
Abstract
PURPOSE:
Objectives included identifying programs that provide pediatric inpatient rehabilitation services (IPRs) across the United States (US), describing differences in location, admission criteria, available resources, personnel and staffing, and populations served between pediatric rehabilitation programs with the overall goal to evaluate rehabilitation needs in geographical areas with limited access for targeted program development.
METHODS:
Online survey emailed to pediatric physiatrists who worked or directed IPRs and completed between December 2018 to March 2019.
RESULTS:
Fifty respondents completed the survey of the seventy-one distributed. Fifty percent of pediatric inpatient rehabilitation services are within a free-standing pediatric hospital with an average of 14 beds. Twenty-eight programs provide acute services with almost half providing accredited specialized programming. All respondents reported that inpatient rehabilitation treatment teams included pediatric physiatry, nursing, social work, and core therapy disciplines.
CONCLUSION:
Although characteristics of pediatric inpatient rehabilitation services vary, similarities exist with respect to team composition, clinical coverage, admission or documentation criteria, and outcome measures. The geographic distribution of pediatric IPRs including available specialty programming reveals resource-limited areas. Results from this study emphasize how practice standards or fiscal limitations impact program structure, resources, and ultimately short- and long-term healthcare outcomes among the population of pediatric rehabilitation patients.
Introduction
Children and adolescents who have survived severe illnesses or injuries or undergone significant surgery resulting in changes in function and ongoing complex medical needs often benefit from a transition to a post-acute level of service. Those who demonstrate a need for, and can tolerate, comprehensive programming with multiple disciplines typically transition to inpatient rehabilitation services (IPRs). The Centers for Medicare and Medicaid Services (CMS) publishes regulations and requirements that largely influence adult inpatient rehabilitation and post-acute care provision throughout the United States (US) [1]. Services and programmatic requirements are then created within institutions to meet these regulations, thereby influencing payment, reimbursement, or private payor contracts. Although Medicaid is funded jointly by states and the federal government, it is mostly implemented on a state level. Anecdotal experience with different inpatient pediatric rehabilitation programs through training, practice, and networking has provided observations about the potential diversity in systems. Currently, there exists limited data regarding pediatric IPR practices. Houtrow et al.’s published study regarding the field of pediatric rehabilitation medicine provides the most data for pediatric physiatrists [2]. Even though the large majority of pediatric physiatrists provide management of patients in both outpatient and inpatient clinical settings, a minority devote most of their time to inpatient practices [2]. The milieu of post-acute care services in the pediatric population is largely undocumented. The hypothesis of this current study is that common elements exist among pediatric inpatient rehabilitation practices, yet much variability exists amongst programs nationwide. This survey aimed to identify pediatric IPRs across the US and describe differences in location, admission criteria, available resources, personnel and staffing, and populations served between pediatric rehabilitation programs with the overall goal to evaluate rehabilitation needs in geographical areas with limited access for targeted program development.
Methods
Study population
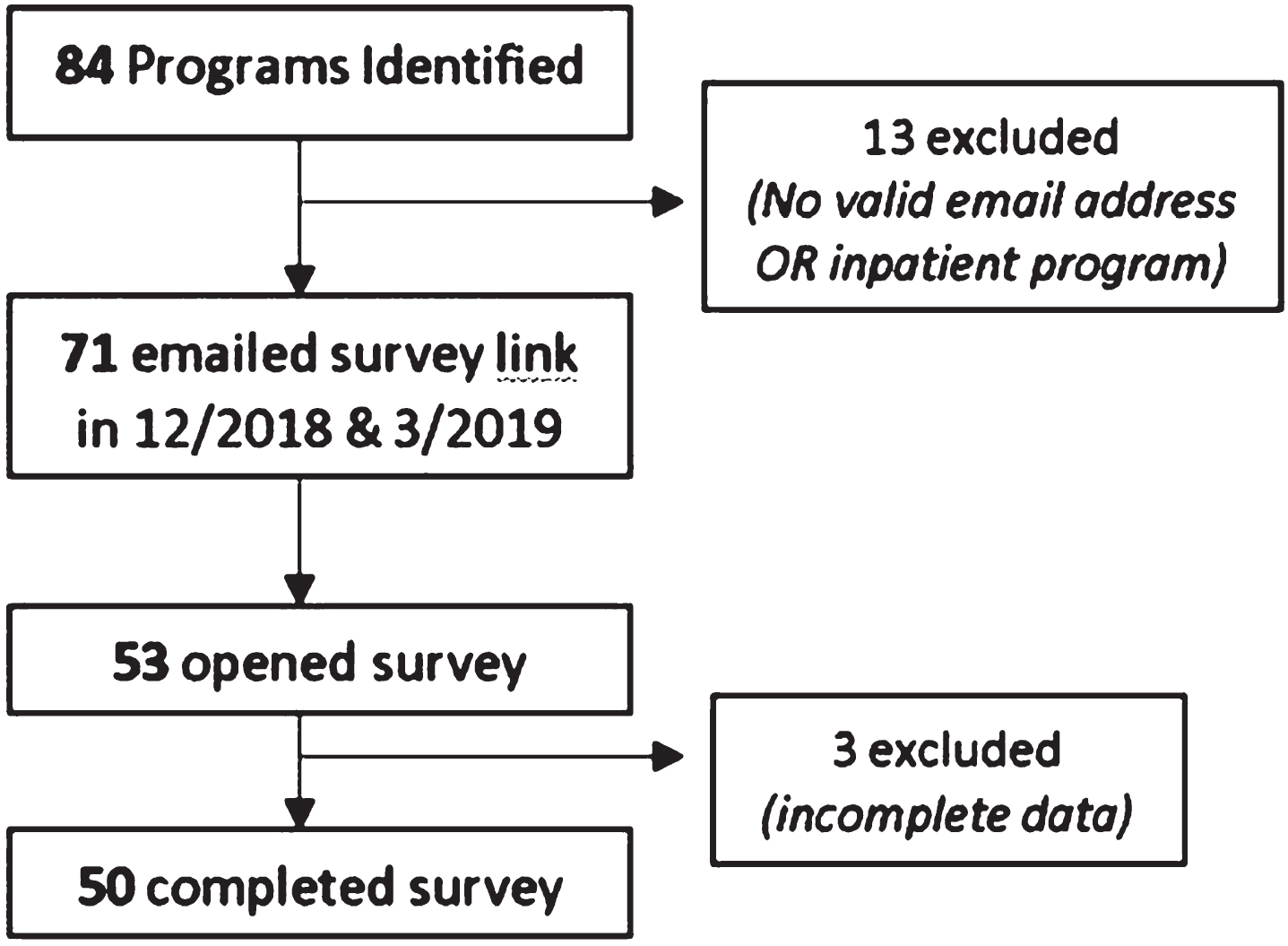
Programs with IPRs were identified via the Commission on Accreditation of Rehabilitation Facilities (CARF) website (programs accredited for pediatric inpatient population, as listed). An advanced search for “Inpatient Rehabilitation Programs - Hospital ” and “Pediatric Specialty Program” was conducted with a total of 36 programs. Not all pediatric IPRs are CARF accredited. Additional IPRs were identified with information from hospital websites (identified by searching the internet for “Inpatient Pediatric Rehabilitation”), the American Academy of Physical Medicine and Rehabilitation (AAPMR) pediatric listserv, and a call through a private social media group, composed of pediatric physiatrists across the nation. A total of 84 pediatric IPRs were identified to target the survey. Thirteen of the 84 potential programs were excluded as no valid email address for communication was found nor did all the programs have an inpatient service at the time of inquiry. As such, 71 surveys were distributed in total (Fig. 1). An online survey using SurveyMonkey software was emailed to medical directors and pediatric IPR practicing physicians through methods above in December 2018. These directors or physicians self-identified as having experience with and information on IPR to complete the survey. One email reminder was sent to improve response rate. Returned surveys were collected from December 2018 to March 2019.
Subject recruitment through survey administration from December 2018 to March 2019.
Informed consent was obtained as part of the online survey and responses were recorded for data collection. Investigators assured one response per program or unit. The survey queried respondents on demographic information, practice type, location, and program characteristics including admission criteria, staffing, services, and programs offered.
Statistical analysis
Incomplete surveys were excluded from analysis. Detailed descriptive statistics were performed for each survey question. Analysis was divided into the following sections: response rate, distribution –geographic and location, admission criteria and authorization, and program characteristics from documentation to medical staff.
Results
Response rate
Between December 2018 to March 2019, 71 surveys were distributed, and 53 respondents opened the survey link (Fig. 1). Fifty individuals completed the survey yielding a 70.4% response rate. There were no duplicate respondents as such these responses reflect input from 50 unique pediatric IPRs. Three program responses were excluded due to incomplete data. Of the 50 responders, 35 (70%) were from the Medical Director of the program.
Distribution of pediatric inpatient rehabilitation programs
No surveys were provided to potential respondents in the following seventeen states as no pediatric inpatient rehabilitation services were identified during the survey collection period including: Alaska, Nevada, Idaho, Montana, Wyoming, North Dakota, Nebraska, Iowa, Kansas, Mississippi, Tennessee, West Virginia, Connecticut, Rhode Island, Vermont, New Hampshire, and Maine (Fig. 2). A large number of states (46%) offered one to two pediatric rehabilitation programs. There were 10 states with more than three programs including California, Texas, Minnesota, Illinois, Michigan, Ohio, Florida, Pennsylvania, New York, and Maryland.
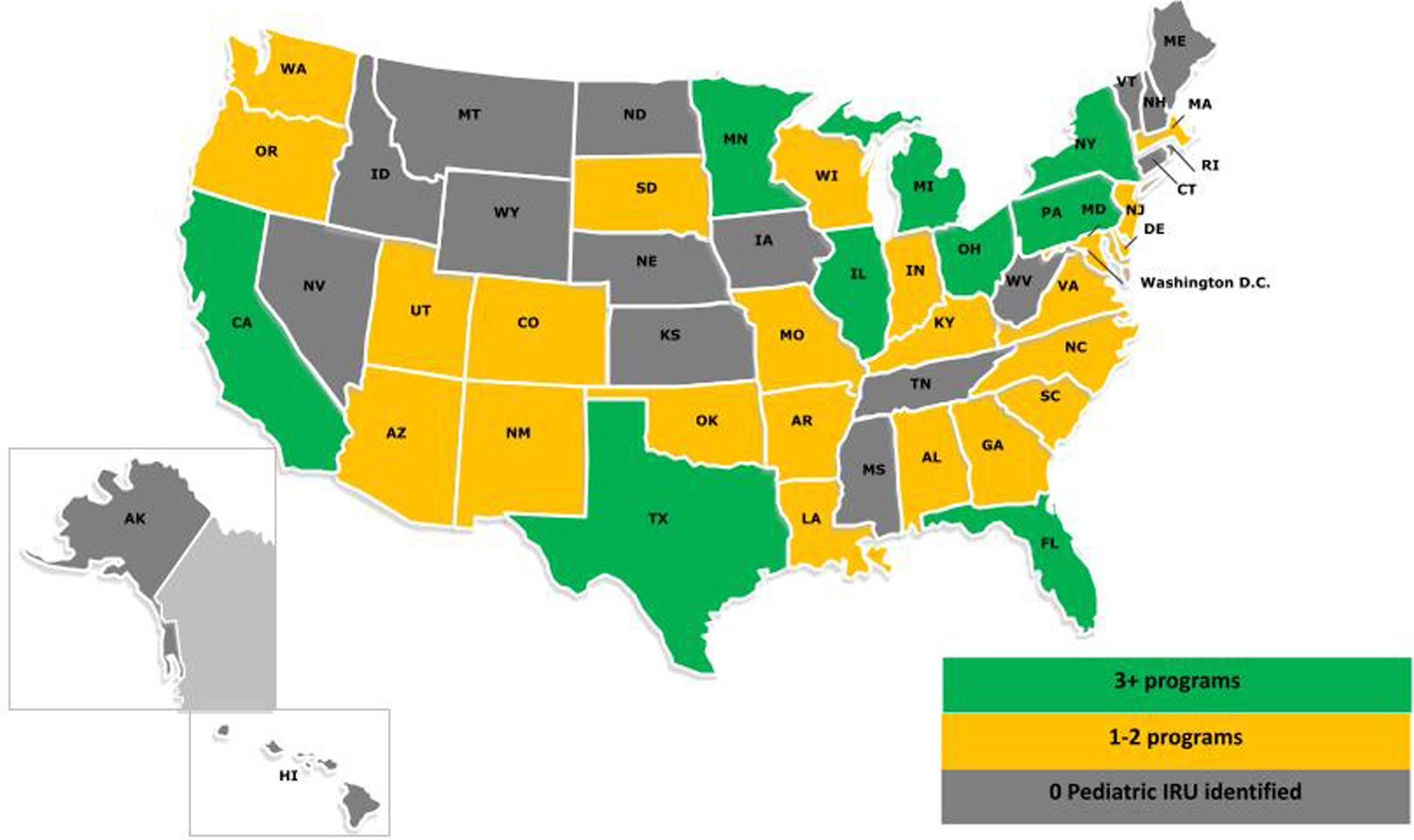
Distribution of Pediatric inpatient rehabilitation services across the United States.
A total of 50 programs providing pediatric rehabilitation services were identified. Of those pediatric rehabilitation programs surveyed, 50% were located within a free-standing pediatric hospital while 24% described their unit as a pediatric rehabilitation service with no distinct pediatric rehabilitation beds within a free-standing pediatric hospital (Table 1). Seven respondents (14%) described their IPR as being within a free-standing pediatric rehabilitation hospital. Fifty-six percent of respondents offered only acute IPR while 24% report offering acute inpatient and day rehabilitation programs. Ten programs (20%) offered subacute inpatient rehabilitation services as well with a few offering day programs and long-term acute care (LTAC) services.
Pediatric Inpatient Rehabilitation Programs (IPRs) – location and program characteristics
Program characteristics
An overwhelming majority (86%) of programs utilized the recommendation of a pediatric physiatrist with insurance approval alone, as main criteria for admission into IPR (Table 2). Twenty of the remaining programs used the recommendation of a pediatric physiatrist in adjunct with either CMS criteria, institutional criteria, institutional guidelines similar to CMS, or InterQual criteria. In terms of timing for insurance pre-authorization, the majority of programs reported requiring 24 to 48 hours (28% and 48%, respectively). Only one program described pre-authorization or approval provided in less than 24 hours. On average, respondents collectively reported a mean of 3% of patients admitted from external referral sources, with an average 14 beds available and a daily census of up to 9.92 patients (Table 1). Once admitted, most of the programs (80%) identified a pediatric physiatrist as the admitting physician. Some programs (16%) reported having a pediatric hospitalist as the admitting physician while only 4% of programs use non-pediatric certified or eligible physiatrists.
Admission Criteria utilized by pediatric IPRs
Admission Criteria utilized by pediatric IPRs
Variation exists among programs with respect to documentation criteria. Sixty percent of programs either use CMS criteria or institutional guidelines similar to CMS for documentation and management, of which documentation by the physiatrist accounts for face-to-face requirements. Only three (6%) of the programs utilized InterQual Criteria, with two of the three utilizing them along with CMS or institutional criteria [1].
A large majority (82%) of programs utilized the WeeFIM as the sole (56%), or among a series of, standard outcome measures selected by the respondents for the pediatric IPR (Table 3). Other clinical outcome measures used alongside the WeeFIM included the Pediatric Evaluation of Disability Inventory (PEDI), Bruininks-Oseretsky Test of Motor Proficiency Second Edition (BOT-2), Six Minute Walk test (6MWT), or the Visual Motor Integration (VMI). Sixty-six percent of programs submit their data to the Uniform Data System for Medical Rehabilitation (UDSMR) (Table 3). The remaining programs use outcomes data for other purposes such as functional documentation to assist in insurance coverage for admission or internal quality surveillance.
Standard outcome measures
Standard outcome measures
Twenty-four programs (48%) reported being CARF-accredited as a Pediatric Specialty Program. Ten of those CARF-accredited programs self-reported having additional CARF certifications for additional specialty programs, such as: Brain Injury, Spinal Cord Injury, Pain or Cancer Rehabilitation. Additional specialty population programs (non-CARF certifiable) included: disorders of consciousness, feeding, functional neurological disorder, complex medical care, selective dorsal rhizotomy or congenital heart disease (Table 4).
CARF-accredited specialty programs
All programs had core members including pediatric physiatry, nursing, and the essential therapy services including physical, occupational, and speech therapy along with a social worker and/or case manager. Nineteen (38%) included a pediatric hospitalist as a part of the core medical team. Only six programs (12%) reported having their own dietitian. An overwhelming majority (92%) reported staffing with a behavioral and/or neuropsychologist. The presence of a school re-entry coordinator or teacher as a member of the rehabilitation team was reported in 36 (72%) of programs. Although 36 programs (72%) also included a recreational therapist, only 15 (30%) had an established child life specialist.
Of the 28 programs which reported using an advanced practice provider (APP), only five require APPs to have a Certification in Rehabilitation Nursing (Table 5). Twenty-two (73.3%) of programs noted APPs’ role in the IPRs is to “co-manage patients (rounds and assist with documentation)” while two programs reported them working independently with distant supervision. An additional two programs reported minimal rehabilitation roles for APPs, who instead worked primarily in comanaging patients in the program under pediatric hospitalist supervision.
Advanced practice providers in Pediatric IPRs
Advanced practice providers in Pediatric IPRs
Only 16% of programs reported no trainees assisting with daytime patient management while a majority of programs (74%) involved PM&R residents or fellowship trainees at the least; fellows assisting including Pediatric Rehabilitation, Neurodevelopmental Pediatric, and Child Psychiatry fellows. Ten programs involved both PM&R residents and pediatric PM&R fellows-in-training. Five programs reported involvement of pediatric rehabilitation residents alone while 11 involved pediatric residents alongside PM&R residents or fellows. A few pediatric IPR providers reported the presence of developmental pediatric or child neurology fellows as well. Most programs (66%) have 24-hour medical coverage, seven days a week with staffing by physicians only (upper level resident, fellow, or attending). Seventeen programs (34%) reported medical coverage by a combination of physician and APPs. Only one program of those surveyed reported no 24-hour medical coverage.
The preparation of this survey assisted in the understanding of geographical location of most pediatric acute IPRs, with a total of 71 programs identified. It had an excellent response rate with 70% of identified programs completing the survey. Among the programs that self-identified as offering inpatient rehabilitation services, most use specific criteria to admit patients to the IPRs with insurance authorization obtained within 24 to 48 hours. Most teams reported similar composition, with the majority having a pediatric physiatrist, in addition to staff from physical therapy, occupational therapy, speech therapy, nursing, and a social worker or case manager to assist with care coordination. Even though there may be similar constructs amongst programs, this does not lend to similar roles among team members. Social workers may provide support for the family’s psychosocial concerns, including emotional wellbeing or identification of community resources in a program, while in others, this team member may assist with coordination of care for discharge or school re-entry efforts. Given this is the first time this survey was compiled, how roles may differ across different programs and institutions was not explored. Role expectation, delineation of responsibilities, and financial considerations for these roles should be further explored in future work.
Most pediatric IPRs reported having trainees involved in the care of patients. The rehabilitation program trainees included PM&R residents, combined pediatric rehabilitation residents, or pediatric rehabilitation medicine fellows. Some programs also provided opportunities for other non-rehabilitation graduate medical education (GME) trainees. Therefore, it could be assumed that most queried programs have direct academic affiliations; however, the survey did not directly address the presence of other trainees in this setting, such as medical, nursing, or other students or trainees. This should be explored in future studies to better understand which ancillary services receive training exposure in the care of this unique patient population.
Close to half of the IPRs have CARF accreditation for a pediatric specialty program. CARF accreditation may be pursued to highlight the program’s mission to stay current in the provision of rehabilitation care. It promotes continuous optimization of outcomes and quality improvement for programs [3].
The majority of programs use CMS standard-guided criteria for daily and programmatic documentation. A pediatric physiatrist provides face-to-face documentation regarding provision of medical care of the patients in the majority of those surveyed. Even though there are no mandated national clinical outcomes or database repositories, the majority of programs reported using at least one clinical outcome measure. The WeeFIM was the most common reported measure being used by programs across the country, with the majority reporting it to UDSMR (private national data repository). However, most programs identified additional clinical measures being used in their programs. National standardization and data repositories may assist in the creation of a structure to further explore the clinical outcomes and value of IPRs for the pediatric population.
Even though most programs obtain insurance authorization within 24 to 48 hours, the survey did not include questions regarding reimbursement or payor sources. Thus, there may be opportunities to understand the fiscal environment of IPRs. Having a national database may assist in comparing if there are regional differences for reimbursement, provision of care, or patient and family demographics. The analysis did not compare programs that are located in free standing rehabilitation facilities or pediatric specialty hospitals from those located within pediatric hospitals, given the limited number of responses obtained from the latter. Seventeen states, mostly located in the north/north central parts of the country, had no identifiable IPRs. Further investigation is also warranted to discern the impact that ethnicity and racial factors may have on access to acute IPRs. Previous studies have shown that non-Hispanic Blacks and Latinx or Hispanic patients are less likely to be referred or receive post-acute rehabilitation services [4–6].
Limitations
There is the potential that some programs were not identified or unreachable since there is no national database for post-acute pediatric medical services, and less so for pediatric IPRs. A commentary published in 2015 by O’Brien et al. identified approximately 145 embedded rehabilitation units within acute pediatric hospitals across the US per information provided by hospital websites, Children’s Hospital Association listings, and state hospital licensure websites [7]. Therefore, the correct number of programs across the country is unknown. The results in the presented survey are also limited by respondents’ knowledge themselves regarding program details. Other limiting factors indicate that some of these IPRs may be currently covered by other providers who are not pediatric physiatrists and may include adult physiatrists, neurologists, independent APPs, or pediatricians. This project attempted to identify the most qualified providers for the completion of the survey, as there may be additional concerns if hospitals are advertising or offering inpatient rehabilitation programs or services without the leadership of qualified pediatric physiatrists to direct its provision of care.
Conclusions
Pediatric IPRs across the US are quite varied, yet have some similar programmatic characteristics. Team composition, clinical coverage, insurance authorization, payor mix, accreditations/certifications for specialty programming may be dependent on location, institution and regional culture. This study has introduced the importance of attempting to understand these factors in order to be able to develop accessible and equitable programs across the nation. Significant underserved areas were identified, which may impact the ability for patients to obtain rehabilitation care that they require. Additional research is needed to identify standards of practice, clinical, and fiscal characteristics. A National data repository could identify how program location affects available resources, subsequent healthcare delivery, and long-term outcomes with the goal of equitable provision of care.
Footnotes
Acknowledgments
The authors thank the UTHealth McGovern Medical School, Department of Physical Medicine and Rehabilitation for their support. The authors have no conflict of interest to report.
Funding
No funding was received to complete any portion of this study.