
Abstract
PURPOSE:
To determine if medical or functional factors influence the ability of a pediatric patient with a tracheostomy to tolerate decannulation.
METHODS:
Retrospective evaluation of patients at a tertiary Children’s Hospital undergoing evaluation with capped tracheostomy polysomnogram (cPSG) for possible tracheostomy decannulation. Charts were reviewed for demographic information, functional status, cPSG characteristics, and success or failure of decannulation. Statistical analysis was performed to determine which patient factors were predictive of successful decannulation.
RESULTS:
A total of 139 sleep studies were analyzed in 104 unique children followed for at least 1 year after a cPSG was performed to determine readiness for decannulation. At 1 year after most recent PSG, 79.8% of children were decannulated. There was no significant association between any single comorbid condition and the ability to decannulate. There was no association between individual or total functional status score and successful decannulation. Patients with at least 3 comorbid conditions investigated and a total functional score less than 7 were less likely to be decannulated successfully than other patients (71% vs. 93%,
CONCLUSION:
Functional status and comorbid conditions do not independently predict successful decannulation. Regular multi-disciplinary team reevaluation is indicated in patients with lower functional status, as removal of tracheostomy tube may be successfully accomplished.
Splaingard et al. functional status score [5]
Splaingard et al. functional status score [5]
Approximately 5,000 tracheostomies are performed annually in the United States in children [1]. The array of indications for tracheotomy underscores both the diversity of post-tracheotomy care and potential decannulation timelines in children. Determining readiness for tracheostomy decannulation is typically a multi-step process that can be assessed in an inpatient or outpatient setting. To predict the likelihood of successful decannulation, a variety of diagnostic procedures may be performed, including complete airway evaluation and capped tracheostomy polysomnogram (PSG) [2]. Several conditions or circumstances may prevent successful tracheostomy decannulation. Occult airway lesions like tracheostomal granuloma, tracheomalacia, vocal cord paralysis, and subglottic stenosis are the most common structural causes for inability to decannulate a child [3]. Additionally, increased oral and airway secretions and aspiration with impaired cough reflex can complicate attempts at decannulation. Knollman and colleagues recommend performing a routine endoscopic evaluation to detect structural airway problems prior to decannulation and polysomnography with a capped tracheostomy tube to detect obstructive sleep apnea or dynamic airway disease not detectable while awake. One day of inpatient observation after decannulation is frequently recommended to detect possible decannulation failures [4].
Functional characteristics have been associated with successful decannulation in children with trache- ostomies. Splaingard et al. [5] described and validated a simple three-parameter (locomotion, self-care, and communication) functional scale (Table 1), which was used to stratify functional status in children with acquired neurologic injury. A higher functional score correlated with a greater probability of successful decannulation. A lower functional status score, measured in areas of locomotion, self-care and communication, at six months after brain injury, predicted the need for tracheostomy for at least two years post-injury. In addition, functional status at 6 months after injury was a strong predictor of dependency and institutionalization at 2 years [5].
The purpose of the presented study was to determine whether a combination of particular medical conditions and degree of functional limitation predicted the ability of children with tracheostomy to tolerate decannulation once deemed appropriate by a normal capped tracheostomy polysomnogram.
Patient characteristics at last PSG with capped tracheostomy during study period (
104)
Patient characteristics at last PSG with capped tracheostomy during study period (
Study population
A retrospective study was performed of children at our institution who underwent evaluation with capped tracheostomy tube polysomnogram (cPSG) for possible tracheostomy decannulation between February 2005–September 2015. Institutional review board approval was obtained. Charts were reviewed for demographic information, functional status, sleep study characteristics, most recent airway evaluation and findings, and success or failure of attempted decannulation. Pediatric-trained Sleep Medicine Physicians Common comorbid conditions were reviewed in this cohort and included cerebral palsy, bronchopulmonary dysplasia (BPD), chronic lung disease, congenital or acquired neuromuscular diseases, congenital heart disease, and history of organ transplantation.
All cPSGs were performed at an AASM certified pediatric sleep center in a tertiary children’s hospital and were scored according to AASM scoring criteria for the time period from 2005 to 2015 [8–10]. Interpretation was performed by fellowship-trained, board-certified pediatric sleep medicine physicians. Recommendation for consideration for decannulation was consistent throughout the time of the study and included 1) an apnea hypopnea index (AHI)
Functional status assessment
The functional status assessment tool described previously by Splaingard et al. is shown in Table 1. This metric has three components: locomotion function (ability to ambulate with/without a gait aid and without support of another person to move about the home), self-care function (ability to perform simple tasks), and communication function (ability to communicate simple needs), was utilized to determine a total functional status score. (Table 1) [5]. Maximum possible total score on this assessment is 9 and minimum possible is 3.
Statistical analysis
The primary outcome in this study was the continued presence of a tracheostomy at 1 year after cPSG predicted readiness for tracheostomy decannulation. So that all children could be followed to determine this outcome, only cPSGs performed at least one year prior to analysis were included in the primary outcome calculations. Statistical analysis was performed to determine whether higher functional status scores at the time of cPSG were associated with a greater probability of recommendation for decannulation, and to determine if there was correlation between the number of comorbidities and functional status score. Mann Whitney U tests and Fisher exact tests were used respectively to evaluate differences in the primary outcome according to the continuous and categorical patient characteristics of interest. Trends in the proportion of patients with decannulation recommended with increasing function status scores were tested using exact Cochran-Armitage trend tests. The correlations between the number of comorbid conditions (which ranged from 0 to 7) and locomotion, self-care, communication and total function scores were evaluated using Spearman rank correlation coefficients. SAS version 9.3 was used for all statistical analyses (SAS Institute Inc., Cary, NC).
Comparison between patients with and without a tracheostomy at 1 year after recommended decannulation per PSG results
Comparison between patients with and without a tracheostomy at 1 year after recommended decannulation per PSG results
Of the 154 sleep studies performed with cPSG, during the study period, 139 sleep studies in 104 unique patients were performed more than one year prior to the time of analysis and were thus included in the analyses of the primary outcome. Characteristics of these 104 patients at the time of their last cPSG during the study period are shown in Table 2. At one year after their last cPSG during the study period, 83 of the 104 patients (79.8%) no longer had a tracheostomy. One patient was decannulated despite a cPSG that did not support this, as he was found to have tracheostoma collapse on bronchoscopy, that improved when the tracheostomy tube was removed. Among patients in whom decannulation was recommended after PSG, there was no significant association between any single comorbid condition and the ability to be decannulated at one year (Table 3). There was also no significant association between any of the individual functional status scores or total functional status score and successful decannulation in this group. Among the patients for whom decannulation was recommended, those with at least 3 comorbid conditions and a total functional status score of less than 7 were less likely to be successfully decannulated at one year than other patients (71% vs. 93%,
Proportion of patients with decannulation recommended by increasing locomotion, self-care, communication, and total function scores (
104)
Proportion of patients with decannulation recommended by increasing locomotion, self-care, communication, and total function scores (
Probability of successful decannulation given number of comorbid conditions and functional status score at time of capped PSG.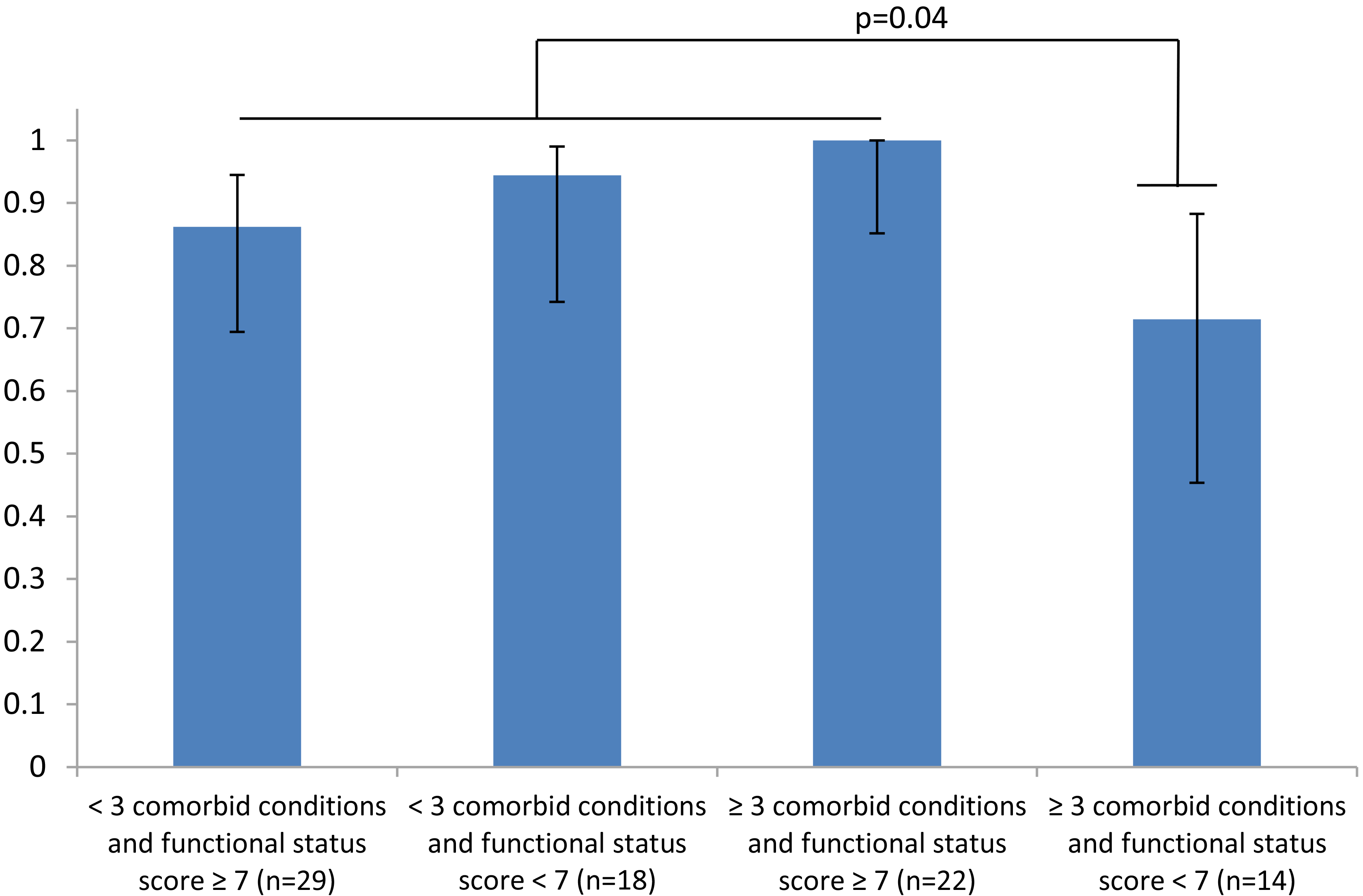
The need for a tracheostomy in some children may be definite, while in others, the ongoing necessity may present a more difficult technical, practical or ethical decision for physicians and caregivers. A tracheostomy tube may negatively impact quality of life for both patients and caregivers or family members. It has its own inherent associated morbidity and mortality. Common morbidities associated with tracheostomy include tracheostomy tube occlusion, accidental decannulation, tracheal scarring or stenosis and development of tracheo-arterial fistulae. These complications can be life-threatening or cause additional complications including anoxic brain injury or need for additional complex surgical correction. Because of these risks, all patients should be routinely reassessed for the ongoing need for tracheostomy. Once a patient is deemed appropriate for consideration of decannulation (no longer requiring ventilator support, able to tolerate capping of the tracheostomy tube), the appropriateness for possible decannulation should be assessed by capped sleep study, airway evaluation, or a combination of these modalities.
In previous studies, patients with neurologic impairments represent the majority of tracheostomy patients and have a higher likelihood of requiring a longer-term tracheostomy and a longer post-tracheostomy weaning and decannulation course. Carron et al. reported decannulation was accomplished in 41% of patients in their retrospective institutional dataset and that time to decannulation was significantly longer in those with neurological impairment [6]. Similarly, Funamura and colleagues reported a shorter time to decannulation in children undergoing tracheotomy for maxillofacial and laryngotracheal trauma compared to cardiopulmonary (21.2%) or neurological indications (38.9%) [1].
Hernandez and colleagues reported similar findings in adult patients with tracheostomy in intensive care units. Time to decannulation was correlated to Glasgow Coma Score (GCS)
This study informs the current literature by finding that functional status or comorbid conditions did not independently correlate with the ability to decannulate children who met decannulation criteria based on cPSG. Our results indicate that a child’s functional status or disease process alone should not determine viability for decannulation. A more nuanced regular evaluation may be necessary to successfully decannulate pediatric patients with multiple comorbid conditions and lower functional status. This is based on our finding that patients with 3 or more chronic comorbid conditions and lower functional status (
While this study aimed to address the paucity of literature on functional status as it relates to successful tracheostomy decannulation, it is clear that much more work remains to assess and validate our findings. While medical comorbidities are likely to contribute to increased time to decannulation, because of the retrospective nature of our study, we could not accurately assess how often each patient was actually assessed for decannulation due to lower functional status. Limitations of a retrospective design required all data to be compiled from electronic medical records. Functional status scores could not necessarily be obtained at the same exact time points as the cPSG, which may be confounding. While some medical comorbidities associated with increased time to decannulation were assessed, the list was not exhaustive and other potentially important factors such as insurance and provider and caregiver status were not analyzed. Finally we were not able to accurately determine how many patients could have been referred for consideration for decannulation but were not, due to low functional status.
Clearly successful long-term tracheostomy decannulation can be successfully accomplished in many children with multiple comorbidities and limited functional status. For this reason, there should be regular careful assessment and family counseling when considering decannulation in patients with more complex comorbid conditions and poor functional status.
Conclusions
Every child with a tracheostomy, even those with a diminished functional status should be re-evaluated regularly to determine appropriateness for decannulation. Utilizing a multi-disciplinary team for the management of these complex pediatric patients may be useful for surveillance of continued need for the tracheostomy tube. Future prospective studies where a
standardized tracheostomy decannulation protocol can be developed should be considered.
Footnotes
Conflict of interest
The authors have no conflicts of interest to disclose. The authors have no financial relationships relevant to this manuscript to disclose.