
Abstract
BACKGROUND:
New technologies have made rapid advances in the field of assistive technologies (AT), with Extended Reality (XR) offering promising results in supporting people with mild intellectual disabilities (ID). Yet, the design and goals of programs for people with mild ID may differ from those for people with moderate and severe ID. It remains unclear how XR technologies are used for people with moderate to severe ID.
OBJECTIVE:
The study we present in this paper aimed to explore what is known from the existing scientific literature about XR-based interventions for supporting people with moderate to severe intellectual disabilities, including the features of XR content and technology that is used and factors that may impact implementation.
METHODS:
We conducted a scoping review, searching Cinahl, PubMed, LibSearch, and Google Scholar based on inclusion and exclusion criteria ensuring the focus on XR and moderate to severe ID. We adopted a qualitative content analysis approach to review the papers resulting from the search.
RESULTS:
In total, we included 16 papers in the review. Most of these focused on XR-based interventions to improve specific skills, such as navigation and daily living skills, in order to increase autonomy and independence. We found a large variety in the content and technology used in these interventions as well as in factors that the authors found to affect the implementation. These factors concern characteristics of users, of caregivers or facilitators, and of the XR environments and systems. The majority of the papers reported studies with small sample sizes, and lacked control groups and follow-up periods to measure long-term effects of XR.
CONCLUSIONS:
The use of XR for people with moderate to severe ID is an emerging field. Although many authors of the reviewed studies do acknowledge the potential of XR, further evidence is needed. Future research might explore the potential of XR as leisure activity, and might study in detail how features of the XR environment impact behaviour to inform professionals about how to approach their use of XR in order to meet the needs and preferences of people with moderate and severe ID.
Keywords
Introduction
According to the United Nations Convention on the Rights of Persons with Disabilities access to assistive technology (AT) is a human right [1]. An assistive technology device is any product (including devices, equipment, instruments, and software) that is either specifically designed and manufactured or commonly available, and whose primary purpose is to maintain or enhance a person’s functioning and independence, and thereby promote their well-being [2, 3]. For people with intellectual disabilities (ID) assistive technology has the potential to facilitate the acquisition of new skills, improve existing skills, and reduce the impact of disabilities on daily functioning [4]. In addition, assistive technology may reduce the need for formal health and support services, long-term care and caregiver work, and promote community living and inclusion [3, 5].
In recent years, extensive development of new technologies has led to rapid advances in AT, with increased interest in Extended Reality as a supportive tool for people with ID. Extended Reality (XR) is an umbrella term that includes Virtual Reality (VR), Augmented Reality (AR), and Mixed Reality (MR) technologies [6]. VR is a computer-generated experience which enables the user to interact with objects and/or characters within a simulated scenario [7]. Compared to traditional therapeutic or educational materials, VR offers the possibility of creating a wide range of realistic environments that can be adapted to fit specific therapeutic needs, such as training of cognitive, motor, and social functions [8, 9, 10, 11]. In addition, VR provides individuals with ID safe access to real-life situations that they might not be able to access routinely due to physical or cognitive limitations (e.g. leisure activities) [12]. AR is a technology which allows computer generated virtual features (e.g. sounds, images) to overlay physical objects in real time [13]. Unlike VR, where the user is completely immersed in a virtual environment, AR allows the user to interact with the virtual features in the real world [13]. As an example, Navigation Heads Up Display is an AR navigation app which uses the camera on mobile devices to produce live views of the physical world and add information for the destination location, such as its name and remaining distance [14]. AR has been shown to be effective in assisting individuals with ID to learn independent living skills, such as checking food labels for possible food allergens or navigating unfamiliar locations [15, 16, 17, 18]. Finally, MR combines elements of both AR and VR, and allows the users to interact with an artificial environment where the surrounding physical space, realistic renderings of physical materials, and digital objects, all coexist and communicate in real time [6, 19].
Several researchers have employed XR technologies specifically for people with ID and showed promising results. Such studies focussed on the acquisition and training of skills that are essential for activities of daily living, such as mathematical and logic skills that are useful for preparing shopping lists and supermarket visits [20] or using an ATM in a simulator [21]. However, these studies involved users with mild forms of ID. The level of severity of ID can be classified into four levels: mild, moderate, severe and profound [22], with mild severity representing the largest group of people with ID. XR-based interventions for people with mild ID, such as the examples described above, may not necessarily be suitable or effective for people with moderate and severe ID. Individuals with moderate and severe ID might, for instance, require more support to understand the instructions and complete the tasks. As little is known about how XR is used for people with more severe forms of ID, we aimed to review existing XR-based interventions for this particular user group. More specifically, we mapped the objectives of existing XR-based interventions for people with moderate to severe ID, the features of the XR content and technology that was used in such interventions, and the factors that may have affected the implementation of those interventions. To our knowledge, the scoping review conducted by Nabors and colleagues [23] is the only overview of XR-based interventions for people with ID. Yet this review only included studies employing VR, most of which included only participants with mild ID. Our scoping review explored what is known about the use of all forms of XR to support people with moderate to severe ID.
Methods
For our scoping review, we followed the methodological framework developed by Arksey and O’Malley [24]. This framework involves five steps for data gathering: (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies; (4) charting the data; (5) collating, summarizing and reporting the results. We adopted this approach because of the broad nature of our review objectives and focus. Our goal was to map the existing research on the selected topic and to identify knowledge gaps and as suggested by Peterson et al. [25] we did not want to make any prior assumptions about the scope, range, and key findings of the studies we reviewed.
Search string.
Based on previous research experience and the expertise of the research team, we formulated the following research question: What is known from the existing literature about the use of extended reality (XR) in supporting people with moderate to severe intellectual disabilities (ID)? Specifically, we were interested in (1) the objectives of the XR-based interventions aimed, (2) features of the XR content and technology used, (3) factors that were reported to affect the implementation of the intervention.
Identifying relevant studies
We conducted the initial search for literature in January 2021 using the following search formula: intellectual disability AND virtual reality OR augmented reality OR mixed reality. We used both free-text search terms and MESH headings to search the following electronic databases: Cinahl, PubMed, LibSearch, and Google Scholar (see Fig. 1 Search String). We limited our search to English papers published between 2010 and 2021. Furthermore we manually screened the reference lists of the papers that we found to identify other potential key publications that we had missed. The retrieval process was iterative, and we redefined the search strategy more than once to ensure full coverage of the literature [26].
Selecting studies
We imported the publications resulting from our search into Endnote and removed duplicated records. Subsequently, we selected relevant publications in three stages. Firstly, we screened the titles of the publications, after which we reviewed the abstracts and full texts. We included any papers without an available abstract directly in the full-text review stage. Two reviewers (PLM and RD) discussed the results until consensus was reached.
To be eligible for review, articles had to meet the following criteria: (a) inclusion of individuals with moderate to severe ID; b) use of XR; (c) reporting of empirical data. We did not apply limitations for age or gender. Due to the high comorbidity of intellectual disability with other disorders [22], we also included papers reporting studies that included participants with other disorders such as Down Syndrome or Autism Spectrum Disorder in addition to a moderate or severe ID. Additionally, since the majority of studies included participants with different severity levels of ID, we only selected papers about studies that included at least one participant with moderate or severe ID. We excluded any articles from our review when they (a) did not include participants with moderate or severe ID, (b) included only participants having acquired brain injury; (c) did not use XR; (c) did not report empirical data.
Charting the data
We developed a data-charting form to map the key findings as well as the following descriptive variables reported in the papers: author names, year of publication, study design, research aim(s), target population, XR system used, the setting and the country where the intervention took place, and outcome measures. Two reviewers (PLM and AV) pre-extracted seven randomly selected articles to determine the degree of congruency between the results. Finally, PLM charted the data, discussed the results with the research team and iteratively updated the data-charting.
Collating, summarizing and reporting results
One of the researchers (PLM) initially performed a content analysis while focussing on the objectives of the reported interventions, the features of the XR content and technology that were used, any factors reported by the authors that may have affected implementation, and lessons learned. Results were then discussed and reported with two other researchers (RD and KS) until consensus was reached.
Results
The initial search resulted in 1281 hits, and after removing duplicates 1217 remained. Overall, we considered 107 articles to be potentially eligible for inclusion in our review. After full assessment, we excluded 91 papers, resulting in the inclusion of 16 papers in the final review (see Fig. 2).
Study selection process.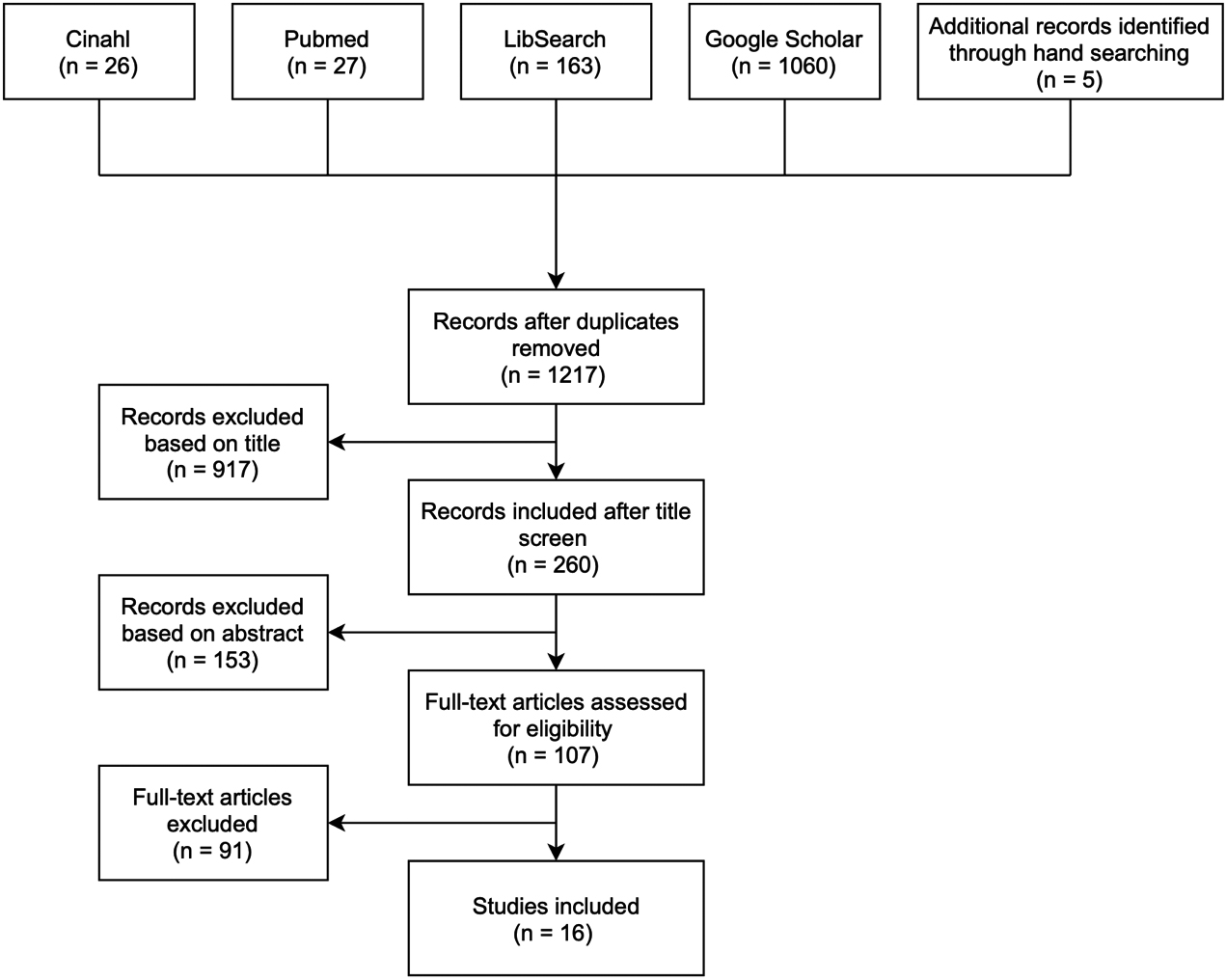
Of the 16 included papers, ten were published in or after 2015. Seven were conducted in Europe, six in Asia and three in the USA. Five out of the 16 papers presented pretest-posttest trials, four involved qualitative studies, and three were multiple-baseline studies. Twelve out of the 16 studies presented assessed the effectiveness of a technology-based intervention aiming for the improvement of specific skills or abilities (e.g. daily living skills). The remaining four papers described studies aimed at exploring the usability, acceptability, likeability, satisfaction, or potential utility of the technology chosen for the target group.
The sample sizes of the studies reported varied between three and 92 participants. In terms of the age ranges of participants, ten studies focused on adults (18 years and older), four studies focused on children (younger than 18), and two studies had a mixed age sample of participants. Nine out of the 16 studies recruited participants with mild-to-moderate ID, while four studies had participants with moderate to severe ID. Three studies included only participants with severe ID; and one study included participants with the entire range of mild to severe ID. Regarding the technologies used in the studies, nine studies used VR, five studies used AR, and two studies used MR. The studies covered a wide range of settings, including community settings (i.e. schools, university campuses, social centres, or augmented reality cinemas), laboratories or research centres and facilities for people with disabilities (i.e. residential care facilities).
In terms of outcome measures, nine studies assessed individuals’ performance scores on the trained tasks (e.g. the number of independent waypoint decisions made when traveling to a new destination [17]). Six studies used self-report questionnaires assessing experiential factors such as fun and satisfaction. Six studies used ethnographic measures such as observations or interviews. Finally, two studies used objective physical measures to assess muscle strength and agility performance [27] and resting pulse [28] (see Table 1 for a full overview of all measurement instruments used in the 16 studies).
In this section we provide an overview of the main objectives of the XR-interventions reported in the 16 papers included in our scoping review. Most of these interventions focused on specific skills domains. Five domains stood out from our scoping review: activities of daily living, navigation, academic development. In almost all of the interventions discussed below, XR-based training was the main activity. Only in 4 studies, XR-based activities were implemented in combination
Study characteristics
Study characteristics
with other traditional activities. Lin et al. [27], for example, combined physical exercises on a treadmill with a VR-based exercise program.
Activities of daily living was the main domain of focus in three studies [18, 29, 30]. More specifically, Bridges et al. [18] examined the effects of AR apps addressing specific household tasks such as ironing, making your bed, and setting an alarm clock. Panerai et al. [29] tested the feasibility of VR apps for remote home-based rehabilitation aimed at teaching how to provide personal information taking medication at appropriate times packing a suitcase and grocery shopping. Finally, Aruanno [30] investigated the acceptability, usability, and satisfaction of a wearable MR device aimed at teaching people with neurodevelopmental disorders to perform simple domestic tasks such as garbage collection.
Four studies tackled abilities in the navigation domain [17, 31, 32, 33]. N’Kaoua et al. [20] explored the spatial deficits associated with ID and evaluated the effectiveness of various types of navigational aids in a virtual environment (i.e. signifying landmarks, such as a flashing yellow bench using arrows, or an elevated view). De la Torre et al. [33] tested the efficacy of a VR-based intervention aimed at enhancing visuospatial orientation skills of people with severe disabilities, that is, the ability to find their way and locate specific goals (e.g., find a specific room). Smith et al. [17] examined the effects of using an AR app to improve navigation skills among three students with ID, and finally, Cherix et al. [9] explored the usability of a VR immersive headset as a learning tool aimed at increasing the ability to cross roads using pedestrian crossings among young people with ID.
Three studies focused on academic development and skills in the special education context [34, 35, 36]. More specifically, Cakir et al. [34] explored the potential contribution of AR teaching materials for improving attention spans of children with special education needs. Pareto et al. [35] investigated the utility of a game to improve mathematical literacy among children with ID and the potential of an AR version of the game in enhancing game experience and learning. And finally, Byrne et al. [36] explored the impact of a VR learning programme designed for students with severe ID, for increasing their self-awareness, social and communication abilities, and levels of class participation.
The remaining studies addressed job skills [37], physical abilities or fitness [27, 28] time perception [7], and providing health care information [38].
Regarding the technology employed in the studies we reviewed, both custom-made and commercially available XR systems were used. The most common devices used for the XR experience included projectors [28, 32, 33, 35, 36], computer or television screens [37, 38, 39] handheld devices [37, 38, 39], head-mounted devices [7, 30, 31], and a gaming console [27]. Finally, one study used a combination of tablets and projection devices [34].
Regarding the content used in the XR interventions, four studies presented a replication of a realistic scenario in a VR environment [31, 32, 33, 38]. Cherix et al. [31] used a scene showing a sidewalk and a two-way street surrounded by buildings. Participants had to cross the road by using the available pedestrian crossings. In the scenario, five different parameters could be modified: the weather, the probability that a vehicle stops, the time a vehicle waits for the user to start crossing once stopped, the travel speed of the player, and the presence of visual and audio feedback in case of a collision between the participants and a vehicle. Similarly, N’Kaoua et al. [32] used a scene showing the area surrounding a hospital in Bordeaux (France). De la Torre et al. [33] showed a realistic rendering of the ground floor of an existing care facility. Finally, the virtual environment used in the study conducted by Hall et al. [38] consisted of a stylized hospital building giving access to different rooms. The hospital scenario incorporated a nurse who offered participants a tour of the hospital.
Another common content-related practice we found in three of the studies we reviewed [7] was the use of a diversity of realistic scenarios in which users had to complete different tasks that resembled real-life tasks. For instance, in the study conducted by Panerai et al. [29], participants had to place clothes in a suitcase, whereas in the study conducted by Eden [7], participants had to arrange different episodes belonging to the same scenario (e.g. baking a cake) in the correct order.
Also related to XR content, in two studies, games were used to stimulate participants to practice certain skills [27, 28]. Both studies involved training of physical skills. In the study conducted by Lin et al. [27], participants could choose between 15 different virtual games, such as boxing, or playing golf, table tennis, and frisbee.
Specifically regarding content in AR-based interventions in two studies researchers used AR tags (i.e. visual cues triggering the display of virtual information) [18, 39]. In the study conducted by Bridges et al. [18], users used laminated cars as AR tags to activate videos containing step-by-step instructions to complete daily tasks. Chang et al. [39], participants had to move AR tags representing food pictures on an LCD screen in the correct order to prepare a meal. In addition, in one study [35] users moved physical cubes containing sensors which are connected to a virtual world to select a corresponding card on the screen. Cakir et al. [34] explored the use of AR in creating teaching material aimed at teaching students about basic real life concepts, such as traffic lights and seasons; whereas Smith et al. [17] examined the use of an AR application in helping users to travel to unknown places. More specifically, they used a mobile application which combines Google Maps with AR features to enable real-time navigation prompts to users.
Finally, several papers reported on features of MR applications. In the study conducted by Aruanno et al. [30], the authors explored the use of HoloLearn, a MR application using HoloLens technology. HoloLens is a device for wearable MR which enables the user to interact with holograms that are placed in the real environment [30]. Aruanno et al. [30] tested an activity aiming to teach participants how to collect garbage properly by means of different holographic bins and some pieces of trash. Walker et al. [37] conducted their research in a laboratory that combines a physical space with simulated people. In this environment, participants were presented with an avatar seated at a desk in the virtual office to practice a job interview.
Factors that impact implementation
This section provides an overview of the practical factors and issues related to the implementation of XR for people with ID that were reported by the authors of the papers we reviewed. We divided these factors in three categories: (1) factors related to users with moderate to severe ID, (2) factors related to caregivers/facilitators, and (3) factors related to the XR environment and system.
User-related factors were mentioned in 11 studies, with motivation being the factor most frequently cited by authors. In six papers the authors specifically reported that they selected participants based on their interest and willingness to participate [17, 18, 27, 29, 33, 39], while two papers reported difficulties with implementing the XR-based intervention because users refused to complete the session [28, 31]. In addition to motivation, four studies observed that cognition played an important role in understanding the goal of the XR-application as well as the instructions [7, 30, 31, 38], which suggest that the severity of the cognitive impairment should be considered in both XR-based intervention development and implementation. As a result of the cognitive impairment, these studies also stressed the importance of mediation (i.e. help needed in completing a certain task) and caregiver support in capturing users’ attention during a session [7, 30, 31, 38]. Finally, and perhaps contrary to what was to be expected, seven studies included a familiarization or training phase in which participants practiced using the XR system and explicitly reported that no major simulator sickness was experienced [18, 27, 29, 31, 32, 33, 39]. Simulator sickness is a syndrome similar to motion sickness, often experienced during simulator or another virtual reality (VR) exposure [40].
In 11 of the articles, authors stressed the importance of involving caregivers or facilitators to support, guide, and encourage participants while using the XR-systems. Four papers mentioned the inclusion of health behaviour experts (i.e. a child psychiatrist, a psychologist, a neuropsychologist) in the design process [18, 29, 30, 31]; whereas three studies involved a technical assistant to assure proper functioning of the XR system [28, 31, 37], and instruct participants on how to use the tablets [29]. Diving deeper into factors related to this supporting role of caregivers/facilitators, Byrne et al. [36] mentioned a positive therapeutic alliance between a therapist and users as an essential element for the learning experience. Hall et al. [40] speculated on how different facilitation styles might have affected the participants’ experience. Specifically, these authors suggested that the facilitator should not intervene too much since they observed that some participants lost interest or confidence when control was taken away. Instead, they argue that assertive facilitation is the ideal facilitation approach since it gives users access to all opportunities in the virtual environments, while negotiated methods are used to determine what they will do in the environment, and how much assistance they need and want. Finally, in two studies, caregivers were not provided with any training about the VR system in order to determine whether the program could be implemented by direct care staff supervised by a therapist, thus reducing the costs associated with such intervention [27, 28].
Factors related to the XR-system that were reported to affect implementation mostly addressed features that influenced the feasibility and acceptability of the XR-system. Such factors included the heaviness of the headset, motion sickness triggered by the virtual environment, and features related to the scenario that irritated some participants [31]. Aruanno et al. [30] encountered difficulties related to the interaction mechanisms of the HoloLearn system (i.e. gaze and air-tap), which proved to be too complex for people with severe ID. Hall et al. [38] noted that only four participants looked like their avatar, making it difficult to assess whether this affected identification with it. However, they did observe that full identification with the avatar did not seem to be highly important as only a few participants referred to it as “I”.
Outcomes and lessons learned
In this section, we describe the main effects of the XR-interventions that were included in this scoping review. Although many authors of the studies emphasise the potential of XR-interventions for people with moderate to severe ID definitive conclusions about their interventions’ effects cannot be drawn due to several methodological reasons. Sample sizes were small; control groups were often missing, and long term effects were not measured. However, several authors shared important and relevant lessons learned in their papers, which we want to reflect on here as well.
Four of the selected studies described what worked well and what did not work, and provided lessons learned concerning the XR systems’ interfaces and design [30, 31, 33, 38]. Giving the heterogeneity of this population, one of the main recommendations based on these studies is to create scenarios with multiple configuration options allowing for adaptation to the specific needs of each individual user [30, 31]. In addition, due to the wide heterogeneity of the target population in terms of skills and needs it is considered important to incorporate people with ID in the design process of XR systems and content [31]. Moreover, some authors emphasized the importance of simplifying the stimulation settings and adapting the interface to educators and professionals in order to facilitate the application use [30, 31].
In two studies researchers noticed that visual similarities between the virtual world and the real world seemed to facilitate transfer of learning between contexts [33] and enhance enjoyment [38]. Likewise, Cherix et al. [31] emphasized that game elements (e.g. scores, badges, etc.) that do not exist in the real world may also represent an obstacle in this sense, indicating that realistic environments may be more effective when applied to VR interventions. In addition, the presence of a human-like “other” might contribute to the user experience. Additionally, even though an animated virtual assistant seemed effective at attracting the user’s attention and engaging them, it did not seem to have any functional benefit when the disability severity is high [30].
Finally, Aruanno et al. [30] provided two different solutions to mitigate the difficulties faced by individuals with severe ID when interacting with complex interaction mechanisms (i.e. gaze and air-tap). The first solution consists of training users to use the interaction mechanisms over a long period of time, whereas the second solution involves changes in the device such as replacing the default white cursor with a purple one which is more visible and intuitive and using a physical button instead of the air-tap interaction mechanism. Finally, Cherix et al. [9] recommended reducing the speed of the movements and avoiding re-creating head movements in VR environments to prevent motion sickness.
Discussion
In this scoping review, we explored scientific literature pertaining to the use of XR for people with moderate to severe ID. The use of XR interventions appears to be a promising but still emerging field, with most of the studies we found being exploratory in nature. The majority of the studies had small sample sizes, no control groups, and no follow-up periods to measure long-term effects, which makes it difficult to draw conclusions about the effectiveness of XR interventions. In addition, no cost-effectiveness studies have been conducted. Most studies included people with mild to moderate ID, and only a small part of the studies addressed XR-based interventions for people with severe ID. In terms of technology used, more than half of the studies used VR, and only 2 studies used MR. Most studies included self-reported questionnaires, observations, interviews or task performance measures to assess changes in behaviour or skill performance. No study included physiological measurements. Overall, the analysis focused on the objectives of the interventions, features of the XR content and technology used, and factors that influenced the intervention. Additionally, we included outcomes and lessons learned when shared by the authors.
The majority of the selected studies focused on exploring XR-based interventions to increase specific skills among people with ID, such as navigation skills and daily living skills, in order to increase their autonomy and independence. This is not surprising since autonomy and participation are considered important needs for people with ID [41, 42]. However autonomy and participation also relate to leisure activities. Substantial evidence suggests that participation in leisure activities promotes subjective well-being and improves the quality of life of people with ID [43, 44]. Additionally, previous studies showed the potential of technology in teaching leisure skills to people with intellectual disabilities [45, 46]. For example, Lancioni et al. [45] explored the potential of a smartphone-aided program to support independent access to different leisure content (e.g. Mr. Bean, travel adventures, a specific singer’s songs, and kitchen recipes) in seven individuals with moderate ID, with promising results. Yet, we found no study that explored the use of XR in teaching leisure activities to individuals with ID, or as a potential leisure activity itself. Surprisingly, none of the XR-based interventions focused on relaxation or well-being. Some studies did, however, show that the use of visually appealing scenes in a VR environment, such as nature scenes, can improve mood and reduce negative affect [47, 48], thus contributing to a use’s emotional well-being. Similarly, nature-based sounds have been shown to have intrinsic relaxing properties [49]. Further research is needed to understand how XR can be used to promote relaxation, subjective well-being and leisure among users with ID.
Regarding XR-content, VR systems, in particular, are recognised for their ability to elicit behavioural and emotional responses that lead to psychologically valuable changes [44, 50]. However, the studies selected for our scoping review did not report specifically on which content triggers specific behavioural and emotional responses. To better understand which content is more effective in triggering the desired responses, future research may include implicit measures that allow for the detection of emotional and psychophysiological responses. Inspirational examples include the work of Higuera-Trujillo et al. [51], who used electrodermal activity (EDA) to compare the psychological and physiological responses evoked by real world and VR scenarios with different immersion levels and the work of Marín-Morales et al. [52], who used electroencephalography (EEG) and electrocardiography (ECG) recording to detect affective states elicited by immersive virtual environments. However XR interventions also come with certain risks that may be particularly important for people with ID. Behr et al. [53], for example, stress that it is important to consider cognitive, emotional, or behavioural disturbances that may occur following re-entry into the real world after a VR experience. Of the studies included in our review, only the study by Cherix et al. [10] reported information related to this topic as one participant in this study reported distressing memories of the experiment due to a collision with a vehicle in the virtual environment [10]. Nevertheless, none of the included articles provide information on how professionals dealt with possible risks posed by XR content, which can be considered a blind spot in the research. Therefore, further research on the possible adverse effects of XR content on users, as well as and guidelines indicating how to deal with such possible side effects may be necessary to protect individuals from potential harm [54, 55].
In developing XR-based interventions, and more broadly assistive technologies for individuals with ID, O’Brolcháin [56] emphasizes the importance of individuals making choices according to their own individual preferences. In line with this, we found that two studies identified the need to create scenarios with multiple configurations, adapted to the specific needs of each individual [30, 31]. In addition, Cherix et al. [31] highlighted the importance of involving people with ID in the conception phase of new XR interventions. Incorporating people with ID early in the design process ensures that their needs, desires and priorities are known and can be taken into account [57]. However, of the studies selected, only Hall et al. [38] actually included people with ID in the design process. More research is needed on how to tailor the XR-application to individual needs and preferences, as well as on how to involve people with ID in the design process.
We found that XR-based interventions can be influenced by factors related to the user, to caregivers/facilitators, and to XR content and system. Based on the NASSS framework for analysing and evaluating technology programmes in health and social care [58], we found that most of the factors we identified were related to the nature of users’ condition, the technology used, and the adopter system. However, it was not possible to extract any information related to the organisation, its capacity to innovate, the nature of the decisions made regarding adoption and funding, and the wider system, including the policy context. In addition, no information could be extracted regarding adaptation over time and organisational resilience. Although this can be explained by the current state of art of XR, as it is not yet clear whether its use does in fact have positive effects, these aspects too require more research.
Our review has several strengths. First, we used a comprehensive search strategy across multiple databases, including grey literature (i.e. Google Scholar) to minimise the risk of having missed relevant articles. In addition, the process of including articles and extracting data was interactive in nature, to assure full coverage of our research questions. However, the results of the review may also have certain limitation. First, the process of data-charting was done by only one researcher, which may have increased a certain bias. Secondly, the search was restricted to a combination of key words based on preliminary but broad literature exploration. Yet, by including grey literature and reference checking we expect to have minimized this potential shortcoming.
Conclusion and implications
The use of XR for people with moderate-to-severe ID appears to be a relatively new field, with most studies involving small sample sizes. The studies selected focused mainly on interventions aimed at increasing the autonomy and independence of people with ID. All studies mentioned factors influencing the implementation of XR-based interventions, including the user, the XR system and the professionals involved. Among these, user’s motivation and cognition were the most cited. Based on an analysis of the literature, four areas for further research and implementation in practice were identified. First, more studies with larger sample sizes are needed to gather insight into the (cost)effectiveness of XR interventions. Second, more research is needed on how XR is meaningful as a potential leisure activity. Third, future research should consider the potential risks posed by XR content and provide guidelines for managing potential side effects in order to protect individuals from harm. Lastly, practice could benefit from more knowledge on how to include people with ID in the design of XR interventions, and on how XR applications can be tailored to individual needs and preferences.
Author contributions
CONCEPTION: Patricia Laura Maran and Ramon Daniëls.
PERFORMANCE OF WORK: Patricia Laura Maran and Ramon Daniëls.
INTERPRETATION OR ANALYSIS OF DATA: Patricia Laura Maran, Ramon Daniëls and Karin Slegers.
PREPARATION OF THE MANUSCRIPT: Patricia Laura Maran, Ramon Daniëls and Karin Slegers.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Patricia Laura Maran, Karin Slegers and Ramon Daniëls.
SUPERVISION: Ramon Daniëls.
Ethical considerations
This study, as a scoping review, is exempt from Institutional Review Board approval.
Footnotes
Acknowledgments
We would like to thank Ashley Vijgen for supporting the data extraction process.
Conflict of interest
The authors have no conflicts of interest to report.