
Abstract
Acute flaccid myelitis (AFM) is a “polio-like” neurologic disorder of the spinal cord gray matter characterized by asymmetric, flaccid limb weakness of rapid onset following prodromal viral illness. It has affected the pediatric population of the United States since 2014, but there is a paucity of literature describing the post-acute comprehensive rehabilitation management that maximizes functional outcomes for patients. This case series attempts to mitigate this by describing the complete acute and post-acute care course of six children diagnosed with AFM in Western Pennsylvania. It is critical that pediatric rehabilitation medicine providers be knowledgeable about the complex medical and rehabilitation management for patients with AFM.
Keywords
Introduction
Acute flaccid myelitis (AFM) is a form of acute flaccid paralysis (AFP) characterized by rapid onset of asymmetric flaccid weakness in one or more limbs following prodromal viral illness that is highly selective to individuals less than 21 years of age [1]. Since August 2014, there have been 667 total cases in the United States. Most patients develop AFM in the late summer and fall with an increase in cases in 2014, 2016, and 2018 [2]. AFM is associated with unique magnetic-resonance imaging (MRI) imaging findings consisting of one or more T2 hyperintense lesions located in the gray matter of the spinal cord or brainstem [3, 4]. Non-polio enteroviruses such as CV-A16, EV-D68, and EV-A71 have been associated with AFM [5–8]. The clinical presentation of it is commonly preceded by one to two weeks of prodromal respiratory viral illness followed by acute onset flaccid limb weakness that can occur over the course of hours to days [9]. Proximal muscles are more affected than distal muscles with or without bulbar weakness; typically, sensation is spared, but autonomic dysfunction can occur. Sequelae of neurologic dysfunction lead to deconditioning, respiratory failure, dysphagia, and impairments in mobility and self-care, resulting in considerable disability [10].
According to the most current guidelines from the Centers for Disease Control and Prevention (CDC), there are no indicated targeted therapies for the treatment of AFM [11]. There is evidence of potential harm with use of corticosteroids in mouse models for both EV-D68 and EV-A71 [12, 13]. Intravenous immunoglobulin (IVIG) and plasma exchange (PLEX) are presumed to benefit the innate humoral immune response. However, the isolated benefit of either treatment is unclear due to limited studies and frequent use in combination with other treatments [14]. Neither anti-viral medications nor fluoxetine have been shown to provide benefits [13, 16]. Use of other treatments such as interferon is cautioned due to their potential to suppress the innate immune response and worsen infection [11]. Although some of these pharmacologic interventions were utilized in the patient cohort, the science and understanding about the lack of absolute clear benefit of these interventions has emerged since this cohort’s clinical presentation. More advanced approaches have been described in the literature, including diaphragmatic pacing for those with chronic respiratory failure and peripheral nerve transfers for restoring motor function [17, 18].
Due to the medical complexity and considerable impairments found in many children with AFM, comprehensive inpatient rehabilitation is often required in the post-acute phase, where medical management and intensive multidisciplinary therapy coincide to maximize functional recovery and coordinate discharge planning. In 2018, there were 238 cases of AFM in the United States, with five of those cases occurring in Western Pennsylvania; one additional case from 2016 was later identified and is also included in this case series [2]. While acute management approaches have been described in the literature, there remains a dearth of literature describing rehabilitation management and functional outcomes in children with AFM. The aim of this study is to describe the rehabilitation management from a single institution in Western Pennsylvania in the context of the complete acute and post-acute courses of six children with AFM.
Case descriptions
This retrospective case series describes six cases of AFM that occurred at the UPMC Children’s Hospital of Pittsburgh (CHP) in Pittsburgh, Pennsylvania, between January 2014 and October 2019. In a previous paper by several contributing authors, three cases were described from the perspective of early identification and acute management [19]. The University of Pittsburgh Institutional Review Board approved this study under the exempt category for human subject research, and all patient-related data was deidentified for the purposes of this case series.
Diagnosis and acute medical management for each case occurred at CHP, and early post-acute comprehensive rehabilitation occurred at Children’s Hospital Rehabilitation Unit (CHRU). Pediatric rehabilitation medicine (PRM) was consulted for rehabilitation management during acute hospitalization and evaluation for acute inpatient rehabilitation. Table 1 summarizes patient demographics, clinical characteristics, work-up, and treatments during acute hospitalization. Figure 1 shows a timeline of initial presentation and management within the first ten days of acute admission. Patients were transferred to CHRU once medically stable and deemed able to tolerate the appropriate therapy intensity. Comprehensive inpatient rehabilitation included at least three hours of therapy, six days per week, with multiple therapy disciplines, including physical therapy (PT), occupational therapy (OT), and language pathology (SLP). Functional electrical stimulation (FES) was performed on each patient, with results shown in Table 3. Team meetings occurred weekly to discuss patient and family-centered goals as well as discharge planning. Specialized rehabilitation nursing was available for medication administration, skin care and protection, and management of neurogenic bowel and bladder. Additional service providers included a teacher, behavioral health specialist, neuropsychologist, recreation therapist, child life assistant, music therapist, case manager, and social worker. Active medical management was directed by a board-certified PRM physician. Pulmonology and respiratory therapists were available for assistance in mechanical ventilation management. Functional assessments were scored using the Functional Independence Measure for Children (WeeFIM), which is a validated rehabilitation outcome scoring system [21]. This scoring system, shown in Table 2, assigns a score from 1 to 7 for functional tasks, with 1 indicating dependent or total assistance and 7 indicating independence. Due to known age-related effect on WeeFIM scores, a developmental functional quotient (DFQ) for the domains of the WeeFIM score was calculated to allow for score comparison based on age-normative data. DFQ scores closer to 100 indicated a functional status closer to that expected at the child’s age [22].
Patient demographics and clinical characteristics
Patient demographics and clinical characteristics
Abbreviations: ITP, immune thrombocytopenic purpura; IVIG, Intravenous immunoglobulin; PLEX, plasmapheresis; RBCs, red blood cells; EBV, Epstein-Barr virus.
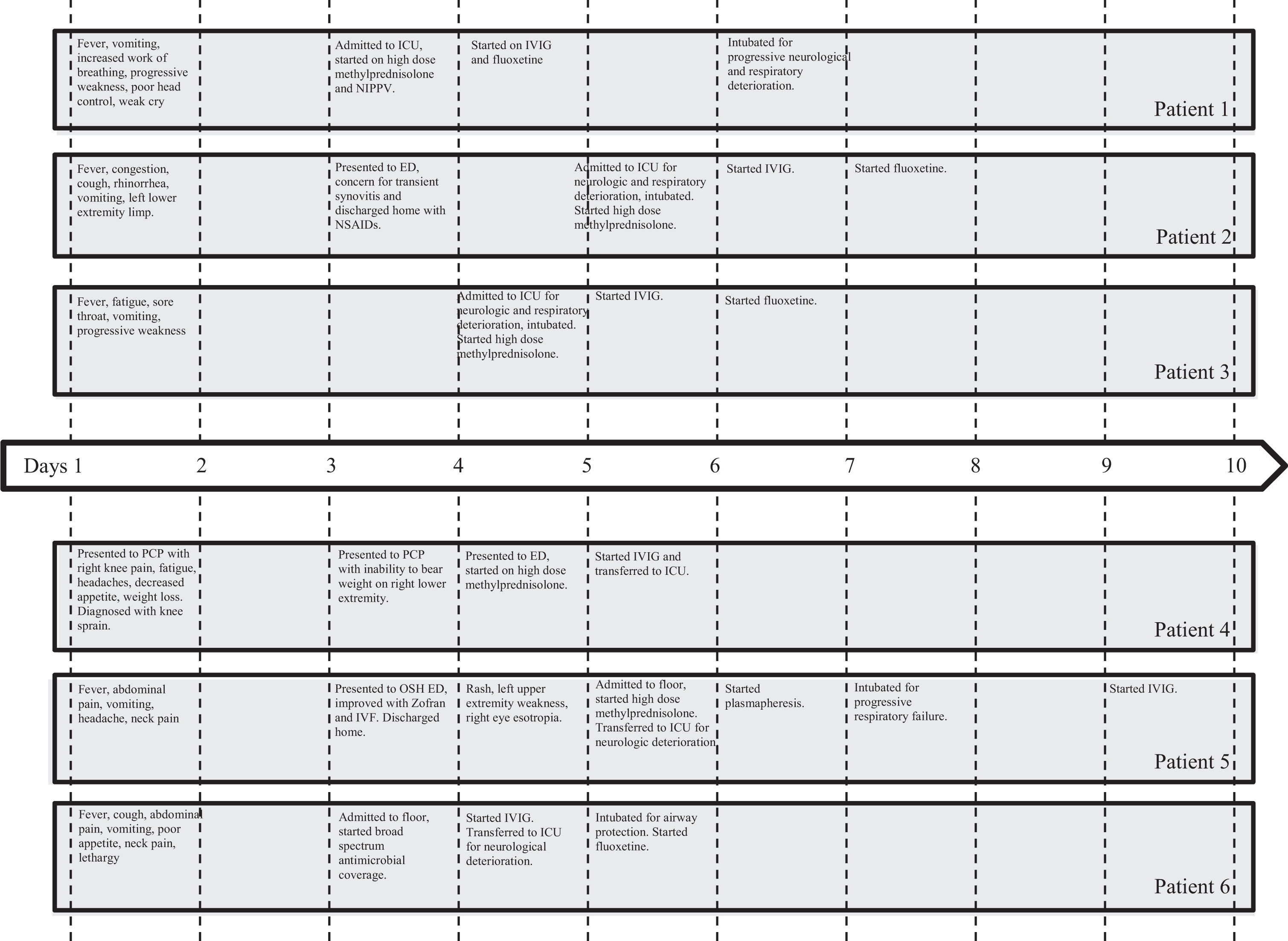
Initial acute course timeline within the first 10 days of presentation. Abbreviations: ICU, intensive care unit; IVIG, intravenous immunoglobulin; ED, emergency department; PCP, primary care provider; OSH, outside hospital.
WeeFIM Measure of Function
Abbreviations: WeeFIM, Functional Independence Measure for children.
An 11-month-old girl presented to an outside facility with difficulty walking, poor head control, and weak cry following a diagnosis of otitis media one day prior with fever and emesis. Due to progressive weakness, she was transferred to the CHP pediatric intensive care unit (PICU). She was hypotonic with poor head control, diminished reflexes in the bilateral upper extremities and left lower extremity and lacked spontaneous movements. Empiric methylprednisolone was administered due to initial consideration of transverse myelitis (TM), however, MRI evidence of subtle T2 hyperintensities without enhancement in the cervical spinal cord gray matter shifted the diagnosis to AFM. IVIG was administered on the fourth day after illness onset. Additional treatments and lab findings are summarized in Table 1. She eventually required tracheostomy and gastrostomy tube placement and was transferred to the CHRU on hospital day 31.
Following 82 days of inpatient rehabilitation, she demonstrated improved upper extremity strength (left greater than right), fine motor skills, head control, standing tolerance, and sitting tolerance for age-appropriate play. PT and OT trialed FES, is summarized in Table 3. She remained on enteral tube feeds but could tolerate 2 oz volume of thin liquids by mouth three times per day. Notably, WeeFIM DFQ total score decreased with decrements in all three subdomains (Table 4), attributed to advancement in age without notable improvement in function. Complications included two separate transfers to acute care; once for tracheitis with respiratory distress and another for hemorrhagic shock secondary to gastrointestinal bleed. Respiratory management on mechanical ventilation included improved tolerance to sprinting off the ventilator for 30 minutes a day, three times per week. She was discharged home with early intervention home-based and outpatient therapies. Durable medical equipment is summarized in Table 3.
Inpatient Rehabilitation Management Summary
Inpatient Rehabilitation Management Summary
Comparison of WeeFIM DFQ scores and percent change between inpatient rehabilitation admission and discharge
Abbreviations: WeeFIM, Functional Independence Measure for children; DFQ, developmental functional quotient; D/C, discharge; %, percent change. Note: Cognitive scores were included in the calculation of total WeeFIM and DFQ scores but are not shown due to minimal changes across all patients.
A 2-year-old boy presented to the Emergency Department (ED) with two days of fever, emesis, rhinorrhea, cough, limp, and left lower extremity areflexia. Following negative work-up, he was discharged home with presumed transient synovitis. The patient returned two days later with acute onset truncal weakness, poor neck control, flaccid paralysis of both lower extremities, and decreased strength in the bilateral upper extremities. Absent reflexes were noted in all limbs except for the right upper extremity. Within three hours, bulbar weakness followed with poor secretion management warranting intubation and PICU transfer. Intravenous methylprednisolone was administered due to consideration of TM. MRI revealed increased T2 signal within the central gray matter of the entire spinal cord, as well as the dorsal pons (Fig. 2). AFM was diagnosed, and IVIG was administered five days after illness onset. The patient underwent placement of tracheostomy and gastrostomy tube. Additional treatments and lab findings are listed in Table 1. He was transferred to CHRU on hospital day 25.
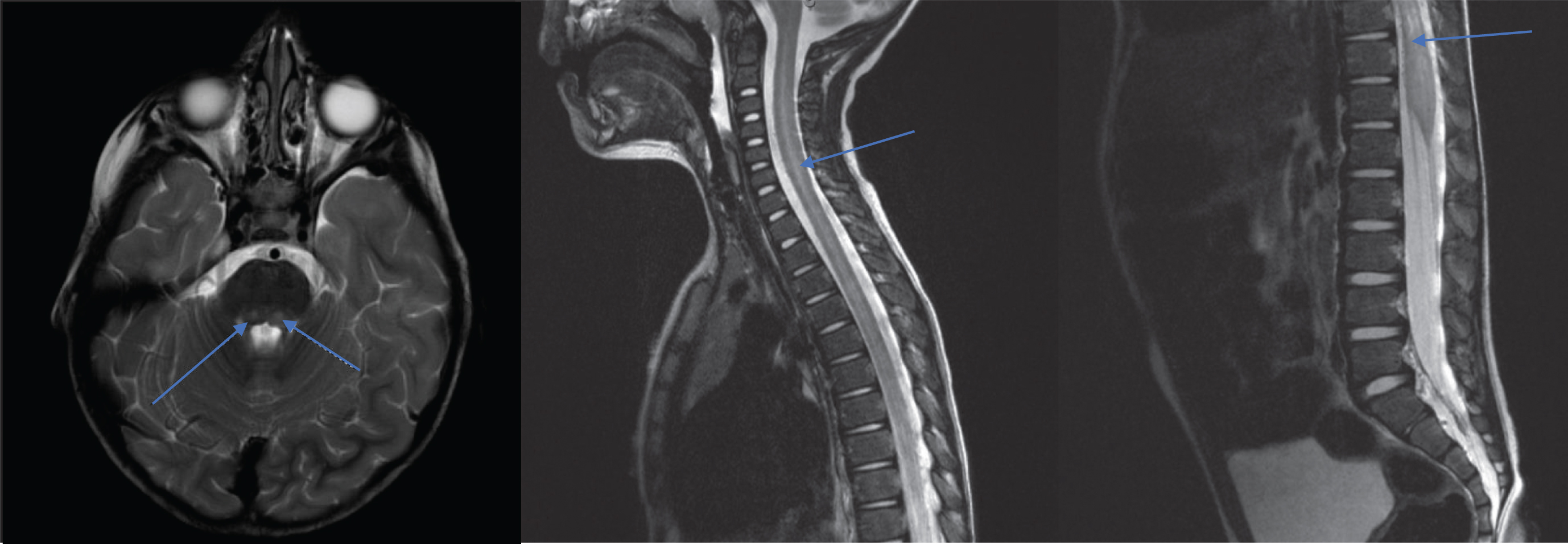
MRI images of patient 2, displaying increased T2 signal within the central gray matter of the entire spinal cord, as well as dorsal pons (blue arrows).
He received 109 total days of inpatient rehabilitation, most notable for increased volitional control of his right upper extremity (trapezius, fourth lumbrical, extensor indicis proprius), improved respiratory tolerance during supported static sitting and car seat trials, tolerance of in-line (in circuit with his ventilator) Passy Muir valve (PMV) up to 30 minutes, diet advancement, and progression to supervision with power wheelchair mobility using adaptive controls including a modified head array. WeeFIM DFQ total score increased with the most improvement noted in the mobility subdomain (Table 4). He required total assistance for transfers, age-appropriate self-care tasks, and play. His course was complicated by PICU transfer for acute respiratory distress in the setting of tracheitis and atelectasis. Notably, there were several episodes of autonomic dysreflexia (AD) characterized by increased diaphoresis, flushing, hypertension, and tachycardia. These episodes were triggered by constipation, tube feed boluses, and one episode was suspected to be triggered by FES to the cervical muscles. Clonidine was used to address episodes not amenable to typical interventions, including position adjustment, bowel, bladder, and skin care. He was discharged home with early intervention home-based therapies, outpatient therapies, and equipment summarized in Table 3. The patient underwent a right spinal accessory nerve transfer to the left phrenic nerve approximately 11 months after initial symptom onset to improve his diaphragm function.
A 3-year-old boy presented to the ED with three days of fever, pharyngitis, lethargy, emesis, and generalized weakness. In the ED, he was tachycardic, irritable, and demonstrated truncal weakness with concerns for sepsis. He was transferred to the PICU due to decreased spontaneous movements in all extremities with symmetrically diminished reflexes and required intubation 10 hours into admission due to the inability to protect his airway. MRI showed increased T2 signal in the grey matter of the brainstem, cervical and thoracic spinal cord. Intravenous methylprednisolone was administered four days after illness onset based on differential diagnosis of TM. However, the diagnosis was changed to AFM, and IVIG was administered five days after prodromal onset. On hospital day nine, he was transferred to inpatient rehabilitation.
Due to family preference, the patient was admitted to CHRU for 12 days prior to being transferred to an outside inpatient rehabilitation facility. Prior to transfer, MBS resulted in diet advancement to purees with thin liquids while maintaining tube feeds for nutrition through nasogastric tube. WeeFIM DFQ total score decreased (Table 4), and he remained a total assist for all self-care tasks and functional mobility. FES was trialed for two sessions with good tolerance, but no muscle contraction was visualized or palpated. Upon discharge, he demonstrated flaccid quadriplegia (trace right greater than left toe flexion) with poor neck control. He was discharged with a cervical collar and car seat for transportation. He was admitted to the outside inpatient rehabilitation facility for 65 days and discharged home. Complications included three acute care transfers for pneumonia, one of which required intubation. He was eventually extubated and transitioned to nighttime CPAP with use of cough assist and a chest vest. He was discharged with early intervention home-based and outpatient therapies along with home nursing. Equipment is summarized in Table 3. He underwent nerve transfer surgery ten months following initial presentation to improve bilateral elbow flexion and at 11 months to improve right hip extension and knee flexion.
Case 4
A 3-year-old boy with a history of immune thrombocytopenic purpura presented with four days of fever, headaches, rash, abdominal pain, emesis, and left upper extremity weakness supported by physical exam with diminished reflexes and additional right eye esotropia. MRI showed increased T2 signal in the brainstem and spinal cord grey matter. Based on a working diagnosis of TM, intravenous methylprednisolone was administered. Within hours of admission, the patient developed progressive flaccid quadriplegia requiring transfer to the PICU. He was treated with PLEX on hospital day two and later given IVIG on hospital day 8. He was intubated and eventually underwent tracheostomy and gastrostomy tube placement. He was transferred to the inpatient rehabilitation unit on hospital day 38. Of note, this patient’s extremities remained flaccid with intact sensation months after his initial presentation. Upon detailed review of his neuroimaging, his final diagnosis was changed from TM to AFM.
Following an 80-day inpatient rehabilitation course, he demonstrated improvements in WeeFIM DFQ mobility and cognition domains. Complications included autonomic dysreflexia and an episode of respiratory distress requiring one transfer back to the PICU. At discharge, he had increased tolerance of prone positioning, edge of bed activities, and use of the stander. He remained dependent for all self-care tasks but advanced to supervision with power wheelchair mobility using adaptive controls. The patient demonstrated active cervical neck range of motion and right thumb movement with emergence of upper trapezius, triceps, and brachioradialis activation. FES was attempted once with good tolerance targeting the left quadriceps, but no palpable contraction was noted. MBS demonstrated safety to advance to a pureed diet with thin liquids. He was discharged on oral pleasure feeds, and enteral tube feeds via gastrostomy tube to maintain caloric needs. At discharge, the patient was voiding volitionally but continued to require neurogenic bowel program with bisacodyl suppository and digital stimulation. He was discharged with early intervention home-based therapies, outpatient therapies, and equipment summarized in Table 3.
Case 5
A 3-year-old boy presented to the ED with four days of right knee pain, headaches, decreased appetite, and weight loss in the context of a viral prodrome 2-3 weeks prior to presentation. On initial evaluation, the patient demonstrated right lower extremity weakness and areflexia. Intravenous methylprednisolone was initiated due to concerns for TM. MRI showed increased T2 enhancement of the anterior cauda equina nerve roots with an abnormal T2 signal within the distal cord without structural compression. He was transferred to the PICU and treated with IVIG. On hospital day 8, he was transferred to inpatient rehabilitation.
The patient completed an 8-day course in inpatient rehabilitation. He progressed to an age-appropriate level in self-care tasks and demonstrated that he was able to ambulate with close supervision and used a right knee hyperextension orthosis. FES was trialed unsuccessfully due to fear avoidance. Bowel and bladder function recovered, and he was advanced to a regular diet and discharged to outpatient PT without equipment needs.
Case 6
A 6-year-old boy with history of motor tics presented to the ED with two days of fever, lethargy, cough, poor appetite, abdominal pain, and emesis. Initial evaluation was notable for tachycardia, tachypnea, hypertension, and truncal weakness. The patient was admitted to the floor with concerns for acute disseminated encephalomyelitis (ADEM) and was started on empiric antibiotics and antivirals for meningitis. MRI showed increased T2 signal throughout the central gray matter of the spinal cord, most prominent in the anterior horns. On hospital day 2, he developed progressively worsening bilateral upper extremity weakness followed by lower extremity weakness, diffusely diminished reflexes, dysphagia, and difficulties managing secretions. The working diagnosis was changed to AFM, and the patient was started on IVIG. He underwent placement of tracheostomy and gastrostomy tube and was transferred to inpatient rehabilitation on hospital day 29.
The patient participated in 62 days of inpatient rehabilitation, where he progressed from dependent for self-care tasks and functional mobility to supervision with ambulation up to 150 feet, stair negotiation, and transfers. While he required total assistance with bathing, he required less assistance for other self-care tasks such as dressing and grooming. Total WeeFIM DFQ improved over time (Table 4). While he demonstrated cervical weakness, he was able to move all extremities against gravity. He required two acute care transfers for mucous plugging and secretion management, but his tracheostomy eventually decannulated. He tolerated a regular diet with thin liquids, but required supplemental tube feeds for nutritional support. He was discharged home with outpatient therapies and equipment. Eleven months after initial symptom onset, the patient underwent left upper extremity nerve transfers at an outside hospital, which included spinal accessory nerve to suprascapular nerve transfer (to improve shoulder abduction and external rotation), median nerve group fascicle to biceps nerve transfer (to improve elbow flexion), ulnar nerve group fascicle to axillary nerve transfer (to improve shoulder flexion and abduction), radial nerve group fascicle to triceps motor nerve transfer (to improve elbow extension), and neuroplasty of the axillary, radial, ulnar, and median nerves.
Discussion
This retrospective case series underscores the sequelae of AFM and demonstrates the important role that pediatric rehabilitation medicine and the multidisciplinary approach play in the post-acute care continuum. Compared to a larger cohort in another study, the average acute care length of stay was shorter (23.3 days±SD 12.2 days vs 49.1 days±SD 74 days), and the average duration of inpatient rehabilitation was longer (69.5 days±SD 33.8 days vs 42.3 days±SD 67.6 days) for the patients included in this study [23]. Total WeeFIM DFQ scores at discharge indicated that the overall functional status of the patients remained below age expectations (Fig. 3), even after intensive inpatient rehabilitation. However, four patients demonstrated improvement in self-care, mobility, and total WeeFIM DFQ scores, as demonstrated in Table 4. Mean total WeeFIM DFQ was 34.7 (SD 19.2) on admission and 44.8 (SD 23.0) at discharge, with improvement within each domain shown in Fig. 4. Although there was not a control group of children with AFM who did not receive early intensive inpatient rehabilitation, it is believed the degree of functional gains demonstrated by this cohort within this timeframe would be unlikely without intensive therapy.
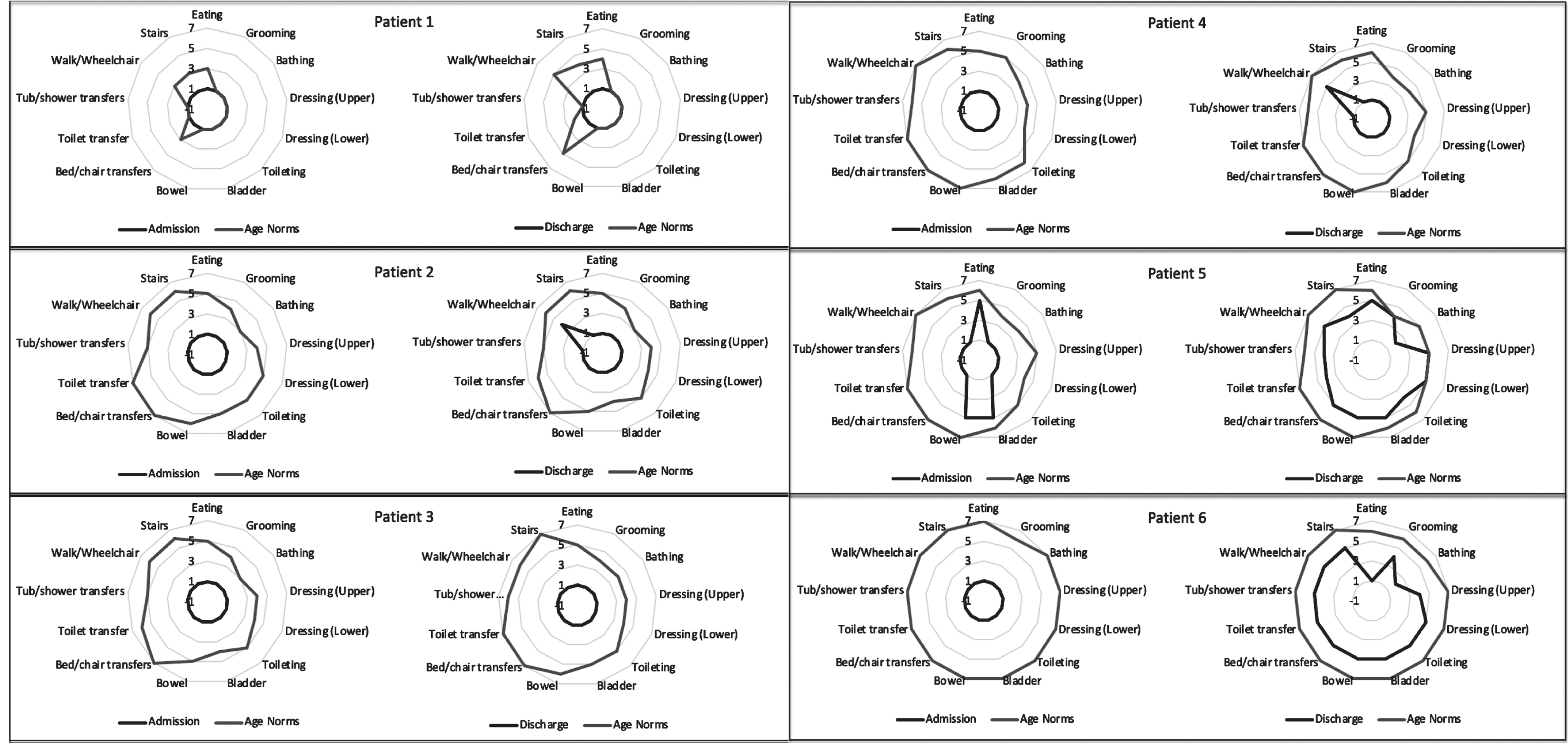
WeeFIM self-care and mobility scores at admission and discharge (dark grey) from comprehensive inpatient rehabilitation. WeeFIM scores for each patient are compared to age norms (light grey). Cognitive scores were included in the calculation of total WeeFIM and DFQ scores but are not shown due to minimal changes across all patients.
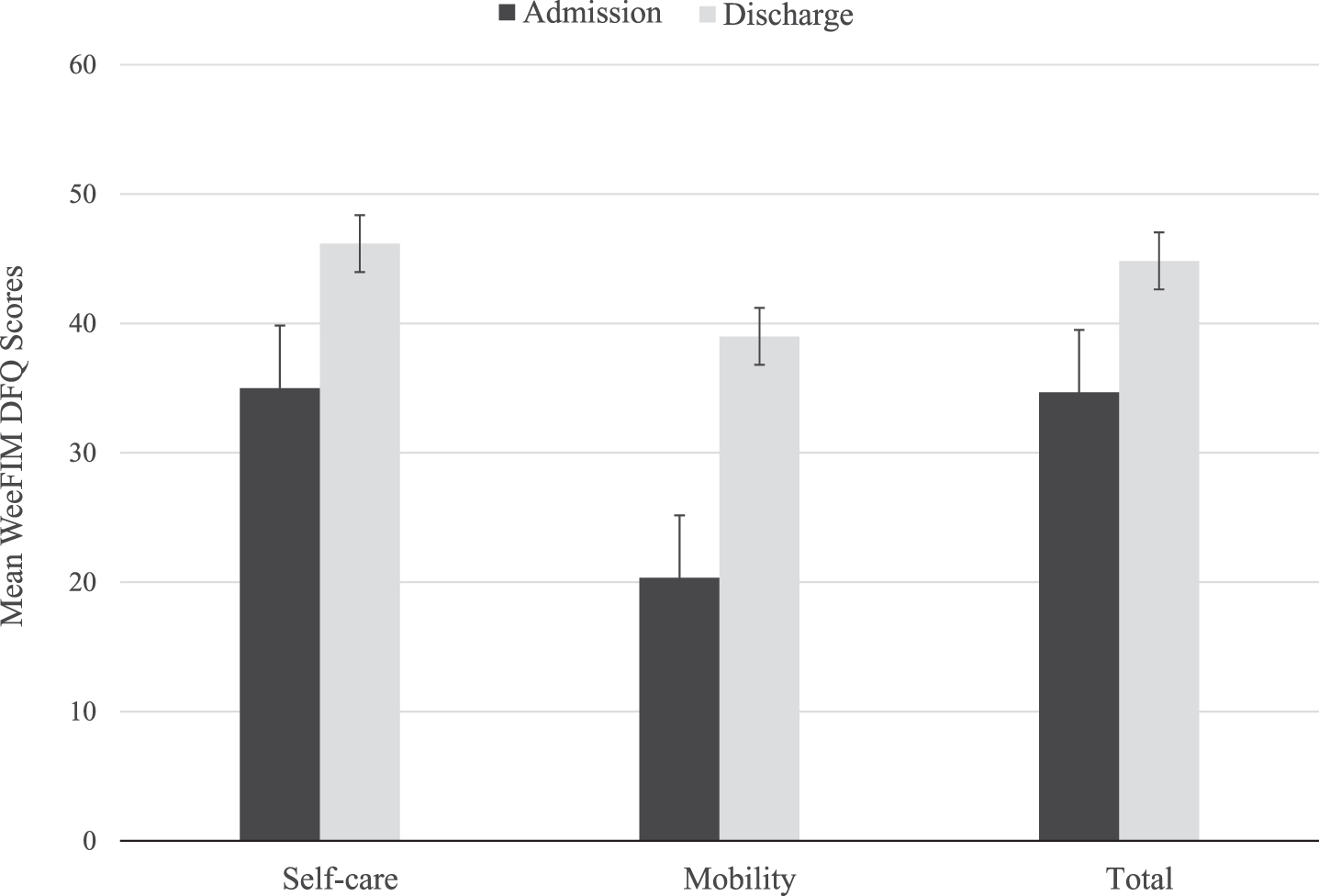
WeeFIM DFQ Scores on Admission and Discharge from Inpatient Rehabilitation.
Three patients required mechanical ventilation upon discharge home. Current literature cites a range of 10–40% of patients with AFM requiring mechanical ventilation at some point in their care [24]. It is therefore important for pediatric rehabilitation providers to work closely with pulmonology and respiratory therapy to ensure that patients with AFM are being provided with adequate respiratory support and optimized pulmonary toileting regimens to mitigate risk of infection, which was the most common complication in this cohort. Since chest physical therapy is a mainstay of pulmonary toileting, pediatric rehabilitation providers should ensure that parents and caregivers have been thoroughly trained in its provision. While prone positioning is often used in acute respiratory failure to minimize atelectasis and ensure that the lowest effective ventilator settings are being used, there is little evidence for its utility in individuals with chronic respiratory insufficiency [25]. However, based on the experience of these cases, prone positioning can be safely trialed during inpatient rehabilitation, and appropriate equipment and training arranged for continuing prone positioning at home.
Complications included respiratory failure with associated infections (tracheitis and pneumonia) in the setting of tracheostomy and mechanical ventilation, dysphagia requiring gastrostomy tube placement, and autonomic dysreflexia. Given the important neurologic sequalae of AFM in this cohort, specifically respiratory insufficiency, it is not surprising that 4 out of 6 patients required readmission to acute care during their inpatient rehabilitation. The higher prevalence of quadriplegia and related respiratory insufficiency compared to other AFM case series partially explains the high readmission rate. However, the reason for relatively more neurologic impairment in this cohort remains unclear [14].
FES provided a novel therapy modality that facilitated muscle contraction in three patients. However, tolerance was limited due to pain, fear avoidance, and a case of autonomic dysreflexia. FES has been used over decades to facilitate muscle strengthening, spasticity reduction, and motor recovery for a variety of diagnoses, including stroke, traumatic brain injury, and spinal cord injury [27]. It has been theorized that FES may induce neuroplasticity in the central nervous system through central modulation, but it is unclear if it can be effective at facilitating preservation at the level of the anterior horn cell affected in AFM. FES has been used in lower motor neuron spinal cord injuries and in activity-based therapy in AFM [28, 29]. Recent published literature indicates that FES should be trialed early in the rehabilitation phase, but the adverse event of autonomic dysreflexia should be noted as a potential risk, especially in patients with cervical level and high thoracic level lesions [24]. As seen in the case series, partial preservation of motor function does occur for some patients in some myotomes. FES is likely to be of the most benefit for this subgroup of individuals with AFM. In addition, after FES tolerance has been demonstrated, parents/caregivers should be trained on its use so this can be done outside of dedicated therapy hours on an inpatient rehabilitation unit.
Three patients underwent nerve transfer procedures several months after their initial diagnosis (average 14.3 months after symptom onset, range 11–18 months). There is a limited window of opportunity for nerve transfer surgeries. Once the lower motor neuron injury occurs, the motor endplate undergoes degeneration and will be permanently lost if no reinnervation occurs before 18 to 24 months. Some studies have recommended nerve transfer surgery 6 to 9 months after symptom onset. Postoperative gains in elbow function have been more reliable compared to shoulder function [18]. Therefore, it is believed that given the few effective treatment options for this condition, early referral to specialists who perform nerve transfers should be standard of care for children affected by AFM.
An important benefit of intensive inpatient rehabilitation is thoroughly preparing parents and caregivers to care for children with new functional deficits. The children described here were healthy and developmentally appropriate, with a pediatrician as their only medical provider prior to their AFM diagnosis. Following discharge, they were seen by multiple pediatric subspecialists, and their care needs dramatically changed. Parents were tasked with the operation of equipment as listed in Table 3, performing safe transfers, medication administration, and respiratory and nutrition management. Acute care hospital systems are not designed to provide caregivers with adequate support and education to care for complex children with new functional deficits, so this is an area where pediatric rehabilitation units and teams can provide immense value.
Comprehensive inpatient rehabilitation should be strongly considered to maximize functional outcomes and quality of life in children and families affected by AFM. Patients made functional gains in different aspects of age-appropriate mobility, self-care, feeding, swallowing, and communication but often remained below age-related norms. Although it cannot be concluded based on this case series that these functional gains would not have been made if these patients had not received comprehensive inpatient rehabilitation, the complex care coordination and discharge planning that is involved in successfully transitioning patients with AFM home is much more likely to be successful in the inpatient rehabilitation setting. FES may have a role in motor preservation and recovery but had variable tolerance. Patients with persistent motor deficits have benefitted from nerve transfer surgery. Since future recurrences of AFM are expected, it is important for PRM providers to be knowledgeable of the complex medical and rehabilitation management for patients with AFM.
Footnotes
Acknowledgments
We would like to acknowledge the efforts of Kristyn Felman, MPH, CPH, MSW, for her assistance in research project coordination and data acquisition.
Conflict of interest
The authors have no conflict of interest to report.
Funding
The authors have no funding sources to report.