
Abstract
Although several human clinical trials using various bone marrow-derived cell types for cirrhotic or decompensated patients have reported a short-term benefit, long-term follow-up data are limited. We analyzed the long-term clinical outcomes of autologous bone marrow cell infusion (ABMI) for decompensated liver cirrhosis (LC). Patients enrolled in a pilot single-armed ABMI study were followed up more than 5 years. Bone marrow-derived mononuclear cells (BM-MNCs) from decompensated LC were harvested and after processing were infused into a peripheral vein. The laboratory test results and long-term clinical course including liver transplantation (LT), development of cancer, cause of death, and survival after ABMI were analyzed. Nineteen patients were followed up for a median of 66 months after ABMI. Liver function, including serum levels of albumin and Child–Pugh (CP) score, was improved at the 1-year follow-up. Liver volume was significantly greater, cirrhosis was sustained, and collagen content was decreased at the 6-month follow-up. Five years after ABMI, five patients (26.3%) maintained CP class A without LT or death, and five patients (26.3%) had undergone elective LT. Hepatocellular carcinoma (HCC) occurred in five patients (26.3%), and lymphoma and colon cancer occurred in one patient each. Three patients (15.8%) were lost to follow-up at months 22, 31, and 33, respectively, but maintained CP class A until their last follow-up. Five patients expired due to infection. While improved liver function was maintained in some patients for more than 5 years after ABMI, other patients developed HCC. Further studies of long-term follow-up cohorts after cell therapy for LC are warranted.
Keywords
Introduction
The end point of liver disease, irrespective of its cause, is liver cirrhosis (LC). Because fibrous scars hardly disappear, a cirrhotic liver does not return to a normal state. Before decompensation, control of the underlying liver disease is important to recover to some degree. After de compensation, patients suffer from repeated and continuous complications, including hepatocellular carcinoma (HCC). At present, liver transplantation (LT) is the only treatment option for patients with HCC.
Although antifibrotic drugs have been developed, their efficacy is limited. Research into bone marrow cells (BMCs) has facilitated the application of cellular therapeutics. In hepatology, hepatocytes from BM have been found in mouse1,2 and human3,4 livers after BMC transplantation, suggesting that BMCs could contribute to liver regeneration. The fate of BMCs injected into fibrotic or injured livers has been investigated5,6. Injected cells migrate to the fibrous area, penetrate into cords of hepatocytes, and produce enzymes that ameliorate fibrosis 6 . Together with BMCs, mesenchymal stem cells (MSCs) have been investigated. Following enhancement of their immunomodulatory and antifibrotic effects in other organ systems, application of MSCs to treat liver fibrosis has shown positive results7-10. For clinical application, MSCs must undergo in vitro selection and culture. A clinical trial using MSCs, therefore, could not start at the initiatory stage in cell therapy until assurance of safety during in vitro manipulation. Although early studies had suggested transdifferentiation of BMCs or MSCs into hepatocytes, mechanisms of action remain poorly understood. Paracrine effects supporting hepatocyte function and liver regeneration and immune modulation are thought to be possible mechanisms 11 .
For clinical application, cell therapy similar to autologous BM stem cell transplantation was first evaluated 12 , as this procedure has long been applied to the treatment of hematologic disease. Subsequent clinical trials of autologous BMCs selected by means of surface markers 13 or injected through the hepatic artery 14 or the portal vein 15 have reported efficacy in terms of liver regeneration after liver surgery or transient improvement of hepatic function. Further trials using BMCs16–18, mobilized peripheral blood mononuclear cells (PBMNCs)19,20, BM-derived endothelial progenitor cells 21 , or BM-derived MSCs (BM-MSCs)22–24 for LC have reported positive short-term results, but the beneficial effects lasted for less than 2 years 23 . However, no study has evaluated maintenance of liver function, survival, and HCC development in such patients at ≥3 years after treatment.
We previously reported the preliminary outcomes of patients who underwent autologous bone marrow cell infusion (ABMI) for advanced LC 25 . Together with gradual improvement of liver function and volume, serial liver biopsies showed an activated progenitor cell compartment after ABMI. A planned single-armed pilot study has been completed, and enrolled patients were followed up for more than 5 years. In this study, the long-term clinical outcomes of patients who underwent ABMI therapy for decompensated LC were analyzed.
Materials and Methods
Patients
Patients enrolled in a pilot trial of ABMI therapy for decompensated LC between June 2006 and February 2011 were analyzed. All patients provided informed consent and met the following inclusion criteria: age 18–75 years, biopsy-proven LC with Child–Pugh (CP) class B or C, platelet count ≥50,000/μl and total bilirubin ≤3.0 mg/dl, and without evidence of HCC on magnetic resonance imaging (MRI). Patients who had a history of HCC without recurrence 2 years after curative treatment were eligible. Patients with a medical condition that made them ineligible for general anesthesia during BM collection were excluded. Patients maintained all medications, with the exception of intravenous albumin. The diuretic dose was adjusted according to the patient's volume status after ABMI. Biochemical tests were performed for 12 months after ABMI. Thereafter, patients were followed up according to their individual clinic visit schedule. Long-term follow-up data were collected retrospectively. In patients who consented to follow-up, LT and development of malignancy, including hepatic function reserve, were monitored. To avoid potential bias, ABMI was considered to have failed in patients who underwent LT.
This study conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the institutional review board (IRB) of Severance Hospital in the Yonsei University Health System (No. 4-2006-0087). This study was conducted with the cooperation of Yamaguchi University Graduate School of Medicine in Japan, under a memorandum of understanding.
Cell Preparation
Under general anesthesia, 500–750 ml of BM was aspirated from both ilia and collected in a plastic bag containing heparin for harvesting of marrow for BMC transplantation. Collected BM was filtered to remove fat and bony particles using a collection and gravity-flow filtration system (BM collection kit; Fenwal Inc., Lake Zurich, IL, USA). Red blood cells and plasma were depleted, and mononuclear cells were collected in a closed system using a COBE 2991 Cell Processor (Gambro, Lakewood, CO, USA). The final volume was ~100 ml. Processed cells were enumerated and tested for viability and contamination. Fluorescence-activated cell sorting (FACS) analysis was performed using a flow cytometer (Cytomics FC 500; Beckman Coulter, Inc., Brea, CA, USA) to evaluate cell populations using cell surface markers [cluster of differentiation (CD) 34, CD45, and CD133 (Miltenyi Biotec Inc., Auburn, CA, USA); CD117 (Immunotech, Beckman Coulter, Marseille, France)]. The final cell product was infused into a peripheral vein over a 1-h period.
Clinical Evaluation
After obtaining informed consent, screening tests were performed to meet the inclusion criteria. Twelve months of clinical follow-up with serial evaluations was conducted. Follow-up visits were scheduled weekly for 2 weeks, monthly for the first 6 months, and then every 3 months for the following 6 months. At each visit, laboratory parameters (complete blood count, serum levels of blood glucose, total protein, albumin, bilirubin, aminotransferases, alkaline phosphatase, γ-glutamyl transpeptidase, urea, creatinine, cholesterol, α-fetoprotein levels, and prothrombin time) were evaluated. Indocyanine green clearance testing was performed before and 6 and 12 months after ABMI.
Liver MRI and biopsies were conducted before and 1, 3, and 6 months after ABMI. All MRI scans to screen for HCC and quantify ascites and liver volume were performed using a 1.5-T MRI scanner (Gyroscan Intera; Philips Medical Systems, Best, The Netherlands). Routine T1-weighted gradient echo, T2-weighted turbo spin echo, T2*-weighted gradient echo, and three-phase, dynamic three-dimensional (3D) T1-weighted images after injection of gadobenate dimeglumine (dose, 0.1 mmol/kg body weight; MultiHance; Bracco SpA, Milan, Italy) were obtained. Total liver volume was measured using commercially available image postprocessing software (Voxel plus 2; Mevisys, Daeduk, South Korea) with one radiologist applying the summation of areas technique using a 10-mm reconstruction thickness. The radiologist was blinded to the patients' clinical information.
Liver biopsies were performed using an ultrasound-guided 16-gauge gun. Transjugular liver biopsy was attempted as an alternative method in cases with massive ascites or a high risk of bleeding. The biopsied liver tissues were routinely processed and stained with hematoxylin and eosin (H&E) and Masson's trichrome. Staining was performed by an autostainer (Symphony staining instrument; Ventana Medical Systems, Tucson, AZ, USA). Unstained slides, available after routine histologic evaluation, were analyzed using a computer-assisted, staining-free method for liver fibrosis assessment by Genesis® 200 (Histoindex, Singapore) 26 .
Statistical Analysis
Serial data from baseline to follow-up visits after ABMI were analyzed. After normality test of data, continuous variables are presented as means ± standard deviations or median (range) accordingly, and categorical variables are presented as absolute values and percentages. Paired-sample t-tests were used to compare values. Data of liver volume did not follow normal distribution; change of liver volume was compared with Wilcoxon's matched-pairs signed-ranks test. All statistical procedures were conducted using PASW Statistics 17.0 (IBM, Armonk, NY, USA). Analyses were based on two-tailed hypothesis tests, and a value of p < 0.05 was considered to indicate statistical significance.
Results
Characteristics of Patients and Cells Infused for ABMI
Twenty patients underwent screening tests, one of whom was excluded according to the exclusion criteria. Therefore, 19 patients underwent ABMI and were followed up. The baseline characteristics of the patients are shown in Table 1. The mean age of the 9 male and 10 female patients was 52 years. Eighteen patients (94.7%) had B-viral LC, and one had alcoholic LC. Sixteen patients had stable hepatitis B with (14 patients) or without (2 patients) antiviral medications. Two patients started antiviral medications, and four patients experienced viral breakthrough during the follow-up period; the antiviral medications of these patients were changed. Three patients had HCC prior to undergoing ABMI. Two patients underwent resection of HCC, and one patient received transarterial chemoembolization and sustained a complete response for >2 years. Fourteen patients (73.7%) had ascites before ABMI. The average CP score of the patients was 7.6, and all but one had cirrhosis of CP class B.
Baseline Characteristics of Patients (N = 19)

Variables are expressed as mean ± standard deviation, median (range), or n (%). HBV, hepatitis B virus; AST, aspartate aminotransferase; ALT, alanine aminotransferase; ICG, indocyanine green clearance test; kPa, kilopascal.
Liver stiffness was measured only in the patients without ascites (n = 5).
The characteristics of infused cells are shown in Table 2. The mean cell number per unit body weight was 0.925 × 108 cells/kg. The average final cell volume after red blood cell (RBC) depletion and concentration was 124.1 ml. These cells were infused over a 1-h period, and no adverse reactions were noted. The majority of the cell population was CD45+ hematopoietic stem cells (83.43%), while CD133+, CD117+, and CD34+ hematopoietic stem cells each made up ~1% of the population. There was no association between cell population and hepatic function improvement.
Composition of Infused Bone Marrow Cells

Variables are expressed as mean ± standard deviation. CD, cluster of differentiation.
Changes in Liver Function
The results of serial blood tests after ABMI were compared to those before ABMI. The results of selected tests related to liver function are shown in Figure 1. The mean serum level of albumin before ABMI was 2.9 g/dl. The mean albumin level during the 6 months before ABMI was also 2.9 g/dl, and this was not improved with conservative management, including use of antiviral agents. This gradually and significantly increased to 3.2, 3.3, 3.4, and 3.4 g/dl at 3, 6, 9, and 12 months, respectively, after ABMI (Fig. 1A). The mean initial level of total bilirubin was 1.6 mg/dl, and it did not change significantly after ABMI (Fig. 1B). The average prothrombin time before ABMI was 70% and improved significantly to 75% at 6 months and 76% at 9 months after ABMI (Fig. 1C). The mean total cholesterol level increased from 123 to 134 mg/dl at 3 months and to 136 mg/dl at 6 months after ABMI (Fig. 1D). Hemoglobin levels increased significantly from 11.6 g/dl before ABMI to 12.3, 12.5, 12.5, and 13.1 g/dl at 3, 6, 9, and 12 months, respectively, after ABMI (Fig. 1E). The initial average CP score was 7.6 and improved significantly after 6, 9, and 12 months to 6.8, 6.7, and 6.7, respectively (Fig. 1F).
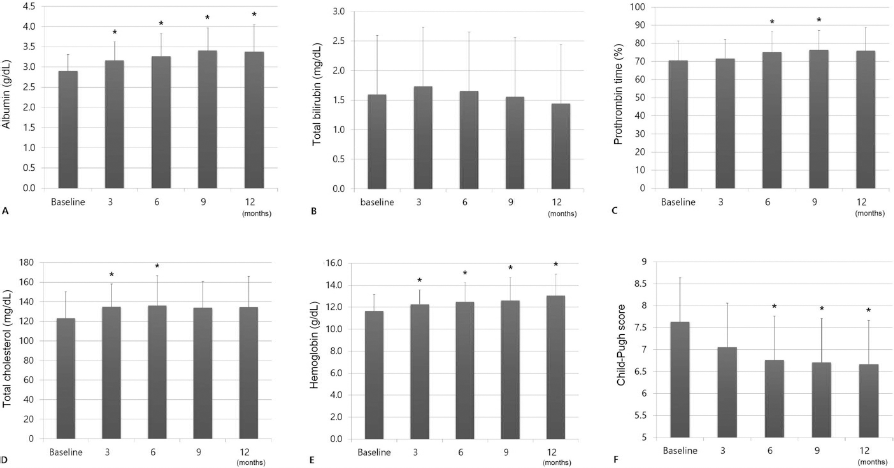
Results of serial blood tests after autologous bone marrow cell infusion (ABMI). (A) Serum levels of albumin gradually and significantly increased at 3, 6, 9, and 12 months after ABMI. (B) Total bilrubin levels did not change significantly. (C) Prothrombin time was significantly better at 6 and 9 months. (D) Total cholesterol level was significantly higher at 3 and 6 months. (E) Hemoglobin level was significantly higher after 3, 6, 9, and 12 months. (F) The Child-Pugh score was significantly better after 6, 9, and 12 months. *p<0.05.
Twelve patients (63.2%) had achieved CP class A within 1 year. This improvement was significantly related only to an increased liver volume after 6 months (p < 0.13). At 24, 36, and 60 months, 11, 7, and 5 patients, respectively, had achieved CP class A without LT or death. Among the five patients with CP class A at 60 months, two had improved to that class after 24 months, while the others were of that class the full 60 months.
Changes in Liver Volume and Fibrosis
All patients underwent MRI at screening, but two patients refused to undergo MRI at the 6-month follow-up. The reconstructed liver volume of the other 17 patients increased significantly at 6 months after ABMI (p = 0.049) (Fig. 2A). Eleven patients (64.7%) showed an increased liver volume compared to baseline. The greatest increase compared to baseline (Fig. 2B, left) was 42% after 6 months (Fig. 2B, right).

Changes in liver volume calculated using magnetic resonance imaging (MRI) scans at 6 months after ABMI. (A) Liver volume significantly increased after ABMI (p = 0.049). (B) Image of the most enlarged liver section image showed a 42% increase in liver volume and decreased ascites at 6 months after ABMI (right) compared to baseline (left). *p<0.05.
According to pathologic evaluation of serial biopsies, ABMI did not lead to resolution of cirrhosis. To compare changes in liver fibrosis, available unstained liver tissues were analyzed in terms of the level of collagen deposition. The percentage of portal collagen decreased significantly at 3 months (Fig. 3A). The septal collagen percentage showed a decreasing tendency after ABMI (Fig. 3B), as did the total fibrillar tissue collagen (fibrosis other than portal and septal fibrosis) percentage (Fig. 3C).
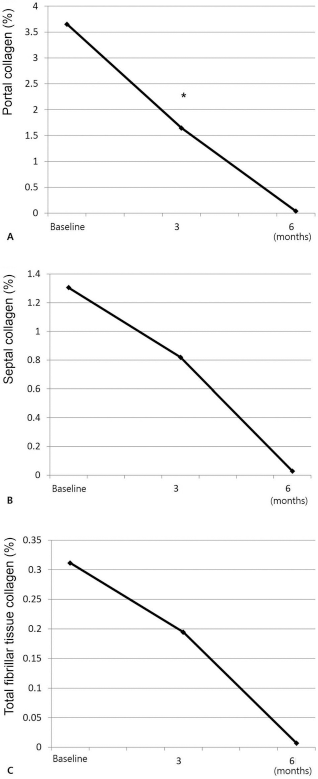
Collagen deposition as determined by a computer-assisted, staining-free method for assessment of liver fibrosis. (A) Percentage portal collagen was significantly lower at 3 months. (B) Septal collagen showed a decreasing tendency over time. (C) Total fibrillar tissue collagen (fibrosis other than portal and septal fibrosis) percentage also showed a decreasing tendency over time. *p < 0.05.
Long-Term Clinical Outcomes
Patients were followed up for a median of 66 months after ABMI (range: 2–113 months). Five patients (26.3%) underwent LT at 5–39 months, five patients (26.3%) died, and three patients (15.3%) were lost to follow-up. A survival curve of patients who did not undergo LT or die is shown in Figure 4A. The median duration of survival without LT was 48 months. Five patients died due to pneumonia (n = 3), lymphoma (n = 1), and spontaneous bacterial peritonitis (n = 1). Three patients (15.8%) were lost to follow-up at 22, 31, and 32 months; these patients did not exhibit deterioration of liver function at their final follow-up.

Survival curve without liver transplantation (LT) and cumulative rate of hepatocellular carcinoma (HCC) development. (A) The median survival duration without LT was 48 months. (B) In HCC-naive patients, the cumulative rate of HCC development at 3 and 5 years was 23.1% and 35.9%, respectively.
HCC developed in five patients (26.3%) after ABMI. One patient had previously undergone HCC resection, while the others developed HCC at 16, 17, 18, and 56 months after ABMI. Four patients underwent successful nonsurgical treatment, and one received elective LT. In HCC-naive patients, the cumulative incidence of HCC at 3 and 5 years was 23.1% and 35.9%, respectively (Fig. 4B). The patient with HCC recurrence exhibited improved liver function but was diagnosed with lymphoma at 49 months. The lymphoma was thought to be hepatitis B virus (HBV)-related lymphoproliferative disease and led to death of the patient.
In one patient who showed improvement to CP class A, cancer of the sigmoid colon was found during routine colonoscopy at 18 months after ABMI. This was removed by endoscopic mucosal resection, and no further recurrence or hepatic function deterioration was noted.
Discussion
The findings of this work suggest that ABMI for decompensated LC could improve liver function and decrease the collagen level in liver tissue transiently and inconspicuously, although LC itself was not resolved. Some patients successfully bridged to LT, and others sustained an improved state without significant adverse events related to ABMI. However, some patients developed infection or HCC after >5 years.
We evaluated the effects of ABMI using various parameters, while other studies using BMCs or MSCs for LC have focused on blood test results. Functional changes were assessed by determining serum levels of albumin and CP class. Pathologic and computer-assisted evaluation of fibrosis and liver tissue were performed. Regenerative changes were assessed by measuring liver volume. The patients showed improvement in terms of biochemical parameters, CP class, and liver regeneration, as indicated by an increased liver volume.
A recent meta-analysis of autologous BM transplantation in decompensated livers showed a benefit after 1 year 27 . Previous studies of cell therapy have reported only short-term effects because long-term monitoring of subjects was not possible. In the early stage of cell therapy research, long-term safety was a matter of concern because, in contrast to chemotherapeutic agents, injected stem cells have long half-lives, the possible ability to transdifferentiate and/or repopulate, and no modulating manner after injected. While use of autologous cells prevents adverse immunologic reactions, their effects on cancer development are unclear. Therefore, maintenance of the therapeutic effects of cell therapy and its influence on cancer development are unresolved issues.
In this cohort, three patients with HCC underwent successful treatment before ABMI. These patients were included in this study because they had no recurrence of HCC for 2 years before ABMI and showed no HCC on screening MRI. Among these three patients, one experienced HCC recurrence at 10 months after ABMI. This patient underwent successful HCC treatment; however, lymphoma developed 49 months after ABMI. A hematologist speculated that the lymphoma was likely related to HBV infection, as reported previously 28 . However, it is also possible that ABMI contributed to the development of lymphoma. Because lymphoproliferative disease usually progresses rapidly, the 4 years between ABMI and the lymphoma diagnosis means that a causal relationship is possible but unlikely. Further research is warranted to resolve this issue. HCC did not recur in the other two patients with HCC before ABMI.
Other than the patient discussed above, HCC was newly diagnosed in four patients after ABMI. Because they had undergone regular evaluations, HCC was found at an early stage and treated successfully. Only one patient considered LT for treatment of HCC; the others elected nonsurgical treatments. The 5-year cumulative risk of HCC has been reported to be 15% in compensated HBV-related LC in a high-endemic area 29 , and patients with a more advanced CP class had a higher risk of HCC 30 . The rate of newly developed HCC in these patients (4/16, 25%) is comparable with that reported previously. However, the relatively high incidence of HCC within 2 years after ABMI warrants further study.
Infection was the most frequent cause of death in our patients. Two patients with improved liver function expired from uncontrolled pneumonia, and two patients without improvement died due to pneumonia and spontaneous bacterial peritonitis. To the best of our knowledge, no previous study has evaluated the frequency of infections after cell therapy in LC patients.
The limitations of this study were its single-arm design and inclusion of a small population. However, this study was started as an exploratory pilot trial in its early days of cell therapy. From the result of this trial, a randomized controlled trial is underway and is expected to provide more confirmative evidence in terms of therapeutic effects and influence on cancer development.
Our results suggest that ABMI for decompensated LC could improve liver function and volume over the short term. Over the long term, while some patients maintained improved liver function, HCC developed in other patients. Further studies of long-term follow-up cohorts after cell therapy for LC are warranted.
Footnotes
Acknowledgment
The authors thank K. J. Song for statistical advice. This study was supported by a grant from the Korean Health Technology R&D project, Ministry of Health & Welfare, Republic of Korea (Nos. A090292 and A050021). The authors declare no conflicts of interest.