
Abstract
PURPOSE:
Arteriovenous malformation (AVM) rupture in children can cause debilitating neurological injury. Rehabilitation is key to recovery, though literature details little regarding rehabilitation outcomes. We examined a single-center experience with pediatric AVMs as related to acute inpatient rehabilitation outcomes.
METHODS:
At our institution, a retrospective chart review was completed examining all cases of intracranial AVMs in patients age 18 and younger who completed our acute inpatient rehabilitation program between 2012–2018. Patient characteristics, clinical data, treatment modality, and functional outcomes were reviewed.
RESULTS:
14 patients with AVMs underwent acute inpatient rehabilitation; nine (64.3%) treated
surgically at our institution, two (14.3%) non-surgically at our institution, and three
(21.4%) surgically at an outside facility prior to transitioning care at our
institution. Eight (57.1%) were male, seven (50.0%) Caucasian, and seven (50.0%)
Hispanic. Seven (50.0%) presented with AVM rupture; six (42.9%) were found incidentally
on imaging. Clinical courses, treatment outcomes, and post-treatment complications
varied. Several patients underwent repeat treatment or additional procedures.
Neurological deficits identified included hemiparesis, dystonia, spasticity, epilepsy,
hydrocephalus, and ataxia. Inpatient rehabilitation unit length of stay was on average
21 days (SD 9.02, range 9–41). Functional Independence Measure for Children
(WeeFIM
CONCLUSION:
We found that all pediatric patients with intracranial AVMs, across all treatment modalities, demonstrated improved outcomes across all functional domains after an acute inpatient rehabilitation program.
Keywords
Introduction
Arteriovenous malformations (AVMs) are congenital vascular anomalies composed of a mass of abnormal veins and arteries linked by one or more fistulas [1]. In the pediatric population, AVMs are the most common cause of spontaneous intracranial hemorrhage (ICH) and account for about half of all pediatric hemorrhagic strokes [2]. AVMs carry an overall annual risk of rupture of three percent, with an increased risk of hemorrhage among previously ruptured AVMs [3]. AVM rupture is associated with high mortality and morbidity including long-term impairment in mobility, speech, cognition, neurological development and functional ability, with half of patients identifying cognitive issues [4]. It is hypothesized that blood products in the brain parenchyma after AVM rupture are cytotoxic, resulting in changes in previously functional tissue, affecting it and surrounding tissue through inflammatory pathways [5].
Unruptured AVMs have also been associated with impairments in cognition, including attention, memory, learning, and verbal and visuospatial intelligen-ce [6], with two-thirds of adult patients with AVMs reporting difficulty in cognitive skill during their school years [7]. One theory explaining the association between AVMs and cognitive impairment regards mass effect on the surrounding tissue causing changes in its function and viability [8]. Additionally, cerebrovascular steal syndrome, where the demand of the high-flow AVM diverts cerebral blood flow from adjacent parenchyma toward the AVM, has been theorized as a cause, whereby decreased cerebral perfusion pressure leads to ischemia of the tissue adjacent to the AVM [8]. Additionally, hypoxic and ischemic changes due to lesional flow dynamics, treatment changes, or hemodynamic variations related to anesthesia during treatment may also impact surrounding brain parenchyma. This can possibly result in mild, clinically inconsequential changes to surrounding brain tissue after resection or in a devastating stroke syndrome if aberrant AVM vessels incorporate important neurovascular structures which treatment compromises.
Regardless of mechanism, both ruptured and unruptured AVMs can greatly affect a developing brain, resulting in significant impacts in normal brain development with important neurological sequelae. A small case series looking at five children with treated AVMs in various intracranial locations demonstrated the impact of AVM in executive functioning and neuropsychological outcomes regardless of location, which suggests AVM disruption of subcortical pathways and the potential role of neural plasticity in pediatric AVM recovery [9]. While intensive therapy is often presumed to help treat and is prescribed following diagnosis and treatment of AVM, there is a dearth of literature understanding the supportive role of acute inpatient rehabilitation following AVM treatment or rupture. One study compared language outcomes in pediatric patients after traumatic brain injury (TBI) or AVM rupture who were treated in an inpatient rehabilitation setting. In addition, patients in the AVM cohort were seen to have worse deficits in terms of working memory, fluency, and aphasia, identifying them as vulnerable populations with much potential for improvement [10]. A recent retrospective case series of 25 children treated for intracranial AVMs explored functional and education outcomes at discharge and long-term follow-up (mean 11.5 years, SD 5.3, range 4.1–24.4); they found positive outcomes, with 23 children enrolled in regular education programs, all with stable or improved functional outcomes, defined by modified Rankin Score, compared to discharge [11]. However, while the patients in this cohort had access to rehabilitative services in this study, they did not have a standardized rehabilitation protocol or inpatient rehabilitation admission.
Rehabilitation has been shown to decrease the morbidity and improve functional outcomes following ischemic stroke and other types of neurological injury [12]. However, there is a paucity of data examining the role of acute inpatient rehabilitation in pediatric patients with intracranial AVMs. Thus, in this population there is a need to examine the impact of rehabilitation on cognitive, motor, and functional outcomes. Better understanding of the impact of rehabilitation can quantify and define the need and role for acute inpatient rehabilitation, as well as identify areas where therapy and recovery can be tailored to better improve the outcomes of pediatric patients with AVMs. This study sought to examine the functional outcomes of pediatric patients undergoing acute inpatient rehabilitation in conjunction with AVM treatment.
Methods
At our institution between 2005–2018, a retrospective chart review was completed examining all cases of intracranial AVMs in patients age 18 and younger. Of the 105 patients identified with this diagnosis, 14 participated in inpatient rehabilitation in conjunction with brain AVM-related needs, after our inpatient rehabilitation unit was opened in 2012. Patients were included if there was an acute inpatient rehabilitation unit (IRU) admission documented.
Candidacy for IRU admission was evaluated by the admitting IRU physician based on the patient’s ability to participate and engage in three hours of acute inpatient rehabilitation daily. All patients were evaluated by Physical Medicine and Rehabilitation physicians and Physical Therapy, Occupational Therapy, and Speech and Language Pathology therapists prior to selection for IRU admission. The acute IRU at our institution consists of a comprehensive, integrated rehabilitation experience that involves pediatric physiatrists/psychologists, physical therapists, occupational therapists, speech and language pathologists, rehabilitation certified nurses, dedicated social workers and case managers, child life specialists, recreational therapists, pet therapists, and many more. Each participant receives an average of three hours of therapy a day. The IRU is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF).
Cases were reviewed in detail to explore preoperative assessment, AVM characteristics, radiographic findings, treatment modality, and outcomes, including postoperative functional and rehabilitation data. Demographics collected included age, race/ethnicity, sex, etiology of presentation, and symptoms at presentation. Clinical data regarding AVM laterality, location, feeding arteries, nidus size, and grade were examined. AVM grade was calculated using the Spetzler-Martin scale [13], a three-item grading scale ranging from I-V, which takes AVM characteristics, including size of nidus, eloquence of location, and venous drainage, into account to stratify risk of surgical resection. Grade I and II are considered low-grade and bear lower surgical risk, compared to higher-grade IV and V lesions. Additionally, we used the Lawton-Young supplementary score [14]. This score was developed to improve patient selection for surgical intervention and considers additional variables to the Spetzler-Martin score, including age, hemorrhage at presentation, and diffuseness of nidus. Higher Lawton-Young scores portend higher incidence of adverse outcomes from surgery.
Functional outcomes were assessed using the Functional Independence Measure for
Children (WeeFIM
Data were evaluated using descriptive statistics. This retrospective study was conducted under Institutional Review Board approval.
Results
Of 105 patients with the diagnosis of brain AVMs, 14 were identified to have participated in inpatient rehabilitation at our institution. Nine (64.3%) underwent surgical treatment of AVMs, two (14.3%) were treated non-surgically, and three (21.4%) were treated surgically at an outside facility prior to transfer of care. Eight (57.1%) were male, seven (50.0%) Caucasian, and seven (50.0%) Hispanic. Seven (50.0%) presented with AVM rupture; six (42.9%) were found incidentally on imaging. Most common presenting symptoms included headache and weakness; others were not clinically symptomatic prior to treatment (Table 1). One patient treated non-surgically had three years of symptoms and presented with progressive dystonia.
Patient demographics per treatment group
Patient demographics per treatment group
Preoperative assessment and work-up included cranial and cerebrovascular imaging. Radiological evaluation demonstrated a variety of AVM pathology. Lesions were both right and left sided, located in various lobes of the brain, classified as a range of low and high grade, with an average of one to two feeding vessels, and with AVM nidus size ranging from less than 1 to 6 centimeters (Table 2). Figure 1 depicts an imaging example of a patient included in our study, who presented with rupture and was treated surgically.
Arteriovenous malformation characteristics per treatment group
cm
Case example of a ruptured pediatric arteriovenous malformation. A) Computed
tomography (CT) head image of a 12-year-old female with right parietal intracranial
hemorrhage (ICH). B) CT Angiogram Brain of a 12-year-old female with ruptured right
parietal arteriovenous malformation. C) Diagnostic Cerebral Angiogram, right carotid
artery injection demonstrating a right parietal arteriovenous malformation in a
12-year-old female presenting with rupture. D) Interval Diagnostic Cerebral Angiogram,
right carotid artery injection demonstrating no residual right parietal arteriovenous
malformation post-operatively.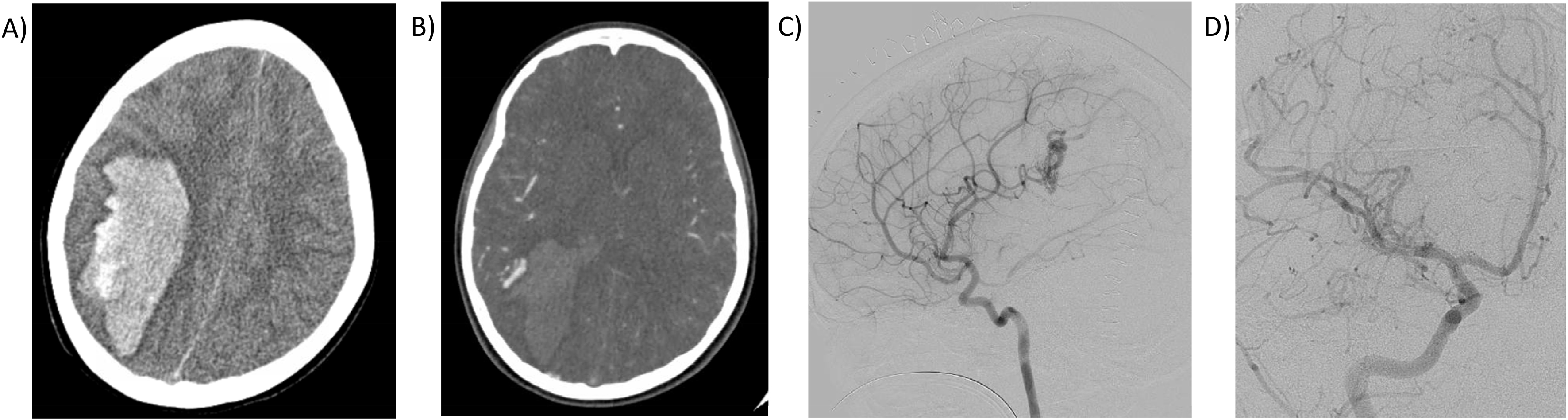
Of the nine cases treated surgically, four underwent preoperative embolization, one of which included four staged treatments. Eight (88.9%) patients had complete resection. Complications included wound infection requiring wound revision, hemiparesis, and bone flap resorption requiring cranioplasty; rarer neurological sequela included spasticity, dystonia, epilepsy, ataxia and hydrocephalus. Postoperative deficits included hemiparesis and/or ataxia in a third of patients treated surgically. Three of the nine cases required additional surgery for residual or recurrent AVM; two underwent repeat craniotomies and the other underwent stereotactic radiosurgery. Radiographically, eight (88.9%) had complete obliteration of AVM at last follow-up. Six of the nine patients had additional neurosurgical procedures, the most common being decompressive craniectomy, hematoma evacuation, and/or external ventricular drain placement, which often are the first lines of treatment for acutely ill neurosurgery patients requiring treatment of elevated intracranial pressure, cerebral edema, and mass effect; others included the wound revision and cranioplasty as aforementioned.
Rehabilitation outcomes
WeeFIM
Of the two cases treated non-surgically, one underwent embolization while one underwent serial radiographic surveillance. The one treated endovascularly had complete treatment of lesion in one stage, complicated by hemorrhage which required craniotomy for hematoma evacuation and external ventricular drain placement. Interval imaging one month after presentation demonstrated small residual AVM which is currently being managed conservatively with observation. The one case treated with serial surveillance was a high-grade lesion in the basal ganglia and thalamus presenting with 3 years of dystonia; over time that patient developed obstructive hydrocephalus related to the lesion and was subsequently shunted. The lesion has remained unruptured for the duration of follow-up.
The three cases seen at outside facilities prior to transfer to our institution were treated surgically, none of which were reported to have had preoperative embolization. As surgery and preoperative work-up was completed at an outside institution, the records for two cases were incomplete with some unknown variables. Postoperative complications in this cohort included hypoxic injury, malignant cerebral edema, infection, resorbed bone flap, and hydrocephalus. All had additional procedures, including external ventricular drain placement, craniectomy, cranioplasty, and ventriculoperitoneal shunt. Two of the three cases had no residual or recurrent AVM; one underwent repeat craniotomy for recurrent AVM at our institution one year after initial surgery. Neurological deficits in this cohort included paresis (hemiparesis and quadriparesis in two patients respectively), dystonia, epilepsy, and spasticity.
All patients in this study participated in an acute inpatient rehabilitation
program to address functional deficits associated with their AVM. Most participated after
AVM rupture and/or AVM surgery; however, one was admitted after AVM rupture but prior to AVM
resection surgery and another was admitted with no history of rupture treated conservatively
but had progressive dystonia related to lesion. IRU lengths of stay (LOS) ranged from 9 to
41 days (mean 21, SD 9.02). All WeeFIM
We found improvement in functional outcomes, including self-care, mobility, and cognitive outcomes, after inpatient rehabilitation admission in pediatric patients with intracranial AVMs. Additionally, our findings and treatment outcomes are congruent with the literature demonstrating similar cure rates with surgical and endovascular management [19, 20, 21, 22] as well as similar types of complications [19, 20, 22].
The main aim of this study was to fill a void in the literature regarding the
role of acute inpatient rehabilitation in pediatric patients after intracranial AVM rupture
and/or treatment. Rehabilitation interventions for acquired brain injury, particularly in
children, are thought to improve functional outcomes by facilitating the retention of spare
neural pathways to compensate for pathways damaged by disease [23]. In a large study of rehabilitation for acute ischemic stroke
which examined over 100,000 patients across more than 800 hospitals, between 56 to 71
percent of patients experienced improvement in activities of daily living [24]. In pediatric patients undergoing AVM treatment,
rehabilitation has not been studied despite a reported 40 percent of patients with AVMs
discharged to a rehabilitation facility [25]. Most
patients discharged to a rehabilitation facility are those who present with more severe
neurologic impairment and disability at admission (National Institutes of Health Stroke
Scale
In this study, the Functional Independence Measure for Children
(WeeFIM
All 14 of the participants in this study had improvement in their self-care,
mobility, and cognitive scores from acute inpatient rehabilitation admission to discharge,
regardless of surgical treatment, conservative management, or treatment at another facility.
The greatest improvements in WeeFIM
WeeFIM
This study provides evidence supporting the role of acute inpatient rehabilitation for pediatric patients undergoing treatment of intracranial AVMs. With improvement in overall functional outcomes in the areas of motor, speech, and cognition, acute inpatient rehabilitation demonstrates substantial improvement in outcomes. The greatest improvement was seen in self-care measures, demonstrating the role of inpatient rehabilitation in improving functionality and independence. This is in conjunction with our finding of post-rehabilitation mean mRS of 0.33 in the surgically treated group and 1 in the non-surgically treated group, signifying functional independence (mRS 0–2). While mobility and cognitive scores increased robustly in the surgical group, for those treated non-surgically, less improvements were seen. This suggests possible improved neural plasticity and recovery in this population, such that after surgical resection of the offending lesion, the remaining healthy brain tissue may recover and result in improved function, perhaps from less compressive or steal-inducing pathology. Conversely, those treated conservatively or with endovascular intervention had less recovery, perhaps due to persistent mass effect from the lesion or residual disease with altered blood flow and brain mechanics. While the exact mechanism underlying changes in brain tissue following treatment remains unknown, future study may glean biochemical, mechanical, and molecular changes that may contribute to recovery.
Overall, our findings support the implementation of acute intensive inpatient rehabilitation in children suffering from intracranial AVMs. Most specifically, those undergoing surgical resection of pediatric AVM may be the most likely to benefit from acute rehabilitative therapies. Aiming to promote access to care, barriers such as location and costs of care should be considered. The overall cost of pediatric stroke care is high, with median cost of care for 1 year at $42,338; the costs are even higher for hemorrhagic stroke with average inpatient costs close to $50,000 [30]. Additionally, the average published cost per day of inpatient admission for rehabilitation is around $1,600 [31]. Despite perceived barriers like cost, intensive therapy can help limit long-term disability and has been shown in stroke to reduce overall costs over time [32]. As more becomes known about the role of inpatient rehabilitation in these patients, healthcare utilization and cost-related studies may shed further light on this impact.
Study limitations
Limitations of this study include the small sample size which limited the performance of analytic statistics to evaluate significance. Additionally, due to a retrospective design, this study was limited by observational data, precluding the ability to apply standardized treatment modalities, allowing for variation in physician practice preferences, and resulting in incomplete records for review from patients treated at outside facilities. Future prospective studies with larger patient populations and additional rehabilitation data, along with further exploring types of rehabilitation programs and specific models for neuro-recovery, may further delineate how populations can benefit in more specific ways from rehabilitation after AVM rupture and treatment.
Conclusions
To our knowledge, this is the first study exploring the role and results of acute inpatient rehabilitation in pediatric patients undergoing intracranial AVM treatment. The study identifies the impact of rehabilitation regarding neurological recovery and includes improvement in self-care, cognition, mobility, and functional independence. These findings support the role and implementation of intensive inpatient rehabilitation in those undergoing AVM treatment, namely surgical resection of pediatric intracranial AVMs.
Footnotes
Conflict of interest
The authors have no conflict of interest to report.