
Abstract
An aneurysmal bone cyst (ABC) is a benign lesion often found in long bones. Almost one third of ABCs are secondary to primary tumors. When found in the spine, ABCs can cause insidious back pain and, in rare cases, neurological deficits. This case will discuss an adolescent female who acquired a non-traumatic spinal cord injury (NTSCI) as a result of complications from an aneurysmal bone cyst. Treatment consisted of surgical removal of the cyst, laminectomy, corpectomy, and fusion of the thoracic spine. Following surgical intervention, the child spent several weeks in an acute inpatient pediatric rehabilitation facility. Goal oriented outpatient services facilitated further recovery and led to near complete resolution of symptoms associated with non-traumatic spinal cord injury. Contemporary and clinically oriented child and family interventions are essential in successful rehabilitation of children with NTSCI as a result of ABCs.
Keywords
Introduction
In the general pediatric population, low back pain is an uncommon complaint that always needs to be taken seriously. Adolescents engaged in competitive sports are prone to develop low back injuries more frequently [1]. Common reasons for back pain in adolescent athletes are spondylolysis, spondylolisthesis, disc degeneration or stress reaction of the epiphysis [1]. A less common etiology of acute lower back pain with neurologic symptoms is an aneurysmal bone cyst. The World Health Organization describes an aneurysmal bone cyst (ABC) as an expanding lesion with blood filled cavities separated by septa of trabecular bone or fibrous tissue containing osteoclast giant cells. ABCs are classified as benign solid bone tumors and can involve the long bones (humerus, tibia), hands, feet and vertebral bodies of the spine [2]. In this case we will discuss the clinical significance and rehabilitation of an adolescent with nontraumatic spinal cord injury (NTSCI) following development of acute low back pain secondary to an aneurysmal bone cyst.
Case report
This is a case of a previously healthy 13-year-old female athlete who reported development of acute back pain with rapid progression of lower extremity weakness. One week prior to presentation to the emergency room, the child had developed left shoulder and upper back pain that was attributed to muscle strain related to playing volleyball. The primary care physician prescribed anti-inflammatory cream, which provided minimal relief.
On the morning the child presented to the emergency room she attempted to get out of bed and her legs gave out beneath her. The onset of lower extremity weakness was described as a “jolt of pain” with subsequent progression of numbness and tingling from the mid-chest level to bilateral feet. Following initial evaluation in a major tertiary academic emergency room the decision was made to obtain an MRI scan of the spine.
a. T2 sagittal view of a pathologic T4 vertebral body compression fracture with retropulsion resulting in severe cord compression and a large presumed aneurysmal bone cyst within the T4 vertebral body extending into the posterior elements. b. axial view of the aneurysmal bone cyst at T4.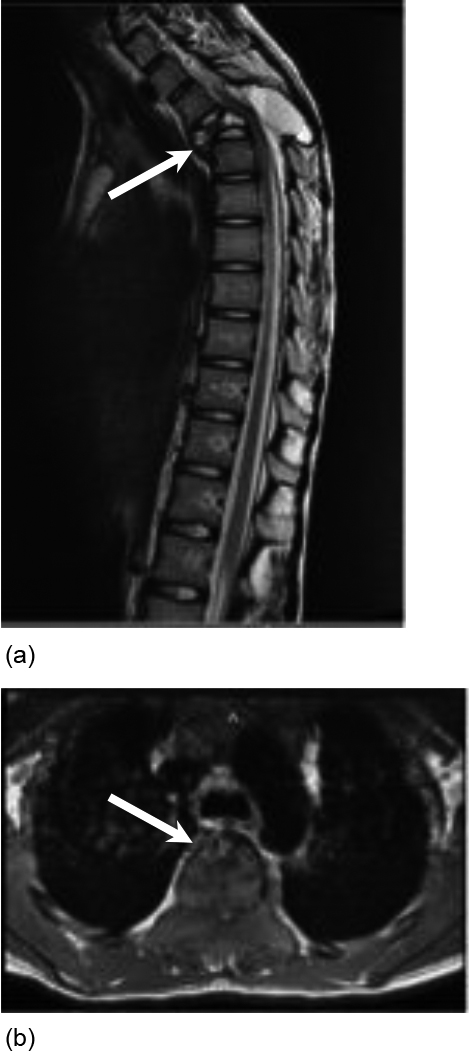
MRI spine showed a “pathologic T4 compression fracture with retropulsion resulting in severe spinal cord compression and a large presumed aneurysmal bone cyst within the T4 vertebral body extending into the posterior elements” (Fig. 1a and b). The child underwent two surgical procedures: laminectomy of T4 and fusion of T1-T7 vertebrae followed by T4 corpectomy one week later (Fig. 2). Pathology report was consistent with an aneurysmal bone cyst. Repeat MRI obtained one week after the second procedure demonstrated “T2 hyperintensity in the central cord from T3-T5” that was reported as “infarction, edema, or developing myelomalacia” Once medically stabilized the child was transferred to a pediatric acute inpatient rehabilitation facility to address new functional deficits due to the incomplete NTSCI.
Status post T4 laminectomy and transpedicular partial corpectomy for tumor resection with T1-7 instrumented fusion.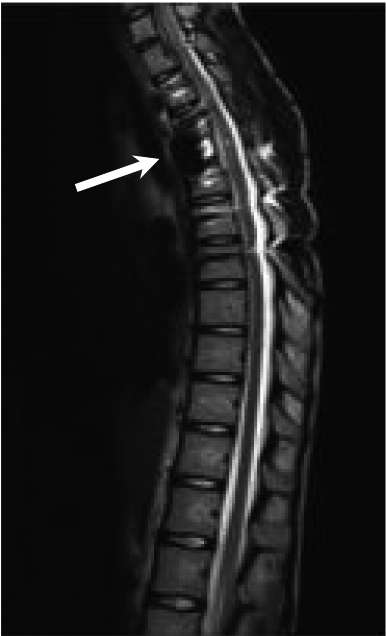
Upon admission to the acute inpatient rehabilitation unit, clinical examination yielded impaired sensation to pinprick and light touch below the dermatome of T4, and weakness in both lower extremities. This was consistent with sensory and motor incomplete paraplegia with neurologic level of T4. It was apparent the child exhibited a significant decline in function requiring maximum assistance with sitting balance, moderate to maximum assistance with bed mobility, and total assistance with transfers. The child did not have sensation in the perineal region and was incontinent with both bowel and bladder functions.
Structured daily rehabilitative interventions and clinical management within the framework of the acute pediatric inpatient rehabilitation unit led to improvements in the clinical, functional and psychological well-being of this child during the admission. Bladder continence was restored with clean intermittent catheterization and a bowel program was utilized to decrease bowel accidents. Introduction of the robotic body-weight-supported treadmill training early in her rehabilitation course proved to be beneficial in restoring her ambulation. Upon discharge to home, the child’s sensation was intact to light touch as well as pinprick sensation throughout the body, and strength was 5/5 in both lower extremities with the exception of 4/5 hip flexion strength. Activities of daily living including toileting and bed mobility were at an independent level. The child still required some supervision with transfers but was able to ambulate up to 150 feet using a unilateral forearm crutch.
Bowel and bladder activities were restored to the extent that the child did not have episodes of incontinence during therapy sessions or at night. She successfully returned to school full time four months after her injury with no signs of cyst recurrence on postoperative imaging. With continued outpatient therapies, the child was able to ambulate independently. Within 6 months of the injury the child had full neurologic recovery in both sensory and motor functions. She eventually regained full bladder control and had spontaneous bowel movements with rare use of stool softeners to prevent straining.
When present in the spine, aneurysmal bone cysts are most commonly seen in the lumbar, cervical and thoracic spine (in descending frequency). It is difficult to determine the incidence because it is often undetected if asymptomatic [2]. On MRI imaging the cysts are usually located in the metaphyseal part of the bone with radiolucent, dilated fluidfilled characteristics [3]. Although most are benign, up to 30% of ABCs can be secondary to other primary tumors such as giant cell tumors, fibrous dysplasia and chondroblastoma [4].
Aneurysmal bone cysts are classified in many different ways. One type of classification was described by Capanna et al who categorized ABCs into 5 different subgroups [5]:
Type 1 (Central) – well contained lesions, minimal or no expanded outline Type 2 – involves entire bony segment with marked expansion and cortical thinning Type 3 - only involves one metaphyseal cortex eccentrically Type 4 – subperiosteal lesions that expand away from bone (least common) Type 5 – located in periosteum and expand peripherally with cortical erosion.
Another classification is the Ennking classification which consists of 3 different subtypes [5]:
Stage 1 (latent) – remains static or heals spontaneously, minimal inflammation or periosteal reaction. Stage 2 (active) – progressive growth but no cortical destruction. Stage 3 cysts – locally aggressive/rapidly expanding cysts with no significant cortical destruction.
Common symptoms of an aneurysmal bone cyst include insidious back pain with or without a pathologic fracture. The mean age of presentation for ABC is 13 years old and they are more commonly seen in females. Although rare, it can cause neurological complications when in close proximity to exiting nerve roots or the spinal cord. Current treatment is removal of the cyst with or without bone grafting. Other treatment modalities include radiation therapy, sclerotherapy, arterial embolization, bisphosphonates or monoclonal antibodies [4].
Prior studies have emphasized that comprehensive inpatient rehabilitation is still an essential part of recovery for a non-traumatic spinal cord injury (NTSCI) [6]. These patients are more likely to have less severe, incomplete paraplegia when compared to spinal cord injuries from a traumatic etiology [7]. These patients also tend to have similar Functional Independence Measure (FIM) efficiency scores and likelihood of discharge to home while having a shorter length of stay when compared to traumatic spinal cord patients [6]. While in an inpatient rehabilitation facility, patients with NTSCI learn to manage neurogenic bladder, neurogenic bowel, spasticity and prevent the development of pressure ulcers [7]. A longterm factor that must be monitored in children with spinal cord injuries is the likelihood of scoliosis, especially if the injury happened before the age of 12 years [8].
With stabilization of her spine and a multidisciplinary team in the acute inpatient rehabilitation setting, the child was able to make a remarkable recovery. The etiology and likelihood of recurrence of the child’s aneurysmal bone cyst still remains unclear. A large part of her recovery was her social support and internal motivation. A year after the injury, she continued to participate in outpatient therapies including robotic locomotor training and wholebody vibration. Studies have shown that along with helping to restore ambulation, locomotor training can improve quality of life, bone density and bowel and bladder continence in children with spinal cord injuries [9]. Wholebody vibration is another modality that can be introduced into the rehabilitation treatment plan for patients with spinal cord injuries to increase blood flow to the lower extremities [10].
Unfortunately, the child has not returned to playing volleyball, and there is little evidence regarding recommendations to return to contact sports after thoracic spinal cord injury with instrumentation.
Conclusion
Aneurysmal bone cysts, although rare, should be included in the differential diagnosis if acute neurological changes are present with complaints of acute back pain. In the event that an aneurysmal bone cyst causes non-traumatic spinal cord injury, neurosurgical intervention, a comprehensive rehabilitation team and strong social support can be essential for recovery and reintegration into the community.
Footnotes
Acknowledgments
None.
Conflict of interest
The authors have no conflicts of interest to report.