
Abstract
Background
Extended reality is increasingly used for rehabilitation after acquired brain injury, offering benefits including improved recovery, reduced length of hospital stay, enhanced self-efficacy, and lower cost. Despite these advantages, XR is rarely implemented in daily rehabilitation practice.
Objective
Outline extended reality for acquired brain injury research, focusing on patient outcomes and experiences to inform scale-up and implementation.
Methods
The Arksey and O’Malley framework and PRISMA-ScR reporting guideline were followed. Studies from 2010 to May 2022 were screened from PubMed, Embase, Cochrane, CINAHL, and IEEE.
Results
Seventy-five studies met inclusion criteria: 63 on stroke patients, seven on traumatic brain injury, and five on multiple disorders. The extended reality applications focused on assessment to diagnose patient’s condition or therapy intervention, categorized into physical, cognitive, and multipurpose. Most studies used Virtual Reality. A wide range of implementation factors were identified, categorized into patient-related, professional-related, and technology and system-related factors.
Conclusions
Our scoping review offers a comprehensive and multidimensional analysis of research on XR applications for acquired brain injury rehabilitation. While it reports potential and promising outcomes of these applications, larger-scale studies are necessary to substantiate the effectiveness of XR and to better understand the factors influencing its implementation in daily practice.
Keywords
Introduction
Acquired brain injury (ABI) is any type of brain damage that occurs after birth and is one of the leading causes of long-term adult disability worldwide. 1 Acquired brain injury includes traumatic brain injury (TBI) and non-traumatic brain injury (non-TBI) such as stroke, infection, and tumor. 2 Effect of ABI pose significant challenges to individuals’ health, well-being, and overall quality of life, leading to various impairments that may affect cognitive, motor, and perceptual functioning. 3 Patients with ABI often require comprehensive rehabilitation interventions, combining psychological and/or neurological with physical therapy (physio-, occupational and/or speech-and-language therapy) and social rehabilitation. 3 The latter is important since participation is considered as the most relevant rehabilitation outcome and fosters engagement in education, employment, leisure, and significant societal roles. 4 Therefore, rehabilitation aims to facilitate maximal independence in daily activities.
Successful neurological rehabilitation requires adherence to essential principles such as repetition, intensity, duration, specificity, and saliency. 5 However, providing this is challenging due to maintaining adherence and engagement in rehabilitation for patients recovering from ABI.6,7 Additionally challenges in healthcare arise with an increase of patients and staff shortage, there is a need to practice without supervision and location independent.4,8–10 Recognizing the limitations of conventional rehabilitation has prompted the introduction of novel, innovative, and promising therapeutic strategies.10,11 An example of an innovative therapeutic strategy is the use of Extended Reality (XR), which is emerging as a promising tool for people with ABI requiring rehabilitation. Extended reality is an umbrella term encompassing Augmented Reality (AR), Virtual Reality (VR), and Mixed Reality (MR). XR is regarded to provide patients with intensive therapy delivered with limited supervision, resulting in faster recovery times, shorter hospital stays, and reduced expenses.10,12 Furthermore, systematic reviews focussing on the efficacy indicating that XR for stroke patients enhances conventional rehabilitation, extending overall therapy duration, and patients perceive virtual tasks more engaging, resulting in boosting their participation and enjoyment in therapy. 10 More explicitly, XR for stroke patients is seen as a highly adaptable and customizable training approach, less reliant on environmental factors, and location-independent, compared to conventional therapeutic rehabilitation settings.13,14
Even though existing evidence presents promising results for using XR in rehabilitation for patients with stroke to achieve desired therapy outcomes, an overview on how XR is used in rehabilitation for patients with ABI is lacking. Therefore, we conducted this scoping review to gain insight into the scope of prior work, used applications, and lessons learned to be able to effectively expand upon existing research.
Methods
In this scoping review we followed the methodology of Arksey and O’Malley, comprising the following five steps: (1) Identifying research question, (2) Identifying relevant studies, (3) Study selection, (4) Charting the data, and (5) Collating, summarizing and reporting the results. 15 Results were reported in line with the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) reporting guideline. 16
Research question
The research questions were identified based on previous research experience and the expertise of the research team. The primary question of this scoping review was to identify what is known in the existing literature on using XR in rehabilitation for patients with ABI? More specific, we were interested in (1) rehabilitation therapy objectives of the reported XR applications, (2) features of XR content and technologies used in the reported XR applications, (3) reported outcomes of the XR applications, and (4) factors that should be considered when implementing XR applications in rehabilitation practice.
Identifying relevant studies
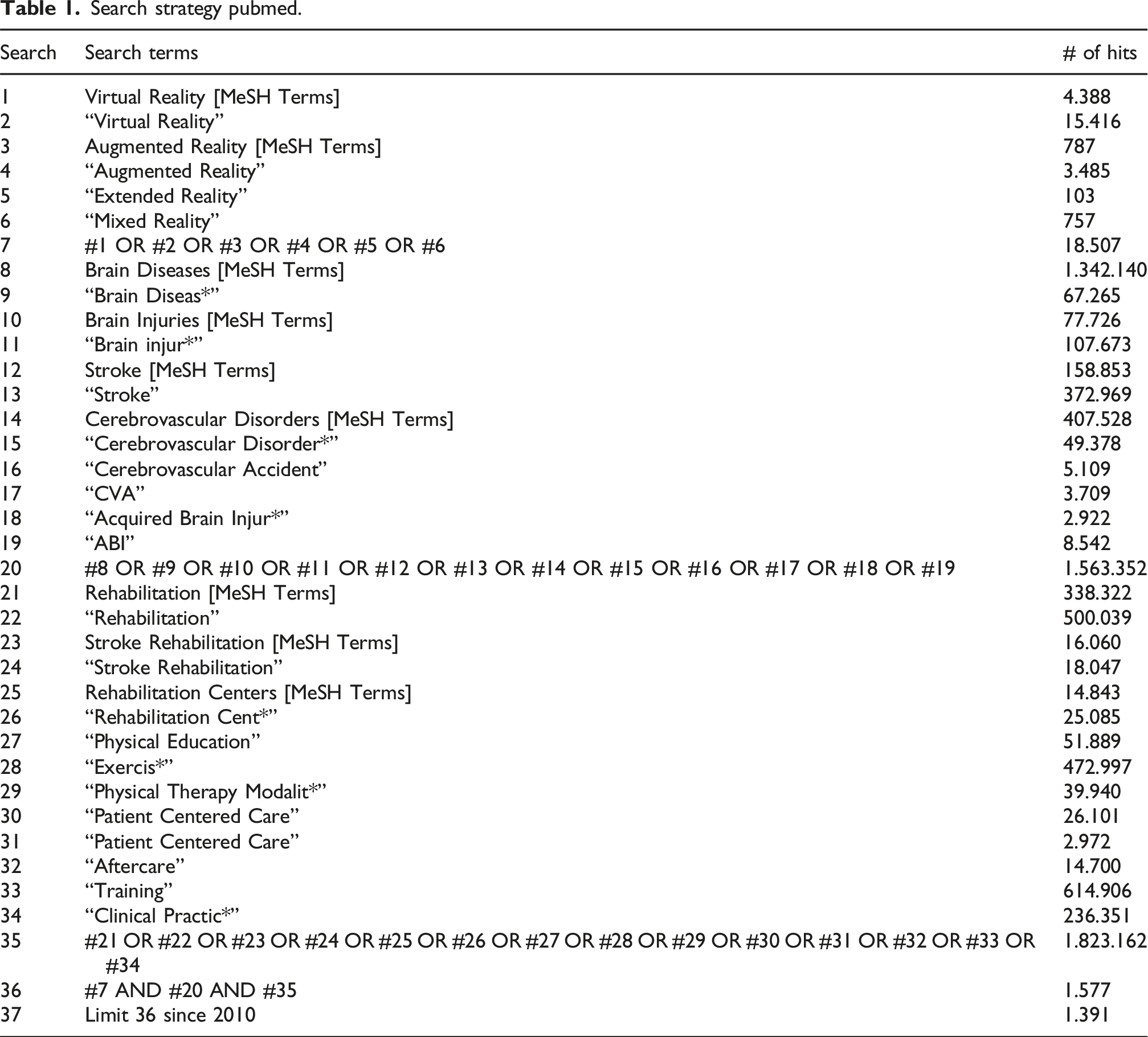
Search strategy pubmed.
Study selection
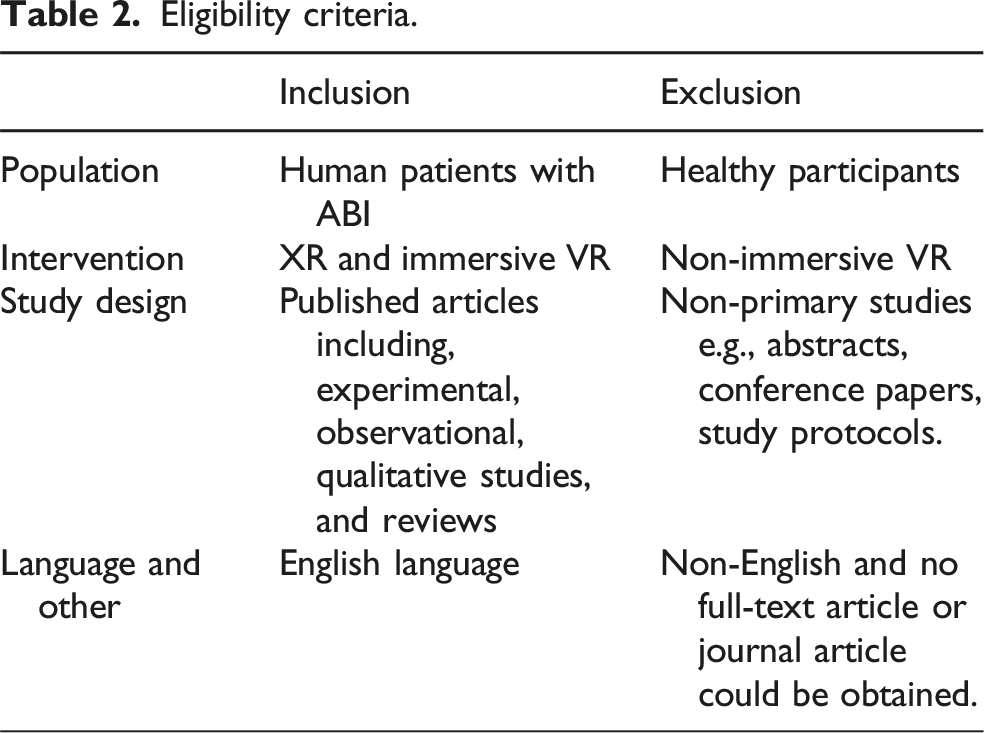
Eligibility criteria.
Charting the data
A data charting form was jointly developed by three researchers (LBS, RvdH, WK) to map the descriptive variables reported in the papers. Data was extracted about study design, participant characteristics, rehabilitation context, features of XR content, details of the used XR technology, objective of the XR applications, scope and outcome of the XR applications, patient experiences, factors for implementation, lessons learned, and conclusions. Independently, the three researchers charted the data, and iteratively refined the data-charting form in Microsoft Excel.
Collating, summarizing and reporting results
First, one of the researchers (LBS) conducted a content analysis based on the data in the extraction table focusing on the objectives of the interventions, features of XR content, outcomes of the XR applications, and factors affecting implementation. Next, results were deliberated and reported in this article in collaboration with all researchers (LBS, RvdH, WK, GH, RD and FV) until consensus was reached.
Results
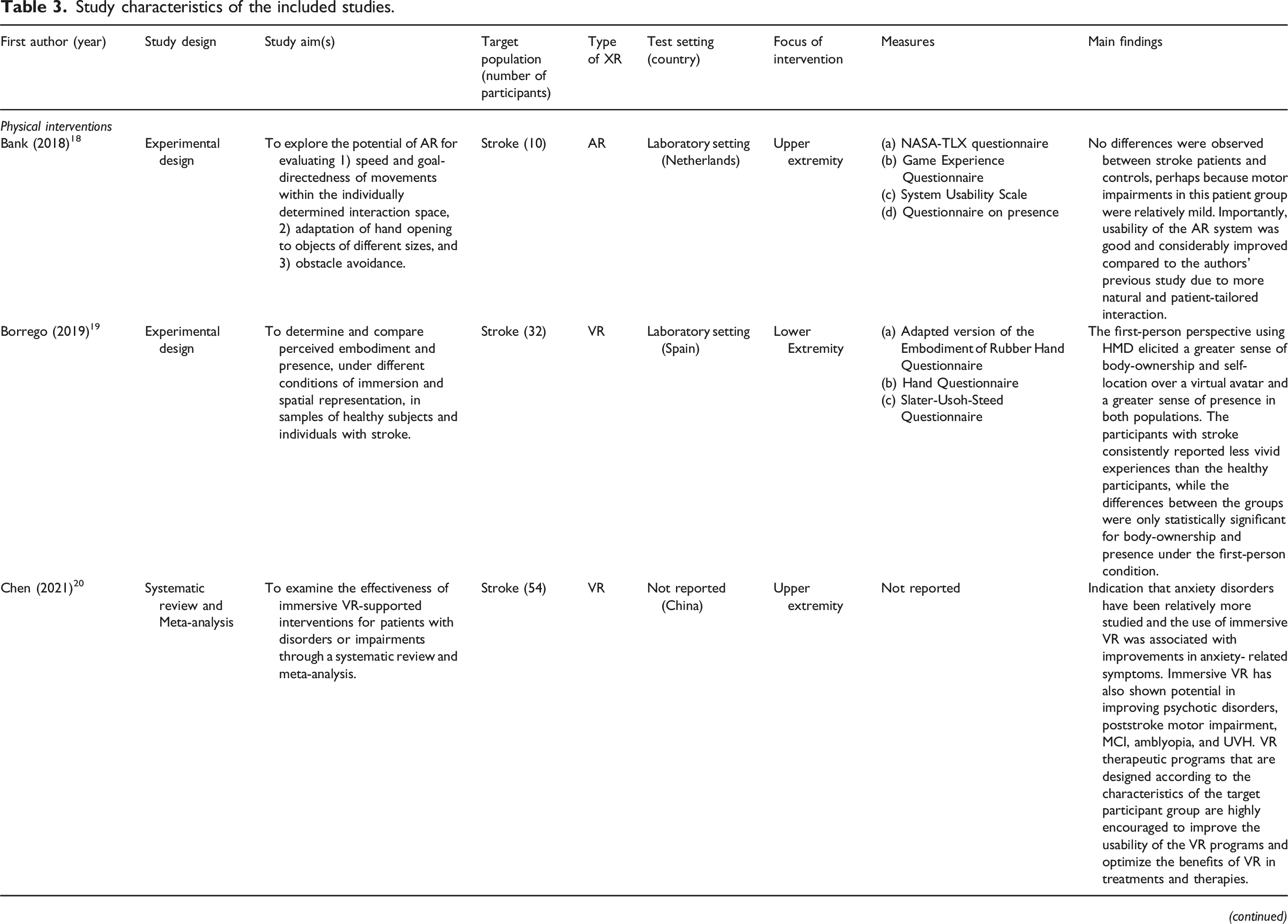
The selection process is depicted in Figure 1. The initial search resulted in 6972 studies, of which 4180 studies remained after removing duplicates. After that, 4020 studies were excluded based on title and abstract, resulting in 160 studies potentially eligible for inclusion. After full text assessment, another 85 studies were excluded resulting in a total of 75 included studies. An overview of these studies and their characteristics can be found in Table 3. Selection process. Study characteristics of the included studies.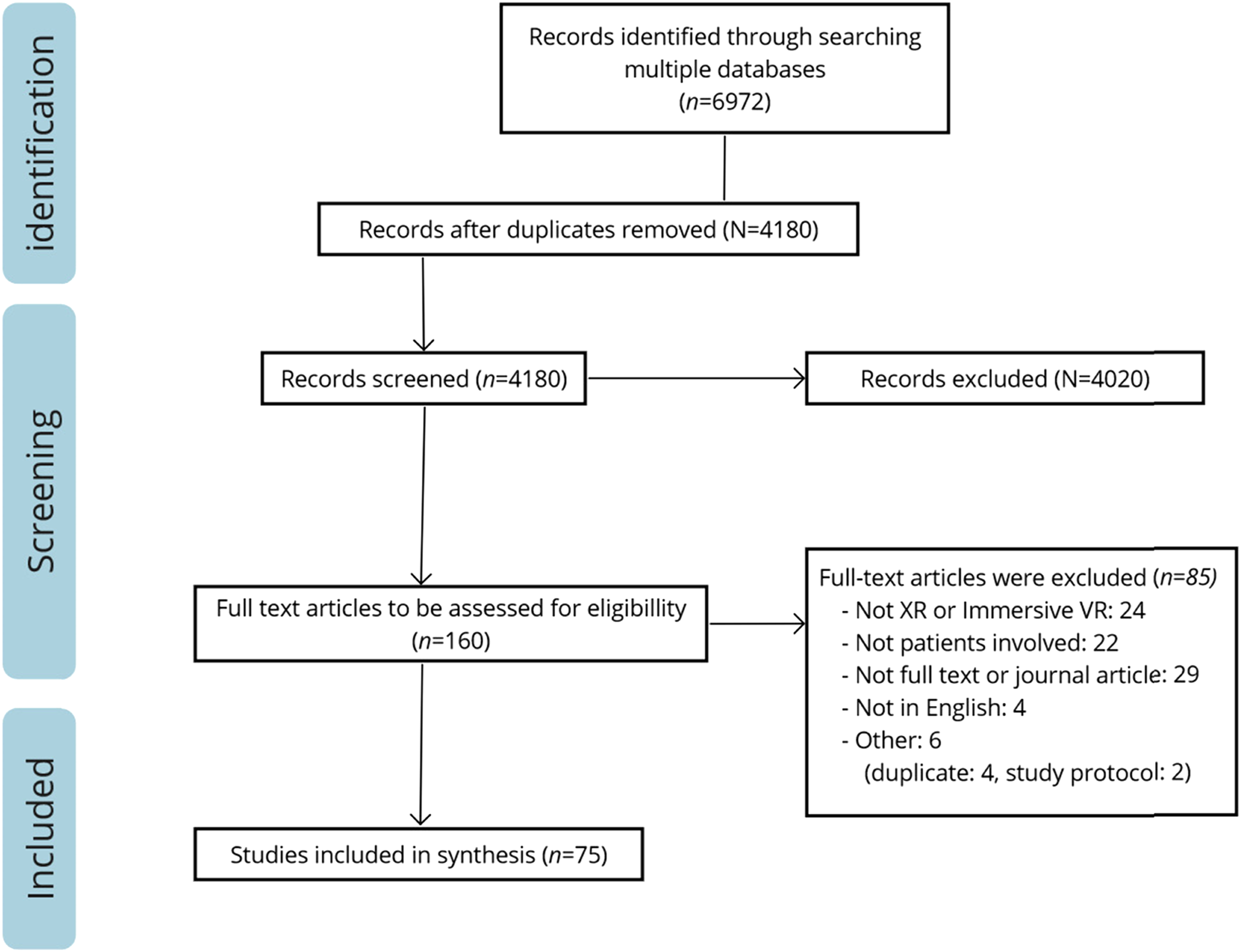
The included studies focused on different types of acquired brain injuries: stroke patients (n = 63), traumatic brain injury (TBI) (n = 7). In five studies, two or more patient groups participated, including patients suffering from multiple sclerosis, stroke, and TBI. VR was used in 70 studies, five studies described AR, and MR was not described at all. The included studies took place in various settings: in a rehabilitation clinic (n = 24), the hospital (n = 17), and five studies at home. 23 studies did not report the setting and six studies took place in multiple settings (both at home and a rehabilitation setting, outpatient, or laboratory). Designs varied from experimental studies (n = 35) including randomized controlled trials (RCTs) (n = 11), case studies (n = 10), pilot studies (n = 6), case control studies (n = 3), feasibility studies (n = 4), cross-sectional studies (n = 2), acceptability study (n = 1), prospective study (n = 1) to qualitative study (n = 1). In addition, 12 literature reviews were incorporated, including systematic reviews (n = 5), meta-analysis (n = 2), literature review (n = 3), and scoping reviews (n = 2).
Rehabilitation therapy objectives of the XR applications (sub question 1)
The objectives of the XR applications can be divided into two groups: (1) Rehabilitation therapy interventions to improve patient’s physical and/or cognitive functions (n = 57), and (2) assessments to diagnose patient’s condition (n = 14). In four articles, objectives could not be clearly determined.
Interventions
The rehabilitation therapy intervention group can be further divided into three subcategories: (1) physical (n = 40), (2) cognitive (n = 14), and (3) multipurpose (n = 3).
The physical interventions-category comprised 40 studies with a focus on improving reach and grasp tasks, gait, balance and walking, and motor function.18–57 In several studies, XR interventions were focused on reach and grasp tasks for the upper limb.21,32,39 For instance: the patient was asked to grasp virtual balls from a table and release them in a basket at another table.21,39 An example of an intervention specifically aimed at improving gait and balance uses Everybody’s Golf and Fruit Ninja, both commercial PlayStation games. Patients were instructed to alternate the cutting motion between both hands. They were also advised to selectively use the hand on the more affected side to increase engagement with that side. 48 For practicing motor function, a VR application stimulated patients to perform a series of hand movements. 35
The cognitive interventions-category comprised 14 interventions, focusing on sequence of tasks,58,64,68 practicing tasks in activities of daily living (ADL),59,61,67 improving visual field and train neglect,62,63,65,66,70,71 and other.60,69 Interventions aimed at practicing task sequence, for example, let patients buy items from the minimarket 68 or learn to prepare coffee with varying levels of difficulty and types of coffee machines. 59 Practicing ADL-tasks was facilitated by different scenes in the bedroom, such as making the bed or choosing clothes, or in the bathroom, like brushing teeth and run the bath. 59 To train neglect, visual stimuli were flashed consecutively for six seconds from right to left on the screen. During this task, the patient had to verbally identify each flashing object. For near neglect, a reaching task was utilized in which three objects turned red when touched correctly. 70
The multipurpose-category included three studies describing interventions for both physical and cognitive therapy,50,72 and one intervention aimed at distraction and relaxation. 73 An intervention that combined physical and cognitive objectives involved patients being tasked with catching a specific quantity of fish. This activity encompassed upper extremity functional exercises along with the retention of numerical information. 72 The intervention involving distraction and relaxation simulated the serene ambiance of a tranquil beach on a sunny day. This experience was facilitated while the participant’s muscles underwent stretching or passive joint mobilization. 73
Assessments
The rehabilitation assessment group can be further divided into two categories. Fourteen studies described the use of XR applications for assessment purposes of which twelve studies could be categorized into cognitive objectives75–86 and two with physical objectives.87,88 In the category cognitive assessments, nine studies focused on assessing (different forms of) neglect,80,84 specifically far and near space, 86 extra personal neglect, 79 visuospatial neglect, 83 and unilateral neglect.81,82 For instance, patients used a VR application to detect spheres and touch them as fast as possible while avoiding distractor cubes. XR application results helped therapists assess the extent of neglect. 80 Furthermore, three studies focused on memory problems.75,76,85 For example, a VR application aimed to assess memory problems through a virtual supermarket where the patient had to select groceries from a list and recall them afterwards. 85 Additionally, one study assessed the locomotor adaptation, 78 while another study assessed the impairments in visual search in life like situations using eye movement. 77 Lastly, two studies concentrated on physical functioning, 88 with one assessing upper extremity motor skills through a buzz wire task in VR. 87
Features of XR content and technologies (sub question 2)
This section provides an overview of the features of XR content and technology included in this study. Features are categorized in XR content, technologies, and XR environments.
XR content refers to the utilized environments in the XR applications whereas technologies described the applied hardware. The XR environment used or developed in the studies could be divided into three categories: (1) real-life (n = 23), (2) simple or basic (n = 23), and (3) fictitious (n = 18). The remaining 11 studies lacked adequate information or any description of the XR environment, making it impossible to categorize them.
Regarding the technologies, a wide variety of Head Mounted Displays (HMD) brands were used. Most used were Oculus quest (n = 21) and HTC Vive (n = 20). Most studies used additional hardware combined with VR devices (n = 57): controllers (n = 26), leap motion (n = 9), computers (n = 18), tracking stations (n = 6), motion capture systems (n = 5), treadmill (n = 3), or a pneumatic glove (n = 1).
The XR environments are structured in three categories: real-life environments (n = 23), simple or basic environments (n = 23), and fictitious environments (n = 18).
Real-life environments
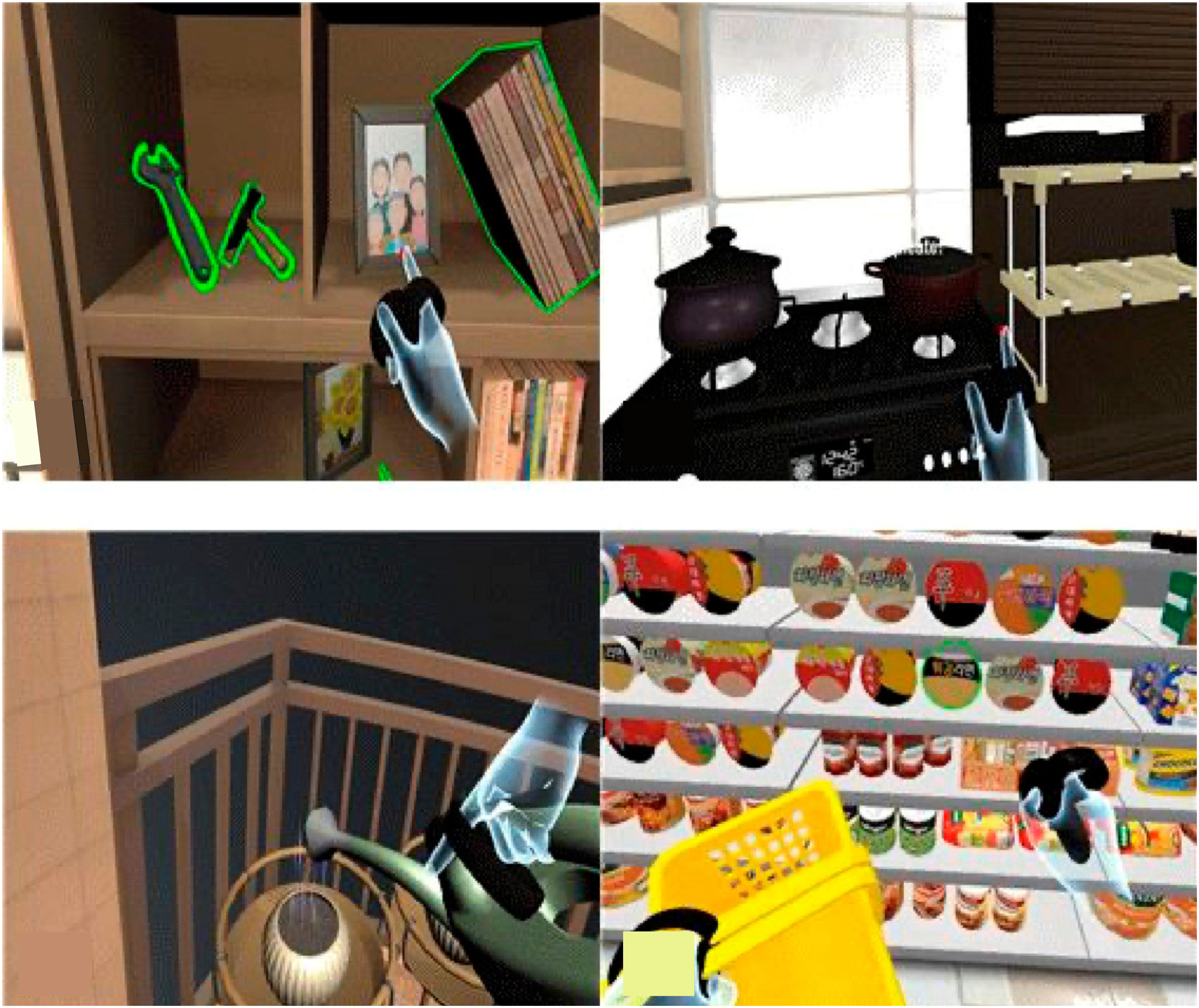
The real-life environments in 23 studies were animated and similar to daily life contexts, such as a house, convenience store or park/garden. For example (see Figure 2): a VR application for daily life training in four different scenes: a house with a living room, a kitchen, a veranda, and a convenience store.
51
The VR application included routine tasks such as activating light switches, arranging a dresser, tidying up a kitchen, tending to plants, and making purchases at a convenience store. In another study, two scenes were developed where patients could stroll in a park for a designated period.
37
Obstacles were present such as rocks, plants, and ramps. When the patient looked down, they could see their arms and feet moving. Another study developed natural outdoor scenes, such as a vegetable garden, lake, and forest. The storyline was about a farmer who became ill and needed help with gardening or watching his children.
63
Example of a VR Real life environment
51
.
Simple or basic environments
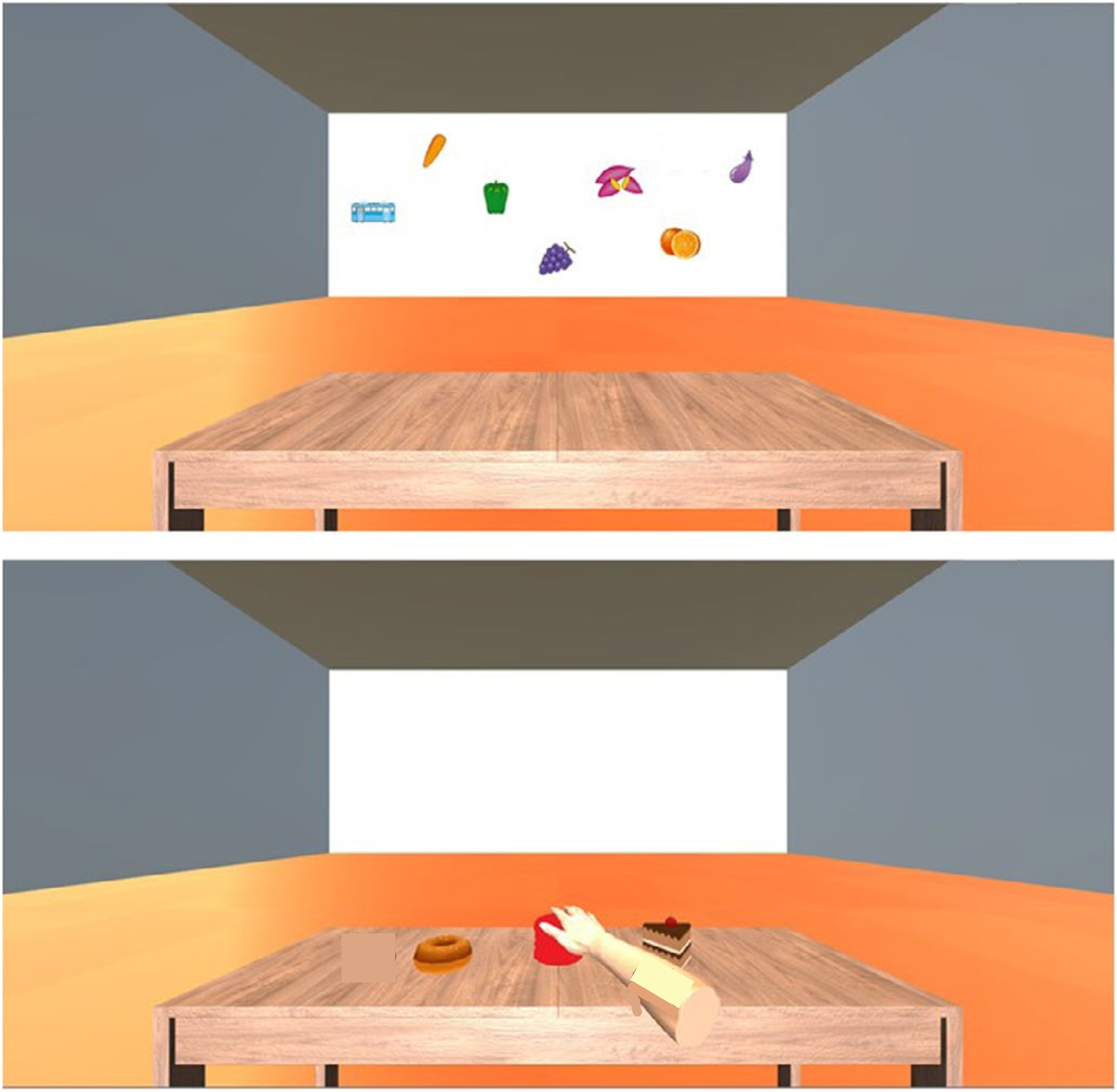
A simple or basic XR environment was used in 23 studies in which the patient could practice in a simple room, identifying objects either by hand, visually, orally, or performing a sequence of tasks. A simple room with basic elements was utilized, featuring only four walls. In some instances, it included a door and a window, devoid of any additional details or distractions in the environment (see Figure 3). This study used a virtual training space in which the controller was designed to look like the patient’s own hand.
34
The program consisted of five tasks: hammering, catching a ball, pouring, touching bubbles, and playing a xylophone. In another XR environment, the patient could sit in a wheelchair for far space training while performing a visual search task.
70
The patient had to orally identify each flashing object. During the near space training, the patient performed a reach task. In another VR application, patients performed a series of four actions to draw their attention to the neglected side of the object.
62
The actions involved displaying the clue stimulation, blacking out the surrounding environment, moving the clue stimulation, and then removing the blackout. Example of a VR basic environment
71
.
Fictious environments
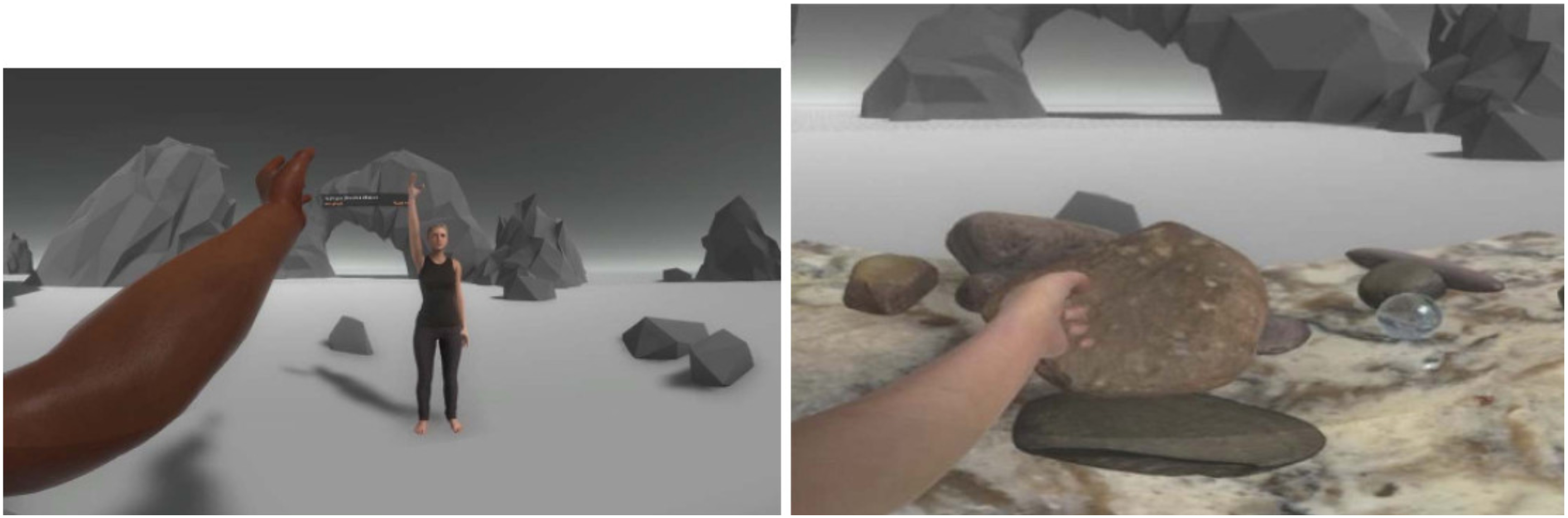
A fictitious environment was described in 18 studies. Fictious environments represented created or imagined scenarios using a wide variety of fictional characters, places or events. For instance: a VR application taking places beneath the surface, in which patients practiced grasping movements by catching fish by using his/her hands (see Figure 4).
55
Furthermore, one study utilized commercial games such as Beat Saber for physical activity. In this game, players wielded a lightsaber in each hand and sliced blocks appearing from different directions to the rhythm of music.
27
Another fictious environment was used for educational purposes in which the patient traveled through his/her own blood vessels by using the hand controller. In this way, tailored stroke visualization was created.
69
Example of a fictitious environment
55
.
Outcomes of the reported XR interventions (sub question 3)
This section provides an overview of the outcomes reported in the included studies. Outcomes are structured according to objectives of the XR interventions as mentioned in 3.1: physical, cognitive, and multipurpose interventions and assessments. Since the category multipurpose included only three studies, we do not further elaborate on this category.
Physical interventions
Physical interventions using XR were described in 40 studies with the focus on upper extremity (n = 23) or the total body (n = 17).
Interventions in 23 studies primarily focused on the upper extremity.18,20–22,24–27,29–31,34,35,38–40,42,44,46,49,51,55 These interventions aimed to improve the functional outcomes for both shoulders and elbow as well as arm, hand, and fingers or a combination of these. All studies demonstrated positive outcomes. Whereas the majority of these studies were exploratory, nine studies followed an experimental design.18,21,22,29,30,35,39,44,51 Among these studies, six utilized randomized control trials with a control group.22,29,35,39,44,51 Control groups received conventional therapy or conventional therapy with a brief VR application, e.g., 45 min of conventional therapy and 15 min of a placebo VR application. 44 The primary outcome measure in twelve studies was the Fugl Meyer Upper Extremity (FM-UE)-test22,25,26,29–31,35,38–40,44,55 and in four studies the Action Research Arm Measurement (ARAT).25,34,38,44
Seventeen studies focused on aspects of the total body, such as motor function, balance, and gait.23,32,33,43,45,47,48,53,54,56 The objectives of 13 studies were to enhance stability and/or walking ability by focusing on improvement of gait, balance, and muscle strength. Of these studies, 12 yielded positive outcomes, whereas one study highlighted several focal points regarding the utilization of XR. 32 Additionally, four studies focused on embodiment and presence, and constructs, such as motivation and enjoyment.19,28,41,50 Among these studies, three were (quasi-)experimental,19,23,56 and three were randomized controlled trials.37,47,57 The control group received therapy with non-immersive VR via a monitor, 56 conventional therapy23,37,47 or no therapy at all. 23 In one study, the control group also received experimental therapy. 19 The most used outcome measurements were the Time up and go (TUG)-test19,28,37,57 and the Berg Balance Scale (BBS).23,37,54,57
Cognitive interventions
Cognitive interventions using XR were described in 14 studies. We classified the cognitive outcomes into two groups: training neglect (n = 5), and executive functioning (n = 9).
Five studies reported neglect-related outcomes with the aim of training neglect and improving visual field. These studies encompassed two pilot studies,62,71 two case studies,66,70 and one feasibility study. 63 Positive results were observed in employing VR for neglect training as patients demonstrated improvement after following sessions using a VR application.
Second, nine studies described outcomes related to working memory.58–61,64,65,67–69 These studies especially focused on cognitive training61,68 and practicing ADL activities.59,64 Five studies had an experimental study design,59–61,67,69 among which was one randomized controlled trial. 59 The included studies all showed an improvement in the cognitive functions. More specific, significant improvements were shown by the end of the treatment for stroke patients with more severe impairments using a VR application. 59 A variety of measurements were used, such as Montreal Cognitive Assessment test (MoCA), Nottingham Extended ADL (NEADL), the Peaced Auditory Serial Addition Test (PASAT), and Wechsler Memory Scale (WMS-III).
Assessments
The application of XR technologies for assessment purposes was described in 14 studies. These studies primarily focused on assessing neglect (n = 7), memory issues (n = 3), upper extremity motor skills (n = 2), determining eye movement features (n = 1), and predict collisions (n = 1) through XR applications.
Seven studies assessed neglect to determine its level or scale. These included five experimental studies,79,81–84 one pilot study, 80 and one case study. 86 Positive results were reported regarding usability, safety, and neglect detection. Two studies utilized validated measurements, such as the line bisection test, letter cancellation test, 10-meter walk test, Rivermead Mobility Index.79,82
Second, three studies assessed memory issues, comprising one feasibility study 76 and two experimental studies.75,85 All three reported positive outcomes in immersion, feeling of engagement and usability of the XR application. However, one study found more negative effects with the HMD compared to conventional therapy. 85 One study employed validated measurements including the simulator sickness questionnaire, and Igroup presence questionnaire. 75
Third, the assessment of the upper extremity was reported in two experimental studies.87,88 Both studies yielded encouraging results, although one study noted the HMD’s weight and the complete isolation from the outside world as uncomfortable. 87 Additionally, one experimental study reported positive results for a more sensitive assessment of impairments in visual search using machine learning. 77 Lastly, one experimental study used an XR application to gain insights into avoidance strategies and underlying factors through three different experiments. 78
Considerations for implementation of XR in rehabilitation practice (sub question 4)
This section provides a summary of our findings regarding the consideration for implementation. Our findings are categorized into three sections: patient experiences, professionals-related concerns, and issues pertaining to XR content and technology. Although none of the studies explicitly mentioned evidence-based considerations for the implementation of XR in rehabilitation practice—such as acceptance, competences, costs, business cases, technological infrastructure, standardization, and ethical aspects—we did identify potential issues highlighted by the authors of the included studies that should be taken into account when integrating XR into daily practice.
Patient
Fourteen studies described experiences of patients when using the XR interventions, which could be categorized in motivation and the experienced added values after using XR.
In general, patients felt motivated when practicing with a XR application. There appeared to be notable enthusiasm among patients for utilization of VR as a training modality.25,29,38 Patients experienced VR as an engaging, motivating, enjoyable, and entertaining intervention. 56 However, not all patients were immediately enthusiastic; some needed time to adapt to the XR application. 44
Furthermore, patients exhibited a preference for VR-based games over conventional therapeutic approaches 24 and liked to use the system more often for self-training to complement the current therapy at home.43,48 Patients experienced a feeling of flow when using the XR application, resulting in fun and enjoyment.25,46 This strengthened the intensity of response to rehabilitation. 46 In addition, XR appeared beneficial to the recovery expressing enjoyment and intention to continue its use for an extended period including a contribution to therapy adherence.58,64 Patients did not experience XR as mentally exhausting, resulting in training motivation and adherence. 56 Finally, patients reported perceived enhancements in functional capacity, pain alleviation, spasticity mitigation, neglect amelioration, and improvements in walking ability.25,46
Professionals
Rehabilitation therapy professionals considered two types of challenges when integrating XR in daily rehabilitation practice: tailoring XR interventions for individual patient needs and ensuring patient support during XR use.
Four studies described the importance of tailoring XR (software) to the individual patient’s therapy requirements. For example, choosing the appropriate XR application, and adjusting the difficulty level to match the patients’ conditions, were identified as important.24,59,63,65 Additionally, encouraging the patient to engage in more frequent practice could be facilitated through the implementation of difficulty levels and gamification techniques.24,65 Furthermore, two studies reported the option of tailoring the technology by the patients themselves: one by allowing the patient to use virtual Post-it notes to plan the day 59 and another by tailoring the game to their own neglect symptoms. 63
Four studies reported considerations that professionals should be aware of when employing XR: movement patterns differed from moving in the real world, 32 and patients’ movements were less precise using a HMD. 52 Additionally, there was a necessity for providing information to patients. Enhanced acceptance is observed when the significance of XR is thoroughly communicated to the patient. 81 Moreover, assistance is essential for patients when putting on a HMD with their specific disabilities. 56
XR-technology and system
Technology-related issues were reported in 27 studies. They encompassed a variety of factors: adverse effects, need for safety measures, and issues related to hardware and software.
Twenty studies described adverse effects, implying potentially harmful and undesired effects that can occur when using XR. This involved cyber sickness (n = 14), discomfort (n = 2), and other adverse events (n = 2). Twice, the explicit absence of adverse events was mentioned (n = 2). Some studies indicated only a few mild symptoms like dizziness, headache, nausea or eyestrain.22,28,34,55,56,58,60,63,67,69,76 The symptoms manifested in diverse ways and frequently decreased during the course of the therapy session.46,48,66 Some of the studies reported additional discomfort, such as fatigue, frustration, and eye discomfort.58,80,85 Two studies highlighted issues with perceiving the HMD as heavy 52 and the fact of entirely being cut off the outside world. 87 Also, two patients provided critical feedback, citing issues such as a slippery headset. 64 Furthermore, hardware issues like a hot headset and potential visual distractions were recognized as challenges to the immersive VR experience. 33 On the other and, other studies explicitly indicated the absence of adverse effects.25,35
Four studies explicitly described safety measures, related to the use of HMD. One study described that the feeling of safety should be addressed adequately, and patients need proper information on use and safety of the HMD. 41 Another study described the necessity of using handrails and harnesses in particular cases, for instance when using a HMD in combination with a treadmill to train gait. 56 Furthermore, careful consideration, on an individual patient basis, is crucial to outweigh potential risks associated with the use of HMDs 56 with guidance and supervision of a therapist. 90 One study reported another type of safety measures: infection prevention. Cleaning HMDs is complex compared to controllers, but guaranteeing clean hardware appeared crucial, particularly when HMDs are shared among multiple (vulnerable) patients. 64
Four studies described other (not HMD-related) hardware issues. Controller design should align with the specific impairments of patients and their capabilities to interact with the XR environment.63,68 One study described difficulties with the haptic response 59 and the necessity of development of this haptic feedback. 34 Some studies indicated moderate usability issues, such as difficulties experienced by stroke patients with the controllers. 63 In addition, four studies emphasized software-related issues to consider since restrictions in the XR environment may limit engagement. 22 For example, for optimal embodiment, the whole upper extremity should be visible instead of only the hands. 34 Future applications should implicitly challenge patients to perform the correct movements in the therapy. 18 In contrast, another study claimed that the costs of developing an environment could be reduced by using simple and free assets. 36 Finally, one study emphasized the significance of integrating technical setup procedures into the implementation of technology in daily practice. 56
Discussion
In this scoping review, we gained insight into the scope of prior work, used applications, and lessons learned to be able to effectively expand upon existing research. The applications’ objectives, describing their technological features and environments, the study outcomes, and issues to consider when implementing XR applications were examined. In total, 4180 publications were screened, of which 75 were included in this review.
XR applications appeared to mainly consist of VR-technology often combining HMDs and hand controllers with software depicting environments varying from realistic environments (e.g., house, supermarket) to basic (e.g., a completely white room) and fictitious (e.g., underwater world). Applications were either contributing to physical or cognitive rehabilitation purposes or assessment purposes, such as detecting neglect, assessing cognitive functioning, or assessing motor skills. Physical rehabilitation objectives were mainly operationalized by upper extremity and total-body exercises, whereas cognitive rehabilitation objectives were reached by training neglect and working memory. It appears that both professionals and patients are motivated to use the XR technology and perceive its use as fun and promising. Adverse events such as cyber sickness seemed to remain limited. However, specific, evidence-based recommendations on how to implement XR applications to support existing rehabilitation care seem to lack in the included studies.
Regarding the objectives of the XR applications, it stands out that the identified applications solely served for physical or cognitive interventions or as assessment ‘tool’. However, literature exploring the application of XR in pain rehabilitation, cognitive rehabilitation, or psychological rehabilitation reveals additional possibilities for its use. 93 These may also be applicable to ABI-patients.94–96 For example, patients experiencing pain have found relief through VR, as it effectively distracts them from discomfort by immersing them in alternative experiences.97,98 Furthermore, XR can serve as a powerful tool for patient education and empowerment by for example providing interactive educational materials, informational videos, supporting patients to understand their condition, treatment options, and self-care strategies. We identified only one XR application that had an educational purpose. 69 The narrow-focused objectives of the identified XR applications might be explained by some factors of successful neurologic rehabilitation such as adherence, motivation, engagement, and participation activities in real-life environment 5 : elements that can more easily be facilitated by XR compared to other rehabilitation types. Additionally, another RCT study concentrated on interventions aimed at participation activities, specifically interventions that limit patient in performing daily life activities such as walking. 99 As rehabilitation encompasses physical, psychological, and social dimensions with participation and aims to facilitate maximal independence in daily activities as the primary outcome, it appears that the potential of using XR in rehabilitation is not yet fully utilized.
Out of 75 studies, 14 were about the use of XR for assessment purposes. It appeared that there has been relatively less research conducted on assessments compared to the identified physical and cognitive intervention objectives. This is remarkable, as assessment in XR appears promising due to the clear advantages of tests conducted in dynamic, three-dimensional virtual environments, compared to static traditional paper-and-pencil tests. 100 None of the studies, however, compared the XR ‘assessment’ applications to conventional assessment instruments. To facilitate the daily use of XR as an assessment tool, its use as such must first be validated. Therefore, studies do call for ecological validity of XR-based assessments in rehabilitation.101,102
Concerning XR content and technologies, our scoping review revealed a distinct separation of hardware and software features. The content could be divided into three environments: basic or simple, real life, and fictious environments. However, the included studies did not report any knowledge on how content elicit particular cognitive or physical responses among ABI-patients. Most XR environments were reported to align well with the studies’ objectives, though deeper understandings of which and how specific elements of the XR content contributed to successful outcomes could not be retrieved. Gaining more insight into this area will lead to more effective deployment of XR, allowing for more targeted decision-making during XR-development. 103 Another scoping review also found that the XR environment elicits responses, and the authors suggest that future research should focus on including implicit measures that allow for the detection of emotional and psychophysiological responses. 104 The RATE-VR guideline, currently under development, is expected to facilitate clear and comprehensive reporting in VR research, thereby ensuring that these outcomes can be extracted from the articles. 105 To improve our understanding of how content contributes to desired outcomes, future research should center on the operational mechanisms of content design.104,106
Looking at the outcomes, we found that almost all included studies about XR interventions showed positive results in favor of the XR applications. Consequently, authors of these studies emphasized the potential of XR for ABI-rehabilitation. We did identify a wide-ranging variability in study designs, application objectives, and outcome measures. Exploratory studies and pilot studies with relatively small sample sizes were predominant. It is important to point out that this study is a scoping review, without assessment of the quality of the included studies. 107 This scoping review therefore does not allow conclusions about the effects of the XR applications in ABI-rehabilitation. Nevertheless, the number of articles reporting positive results does show potential of XR in rehabilitation of ABI-patients. Furthermore, included studies show the effectiveness of XR applications remains limited; additional clinical trials are required to substantiate their efficacy. The value of these interventions lies not just in reinforcing therapy effectiveness, but also in their potential for personalization, efficiency, and engagement. They enhance the patient environment and aid therapists in fostering empathy, as well as promoting innovative treatment methods. 108
Implementation of new technology in rehabilitation implies overcoming several hurdles, encompassing concerns surrounding interoperability, technical limitations, user acceptance, lack of standardization in exercises, and integration into existing workflows.109–111 The intention to utilize technology does not necessarily translate into its actual use. 112 However, the included studies did only implicitly report about factors that impact implementation. The suggestions made by the studies’ authors remained quite conjectural, with no determinants of successful implementation based on research provided. This results in a knowledge gap regarding facilitators or barriers to implementation at the individual, team, or organizational level.89,113 Historically, incorporating evidence into clinical practice has been challenging, with findings from clinical trials taking an average of 17 years to be adopted and only half of efficacy research being implemented. 114 It is therefore logical that XR still remains in developmental or pilot stages, not yet ready for daily practice due to ongoing refinements. 115 Studies on XR development and implementation considerations may not be immediately relevant, and there is a failure to translate implementation-related factors from research outcomes to healthcare practice. 116 There remains a need for additional implementation studies to ascertain the practical benefits of XR. 117 New technological developments will continue to emerge, creating opportunities for further innovations. However, as long as the implementation of such developments in practice receives little attention, these new possibilities will have difficulty finding their way into practical application.
Therefore, more research is needed towards scaling up XR in rehabilitation. We hereby advocate to approach implementation from a multidimensional perspective incorporating the individual, societal, and organizational level.115,118,119 Innovation in the context of rehabilitation can, as mentioned in the introduction, be conceptualized as a social dimension (e.g., participation in daily activities) and perceived as a situated novelty: a multifaceted entity and a unique set of local actions, interactions, and dynamic processes within a healthcare organization to develop and implement innovations. 119 Since the majority of studies have a singular perspective, there is a need to redirect the research focus towards a more comprehensive approach within the patient’s environment using a human centered design.89,120 Additionally, the patients and lay carers’—only included in one study in this scoping review—perspective on using XR are underrepresented. 121 Following this line of reasoning, a service model approach might help in here, due to its holistic perspective, tailored solutions, value alignment, qualitative insights, and collaborative nature.122,123 By considering the needs of diverse stakeholders and aligning technology with underlying values, this approach fosters acceptance and engagement while providing customized solutions for effective implementation in real-world settings.
Our review’s careful methodology, inclusion criteria, and structured analysis and structuration of findings contribute to its strength as a valuable resource for both researchers and practitioners in the field of ABI rehabilitation. Although we applied a comprehensive search strategy across multiple databases, and had a thorough, iterative process of including articles and extracting data, with sufficient interrater reliability, our results may also have certain limitations. First, gray literature was not incorporated. This may have restricted the breadth of insights included. Second, due to the fast-paced evolution of XR technology, more recent studies may have been published that impact our results. As XR technology advances, the volume of studies is likely to grow, possibly shifting from VR to MR. Thus, it is crucial to replicate this review in the near future to capture new developments and maintain relevance.
In conclusion, this scoping review contributes to the rapidly evolving field of XR in rehabilitation by not only collecting and analyzing current evidence but also by highlighting the diversity of the field. It provides a comprehensive and multidimensional overview of research on XR applications for ABI rehabilitation identifying key elements such as objectives of these XR applications, technologies used, content offered, reported outcomes, and factors impacting XR implementation in rehabilitation practice. Based on our analysis, three key areas for further research and implementation in practice were identified. First, a comprehensive understanding of implementation factors for XR in daily clinical practice is necessary, using a holistic approach that focuses on patient participation in everyday activities, such as a service model. Additionally, larger-scale studies with standardized methodologies are essential to validate the effectiveness of XR interventions and assessment capabilities. This includes longitudinal studies exploring long-term outcomes and randomized controlled trials comparing XR with traditional methods. Second, this scoping review includes mostly VR, whereas AR and MR are expected to increase and should explore the practical requirements for transitioning towards XR utilization in clinical settings. Third, numerous opportunities for expanding XR research for ABI were revealed, such as assessment and using XR applications for other objectives.
Footnotes
Acknowledgements
The authors would like to thank professor Harry van Goor, MD for his critical reflection on this review.
Author contributions
Conception: Loes Bulle – Smid, Renée van den Heuvel, Wouter Keuning, Gido Hakvoort, Ramon Daniëls. Performance of Work: Loes Bulle – Smid, Renée van den Heuvel, Wouter Keuning, Gido Hakvoort. Interpretation or Analysis of Data: Loes Bulle – Smid, Renée van den Heuvel, Wouter Keuning. Preparation of The Manuscript: Loes Bulle – Smid and Renée van den Heuvel. Revision for Important Intellectual Content: Renée van den Heuvel, Gido Hakvoort, Ramon Daniëls, Fenne Verhoeven. Supervision: Ramon Daniëls and Fenne Verhoeven.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by two collaborations: (1) A collaboration between V3RLabs, Windesheim University of Applied Sciences, and Rehabilitation Vogellanden, Center of Rehabilitation Medicine & Special Dentistry in a project called ‘Virtual Reality for Rehabilitation – Part 2’ (TFF 2116) funded by TechForFuture, Centre of Expertise HTSM (https://www.techforfuture.nl/). And (2) a collaboration between Adelante Rehabilitation Centre, Struqt, Maastricht University, Zuyd University of Applied Sciences in a project called ‘Customized training of arm-hand skills with immersive Virtual Reality: an investigation into the optimal use of immersive virtual environments for individuals with a stroke’ (KIEM.K21.01.097) funded by Regieorgaan SIA (![]() ).
).
Ethical approval
As a scoping review, this study is exempt from requiring Institutional Review Board approval.