscle tone (4). Symptoms commonly observed in the children affected by such disorders are motor weakness, change in muscle tone, delayed milestones, headaches, seizures, lack of coordination, etc. (7). An important concern in the treatment of neurological diseases is that the neurons in the brain and spinal cord are unable to instinctively regenerate (7). Stem cells have a unique capacity of self-renewal and differentiation into different types of mature cells. Some stem cells are believed to possess the property of transdifferentiation wherein they can differentiate from one cell type to another within the same tissue or develop into a completely different tissue without acquiring an intermediate undifferentiated progenitor state (9). They are instrumental in the formation of new tissues and thereby promote repair and regeneration. They are obtained from various sources such as preim-plantation embryo, cord blood, bone marrow, and fat tissue (11).
We present the data of a clinical trial conducted to study the result of autologous bone marrow stem cell therapy in pediatric neurological disorders. Seventy-one patients suffering from various incurable neurological disorders underwent autologous bone marrow-derived mononuclear cells transplantation intrathecally and, in certain cases, intramuscularly. It was found to be a safe therapy with no serious adverse events and the quality of life of these patients was shown to exhibit significant improvements.
Materials and Methods
Patients Selection
Patient selection was based on the inclusion criterion of paragraph 35 of the World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subject (3) (i.e., only patients for whom there were no proven interventions available or if available had been ineffective were included). The protocol had been reviewed and approved by the Institutional Committee for Stem cell Research and Therapy (IC-SCRT) in accordance to the Indian Council of Medical Research (ICMR) guidelines. Seventy-one children with neurological disorders such as muscular dystrophy, spinal cord injury, cerebral palsy, etc., underwent the treatment. An informed consent was obtained from the parents and patients evaluated in detail prior to the commencing of the therapy. The exclusion criteria were any disease for which a proven therapy existed or had not been completely tried out, presence of acute infections such as HIV/HBV/ HCV; malignancies, and any other medical conditions such as respiratory infection, fever, etc. Before the therapy all the patients underwent extensive evaluation by a team of medical and rehabilitation experts. The evaluation included a neurological examination, psychological examination, manual muscle testing (MMT) along with disorder-specific scales such as American Spinal Injury Association scale (ASIA) in spinal cord-injured patients, Brooke and Vignos Scale in muscular dystrophy patients, and Functional Independence Measure (FIM) in all. Patients were assessed for pretherapy fitness through routine blood tests, X-rays, etc. Disorder-specific testing such as serum creatine phosphokinase (CPK), electrophysiological assessment like EMG, NCV, SSEP, and EEG, imaging studies of the brain, spine, and musculoskeletal system were performed.
Neurological Evaluation
All patients underwent an initial neurological evaluation. The follow-up period varied from 6 to 24 months with a mean follow up of 15 ± 1 months.
In spinal cord-injury patients, the ASIA Scale was used to evaluate the motor and sensory functions with definitions as:
A: No motor or sensory functions preserved in the sacral segments S4–S5.
B: Sensory but not motor function preserved below the neurological level and includes the sacral segments S4–S5.
C: Motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade less than 3.
D: Motor function is preserved below the neurological level and at least half of key muscles below the neurological level have a muscle grade of 3 or more.
E: Motor and sensory functions are normal.
In muscular dystrophy patients, Brooke and Vignos scales were used to assess the functional limitation. Brooke scale is used for upper extremities ranging from grade 1 to 6, showing increment in the weakness in upper extremities from ability to raise upper extremity completely to not being able to raise hands to the mouth or have any purposeful hand functions.
Vignos scale was used for lower extremities ranging from grade 1 to 10, showing increment in the weakness of lower extremities from ability to walk and climb stairs without assistance to being totally confined to bed or immobile. Patients were evaluated on the basis of these two scales because they are widely accepted assessment tools and clearly show both functional and neurological improvements posttherapy (1,21).
Quality of Life Evaluation
The FIM scale was used to assess the changes in functional abilities thereby improving the quality of life of patients post stem cell transplantation. The FIM assesses the levels of independence from level 1 to 7 ranging from complete independence (timely, safely) in all activities of daily living (ADL) to total assistance required in all ADL. The areas of ADL that are assessed in detail are self-care, sphincter control (bladder and bowel management), mobility (transfers and locomotion), communication (comprehension and expression), social cognition (social interaction, problem solving, and memory) (8).
Radiological Evaluation
Before the treatment, all the patients underwent magnetic resonance imaging (MRI) scans for the specific regions of interest. For all MRI studies a general Electric 1.5 Tesla closed system was used. The MRI was also carried out on follow-up to compare the changes.
Electrophysiological Evaluation
Electromyography (EMG) was done for patients with muscular dystrophy to assess the extent of damage to the muscles and also as a preoperative outcome tool for specific muscles, in which mononuclear cells were to be injected intramuscularly. Nerve conduction velocity (NCV) was performed for all spinal cord injury and muscular dystrophy patients to assess the electrical activity in the motor and sensory nerves. The somatosensory evoked potential (SSEP) test evaluates the nerve pathway from the peripheral nerve through the spine to the somatosensory region of the brain. SSEP was done only for spinal cord injury patients. Electro-encephalography (EEG) was done in patients with cerebral palsy to assess the electrical activity in the brain, as the majority of them had a history of seizures. The pattern of activity in the brain is specific, and when seizures occur, there are clear deviations from normal activity. EEG was carried out as a tool to pick up the abnormal brain electrical activity and also to compare postoperatively in patients whom the parents had reported a reduction in seizure frequency posttherapy.
Granulocyte-colony stimulating factor (G-CSF) injections were administered 48 and 24 h prior to the treatment to mobilize the granulocytes (14).
Isolation and Administration of Autologous Bone Marrow Cells for Administration
Bone marrow was harvested by aspiration under local or general anesthesia depending on the individual case. Approximately 100 ml (varying between 80 and 120 ml based on the age and body weight) of bone marrow was aspirated from the anterior superior iliac crest bone using a standard procedure. Mononucleocytes (MNCs) were obtained after density gradient separation. Viable count of the isolated MNCs was taken. The MNCs were checked for CD34+ by fluorescence activated cell sorting (FACS). Body weight (in kg) x 106 MNCs were injected immediately postseparation, intrathecally in L4–L5, via lumbar puncture using an 18-gauge Touhy needle and catheter over a period of 5–10 min. MNCs diluted in the cerebrospinal fluid, which was obtained via lumbar puncture, were also injected intramuscularly at the specific motor points on the muscles, depending on the individual muscle testing assessed by the physiotherapists during the manual muscle charting prior to the therapy, in reference to the functional limitations reported by the patients. As a general rule of thumb, proximal girdle muscles or weak antigravity muscles like the deltoid, biceps, triceps, abdominals, glutei, quadriceps, hamstrings, tibialis anterior, peroni longus, and brevis of the upper, trunk, and lower limbs were selected for mononuclear cell injection. Simultaneously, the patient was administered intravenous methylprednisolone (30 mg/kg over 1 h) during the mononuclear cell transplantation.
Neurorehabilitation
All the patients underwent extensive rehabilitation, which included physiotherapy and occupational therapy, under the guidance of an expert team of neurorehabilitation specialists, for a period of 6 months to 1 year. The exercise protocol was planned out specifically for individual patients, as per the detailed assessment done before the therapy.
Statistical Analysis
Chi-square test and t-test were carried out for muscular dystrophy and cerebral palsy data. For the other disorders the sample size was too small for statistical analysis. The data were expressed as frequencies in contingency table and chi-square value was calculated. A part of the data was also expressed as means ± SD and t-test was calculated. A significance level of 0.05 was used.
Results
Seventy-one patients diagnosed with incurable neurological disorders and injury such as muscular dystrophy (n = 38), spinal cord injury (n = 4), cerebral palsy (n = 20), and miscellaneous (n = 9) underwent autologous bone marrow-derived mononuclear cell (MNC) transplantation (Table 1). All the patients were administered with body weight (kg) x 106 MNCs. After cell transplantation, the patients had no major side effects. However, some procedural-related side effects (headache, nausea, vomiting, and backache) were noticed in a few cases. In muscular dystrophy, 6 patients complained of headache with 2 having accompanying nausea whereas 9 had backache. Only 1 patient of spinal cord injury reported a mild headache while 5 of the treated cerebral palsy children had severe headache and neck stiffness along with vomiting and nausea. In the miscellaneous group only 1 had backache. All these minor side effects were self-limiting and were relieved in 1 week.
Total Types of Pediatric Patients Underwent Autologous Stem cell Transplantation

Along with the cell therapy, the patients underwent intensive neurorehabilitation consisting of physiotherapy, occupational therapy, and speech therapy. Neurorehabilitation has been shown to promote recovery and independence through neurofacilitation (5). Changes were documented in the ASIA scale for spinal cord injury cases, and Brooke and Vignos scales for muscular dystrophy cases. Quality of life was improved as demonstrated by a shift in the FIM scale in all of the disorders. The statistical analysis showed significant improvement.
In order to quantify the improvements observed, a system was devised that graded the improvements as:
Deterioration: On reassessment, patient showed clinical/ neurological worsening or death.
No improvement: On reassessment, patient was the same as before the therapy.
Mild improvement: Patient reported subjective improvements/caregivers reported ease in handling but no demonstrate able neurological improvement.
Moderate improvement: Patient showed shift in assessment scales (e.g., FIM, ASIA Scale, Brooke and Vignos scales).
Significant improvement: Improvement in assessment scales along with demonstrable neurological improvement and/or improvements in the radiological (MRI) or electrophysiological (EMG) findings.
Muscular Dystrophy
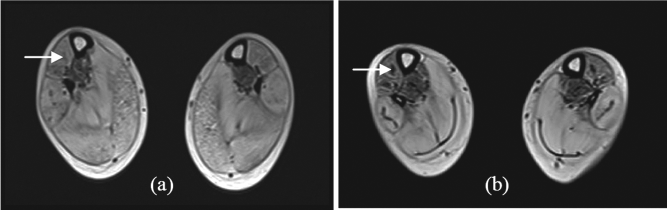
Thirty-eight muscular dystrophy patients (36 were Duchenne muscular dystrophy and 2 were congenital type) underwent autologous bone marrow-derived mononuclear cell transplantation. Symptoms commonly observed among the cases were abnormal gait, scoliosis, hip knee flexion deformity, tendo achilles (TA) tightness, talipes equino varus (TEV) (Fig. 1). Twenty-four patients out of 38 were wheel chair bound. On mean follow-up of 15 ± 1 month post-stem cell administration, 97% of cases showed improvement (Fig. 2) with 28 out of 38 cases (73%) showing improvement in trunk strength and 27 out of 38 cases (71%) showing improvement in lower limb strength, among the others (Fig. 3). On reassessment, 13 improved on Brooke scale, thereby showing improved upper limb strength, and 4 improved on Vignos scale, indicating improved lower limb strength. On FIM, 6 shifted in their scores, showing improved independence in activities of daily living. Comparative MRI (musculoskeletal system) carried out before the transplantation and on follow-up in two of the DMD cases showed a decrease in fatty infiltration with minimal muscle regeneration, generally in the proximal muscles of the limbs, in which mononuclear cells were injected. For example, in one of the patients, these changes were noted in the vastus medialis, vastus lateralis (Fig. 4) and semi tendinosus (Fig. 5) muscle in the thigh as well as in the tibialis anterior (Fig. 6) and medial and lateral head of gastrocnemius (Fig. 7) muscle in the leg. In the arm, improvement was noted in the long and lateral head of triceps muscle and biceps brachii muscle. Thus, features of regeneration were prominently noticed in the muscles that were injected with mononuclear cells.

Graph showing symptoms commonly seen in MD patients (total 38), such as abnormal gait, scoliosis, hip knee flexion deformity, tendo achilles (TA) tightness, talipes equino varus (TEV), and wheel chair (w/c) bound.
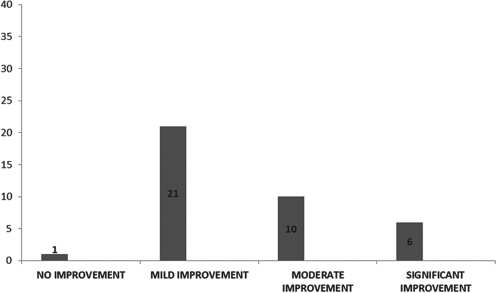
Graph showing improvements after stem cell therapy (total 38) in muscular dystrophy patients.
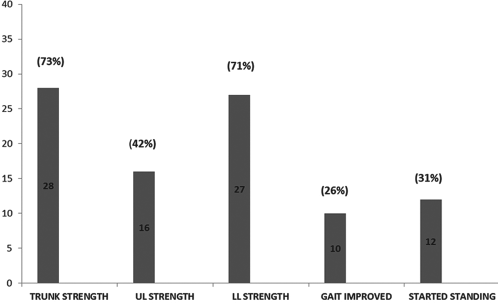
Graph Representing Symptom-Wise Improvements In Muscular Dystrophy Patients (Total 38) With Respect To Their Trunk Strength, Upper Limb (Ul) Strength, Lower Limb (Ll) Strength, Improvement In Gait And Standing.
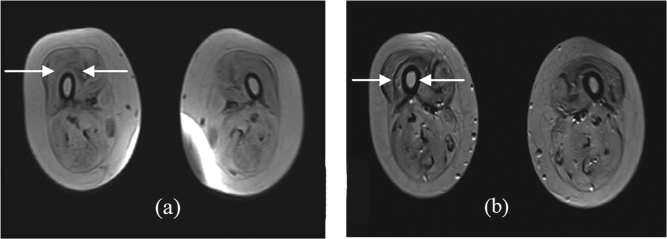
(a) MRI scan of MD patient's vastus medialis and lateralis muscles (arrows) pre-stem cell therapy. (b) MRI scan of MD patient's vastus medialis and lateralis muscles (arrows) post-stem cell therapy showing muscle regeneration.

(a) MRI scan of MD patient's semitendinosus muscles (arrow) pre-stem cell therapy. (b) MRI scan of MD patient's semitendinosus muscles (arrow) post-stem cell therapy showing muscle regeneration.
(a) MRI scan of MD patient's tibialis anterior (arrow) muscles pre-stem cell therapy. (b) MRI scan of MD patient's tibialis anterior (arrow) muscles post-stem cell therapy showing muscle regeneration.

(a) MRI scan of MD patient's medial and lateral head of gastrocnemius muscles (arrow) pre-stem cell therapy. (b) MRI scan of MD patient' medial and lateral head of gastrocnemius muscles (arrow) post-stem cell therapy showing muscle regeneration.
On comparing the EMG carried out before the transplantation and on follow-up, improvements were recorded in 3 patients in most antigravity muscles and also the ones that were injected intramuscularly (e.g., the vastus medialis, tibialis anterior, glutei, deltoid, etc.). Electrophysiological improvements while recording EMG included an increase in the amplitude of motor unit potentials and also increased number of motor unit recruitment compared to before. The amplitude potentials that were recorded as myopathic in a few muscles later showed normal potentials posttherapy.
On reevaluating them on assessment scales, 6 out of 38 patients showed an increase in the FIM scores mainly in areas of self-care and mobility. Six out of 38 showed an improvement in Brooke and Vignos scales.
The statistical analysis of the improvements observed in each symptom of muscular dystrophy was performed using chi-square test and t-test, which showed that the results were significant at the 0.05 level of confidence (Tables 2 and 3).
Statistical Analysis of Effect of Stem Cells on Different Symptoms of Muscular Dystrophy Patients Using Chi-Square Test
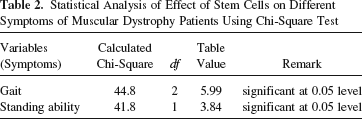
Statistical Analysis of Effect of Stem Cells on Different Symptoms of Muscular Dystrophy Patients Using t-Test

Spinal Cord Injury
Four patients of spinal cord injury (SCI) underwent autologous bone marrow-derived mononuclear cell transplantation. Their major complaints were motor and sensory deficit, abnormal muscle tone and bladder/ bowel incontinence (Fig. 8). On mean follow-up of 15 ± 1 month post-stem cell administration, all 4 patients (100%) showed evidence of varying grades of improvement (Fig. 9). Three out of 4 cases (75%) showed improved muscle strength and better urine control while 2 out 4 (50%) showed improvement in sitting balance and sensation. Tone was normalized in 2 out of 4 (50%) patients (Fig. 10).
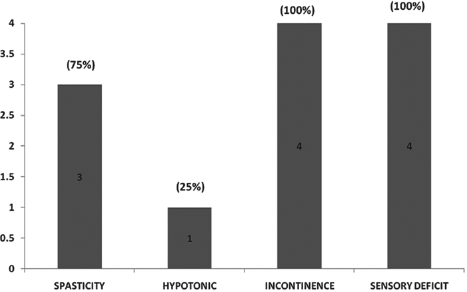
Graph showing major complaints in spinal cord injury (SCI) patients (total 4) like spasticity, hypotonicity, incontinence, and sensory deficit.

Graph showing improvements after stem cell therapy in spinal cord injury (SCI) patients (total 4).

Graph showing symptom-wise improvements in spinal cord injury (SCI) patients (total 4) for muscle strength, sitting balance, urine control, sensation, and reduction in spasticity.
On reassessment, 1 out of 4 patients (25%) shifted on ASIA scale. They were also reassessed on FIM scale, which showed a positive shift in 3 of them, indicating functional improvement mainly in areas of mobility and self-care.
Cerebral Palsy
Twenty cerebral palsy patients, which included cases of dystonic and spastic cerebral palsy, underwent autologous bone marrow-derived mononuclear cell transplantation. Symptoms commonly observed in them were frequent seizures, cognitive impairment, swallowing and speech problems, etc. On mean follow-up of 15 ± 1 months post-stem cell administration, improvement was observed in 85% cases (Fig. 11). Improvement in muscle tone (15/20) and speech (10/20) as well as significant reduction in seizure frequency (2/20) patients and dystonic movements, improved limb strength (11/ 20) patients were observed (Fig. 12). On FIM scale, 3 of them showed improved scores.

Graph representing overall improvements after stem cell therapy in cerebral palsy (CP) patients (total 20).

Graph representing symptom-wise improvements in cerebral palsy (CP) patients after stem cell therapy (total 20) for symptoms like muscle tone, seizure frequency, cognition, swallowing, speech, neck holding, sitting balance, and leg and hand movements.
Symptom-wise statistical analysis of improvements in the cerebral palsy group, with respect to reduction in seizure frequency, cognition, neck holding, sitting balance, postural tone, gross motor ability, and speech showed significant changes (Table 4).
Analysis of Effect of Stem Cells on Different Symptoms of Cerebral Palsy Patients

Other Neurological Disorders
Nine patients of various genetic and other neurological disorders were also administered autologous bone marrow-derived mononuclear cells (Table 5). On mean follow-up of 15 ± 1 months post-stem cell administration, improvements were observed in 89% cases (Fig. 13). On FIM scale 3 of them showed improvement.
Miscellaneous Conditions Treated by Stem Cells


Graph representing overall improvements after stem cell therapy in the miscellaneous group of patients (total 9).
Discussion
Considering the present unavailability of an effective line of management for the above-mentioned disorders, autologous bone marrow-derived MNC transplantation represents an alternative therapy for these neurological conditions for which either there is no treatment available or conventional treatments have failed to work. The MNCs obtained from bone marrow are comprised of a variety of cells like hematopoietic stem cells, tissue-specific progenitor cells, stromal cells, and specialized blood cells in different stages of development. The G-CSF administered before the transplantation helps in stimulation of CD34+ cells and also in their survival and multiplication. Studies have shown that stem cells migrate to the site of injury from the site of injection (2). They work by enhancing angiogenesis and contributing to neovascularization by producing signaling molecules such as vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF2) (20). Along with increase in angiogenesis they also promote tissue remodeling, prevent apoptosis, decrease inflammation, and activate the satellite cells (17). Research shows that cerebrospinal fluid (CSF) is a biological medium that supports the growth, survival, and proliferation of cortical cells both in vivo and in vitro. CSF is known to harbor growth factors that help the growth of the cortical epithelium and promotes vascularization in the nervous system (13). Hence, we have extrapolated these characteristics of the CSF and used it as a diluting medium for the mononuclear cells during the intramuscular injections.
The objective of this study was to demonstrate that the administration of autologous stem cells for incurable neurological disorders, intrathecally and intramuscularly, is safe, feasible, and has the potential to improve the quality of life of the patient. Studies have shown the efficacy and safety of this treatment. Administration of autologous bone marrow-derived stem cells in patients with subacute and chronic spinal cord injuries has resulted in improvements like changes in ASIA scale as well as electrophysiological changes (6,12,19). In case of cerebral palsy, published data have revealed that cell transplantation in patients suffering from cerebral palsy is found to be safe and showed apparent neurological improvements (10,15,16). For muscular dystrophy, trials have been conducted for transplantation of myoblast cells, mesenchymal stem cells, and umbilical cord stromal cells, proving cell transplantation to be safe and efficacious (18,22). We carried out a study on 71 children suffering from various incurable disorders including spinal cord injury, cerebral palsy, muscular dystrophy, and other neurological diseases who underwent autologous bone marrow-derived mononuclear cell transplantation with a mean follow-up of 15 ± 1 months posttransplantation. The results obtained were similar to previously published data. It was observed that none of the children had deteriorated from the time of cell transplantation with respect to their muscle strength, which was confirmed by the manual muscle charting done by the same physiotherapist. Improvements with respect to normalization of muscle tone, balance, etc., were recorded. Experimental studies show that a combination of various therapies such as cellular therapies (stem cells) and exercise (neurorehabilitation and neurofacilitation) together yield better outcome as opposed to single strategies employed independently (22).
In conclusion, autologous bone marrow stem cell transplantation (intrathecally as well as intramuscularly) followed by a comprehensive rehabilitation program is a safe treatment option that produces functional improvements in incurable neurological diseases and injury.
Footnotes
Acknowledgment
The authors declare no conflicts of interest.