
Abstract
This case report details the complex rehabilitation of an adolescent patient with congenital heart disease with anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) who presented with a sudden cardiac arrest. The International Classification of Functioning, Disability and Health for Children and Youth, World Health Organization (ICF-CY WHO) principles were used to guide the course of the patient’s acute inpatient rehabilitation.
Introduction
In the United States, the incidence of sudden cardiac arrest (SCA) in children and young adults is approximately 2 per 100,000 person years [1]. Short term survival rates following SCA are near 40% with the widespread availability of community emergency medical services [2]. However, a recent population-based observational study reported an overall neurologically favorable outcome 1 month after an out-of-hospital cardiac arrest of only 3% [3]. In the Therapeutic Hypothermia after Out-of-Hospital Cardiac Arrest (THAPCA-OH) trial of targeted temperature management post-cardiac arrest, one third of subjects were alive after 1 year. Of these, one third had good to average functional status and one third had severely deficient function [4]. In the same trial, one fifth of subjects who had severe neurological deficits at discharge had significant improvement at one year follow-up [5].
Overall, there is a paucity of literature on the rehabilitation management of pediatric SCA survivors. In this case report rehabilitation interventions and the course of treatment for an adolescent who suffered a SCA due to previously undiagnosed congenital heart disease with an anomalous left coronary artery from the pulmonary artery (ALCAPA) were noted. Coronary artery origin from the pulmonary artery occurs in 0.4 percent of patients with congenital cardiac disease. It leads to anterolateral ischemia, and eventual dilated cardiomyopathy and heart failure [6]. Presentation of this abnormality may be delayed to later childhood, adolescence, or even adulthood if there is good collateral blood flow [6]. Following SCA, this patient had severe neurological, behavioral, and functional deficits that required intensive rehabilitation. Detailed rehabilitation aspects based on International Classification of Functioning, Disability and Health for Children and Youth, World Health Organization (ICF-CY WHO) principles after SCA of children with this rare pathology has not been documented previously in the literature.
Case history
The patient was a 14 year-old adolescent previously in good health with no chronic medical conditions, previous hospitalizations, or family history of SCA or congenital heart disease. The youth also had no history of fainting, chest pain, unusual fatigue, dyspnea, palpitations, or other cardiac symptoms. The patient collapsed and became unresponsive during a school basketball game and cardiopulmonary resuscitation was not started until eight minutes later, when the emergency medical technicians (EMTs) arrived. The EMTs administered automated external defibrillator shocks for pulseless arrest. Resuscitation efforts on the scene led to recovery of a stable pulse in approximately 16 minutes after which the patient was intubated and transported to the nearest emergency department. Diagnostic workup included computed tomography (CT) angiogram revealing ALCAPA. The pediatric intensive care unit course was notable for acute hypoxemic respiratory failure due to aspiration, post-arrest distal pulmonary emboli, and hypoxemic encephalopathy. The patient underwent surgical correction of the congenital cardiac defect, with left coronary artery re-implantation into the left aortic coronary cusp. Post-operative course was complicated by sinus tachycardia which improved with a course of beta blockers, and reactive pericarditis which improved with administration of non-steroidal anti-inflammatory drugs. The patient made hemodynamic improvements, but continued to exhibit neurological and cognitive sequelae due to hypoxic encephalopathy as well as dysphagia and vocal cord paralysis secondary to the initial emergent and traumatic intubation. Levetiracetam and prednisolone were started for encephalopathy. Following extubation and evidence of increased ability to tolerate bedside therapy interventions, the patient was referred to an acute intensive inpatient rehabilitation program.
Imaging
Brain magnetic resonance imaging (MRI) is often used after cardiac arrest to obtain additional data for patient prognostication and to plan for future care needs. MRI has superior accuracy to CT scans in assessing regional injury severity resulting from hypoxic ischemic injury [7]. The patient had consecutive brain MRIs which showed mild hypoxemic encephalopathy localized to the thalamic nuclei and general decrease of volume. A global reduction in brain volume is consistent with widespread deficits in memory, visuospatial, and executive function in adults and cerebral palsy and neonatal asphyxia [8]. However, information on the predictive value of MRI in older children is limited.
Discussion
Rehabilitation classification
Adherence to WHO principles are very helpful in formulating an overall comprehensive care model that can be achieved only in a multi and interdisciplinary setting [11]. The WHO principles are the basis of the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY), a derived version of the International Classification of Functioning, Disability and Health (ICF, WHO, 2001) designed to document characteristics of the developing child and the influence of the surrounding environment [10]. The ICF has two parts, each with 2 components:
Part 1. Functioning and Disability composed of: Body Functions and Structures Activities and Participation
Part 2. Contextual Factors composed of: Environmental Factors Personal Factors [11]
Figure 1 shows the ICF-CY model of functioning and disability for hypoxemic encephalopathy. The WHO outlines the following 5 principles of rehabilitation: Body Functions and Structures, Activities, Participation, Environmental Factors, and Personal Factors. The ICF-CY classifies health and health-related states and therefore requires the assignment of a series of codes that best describe a profile of the individual’s functioning.
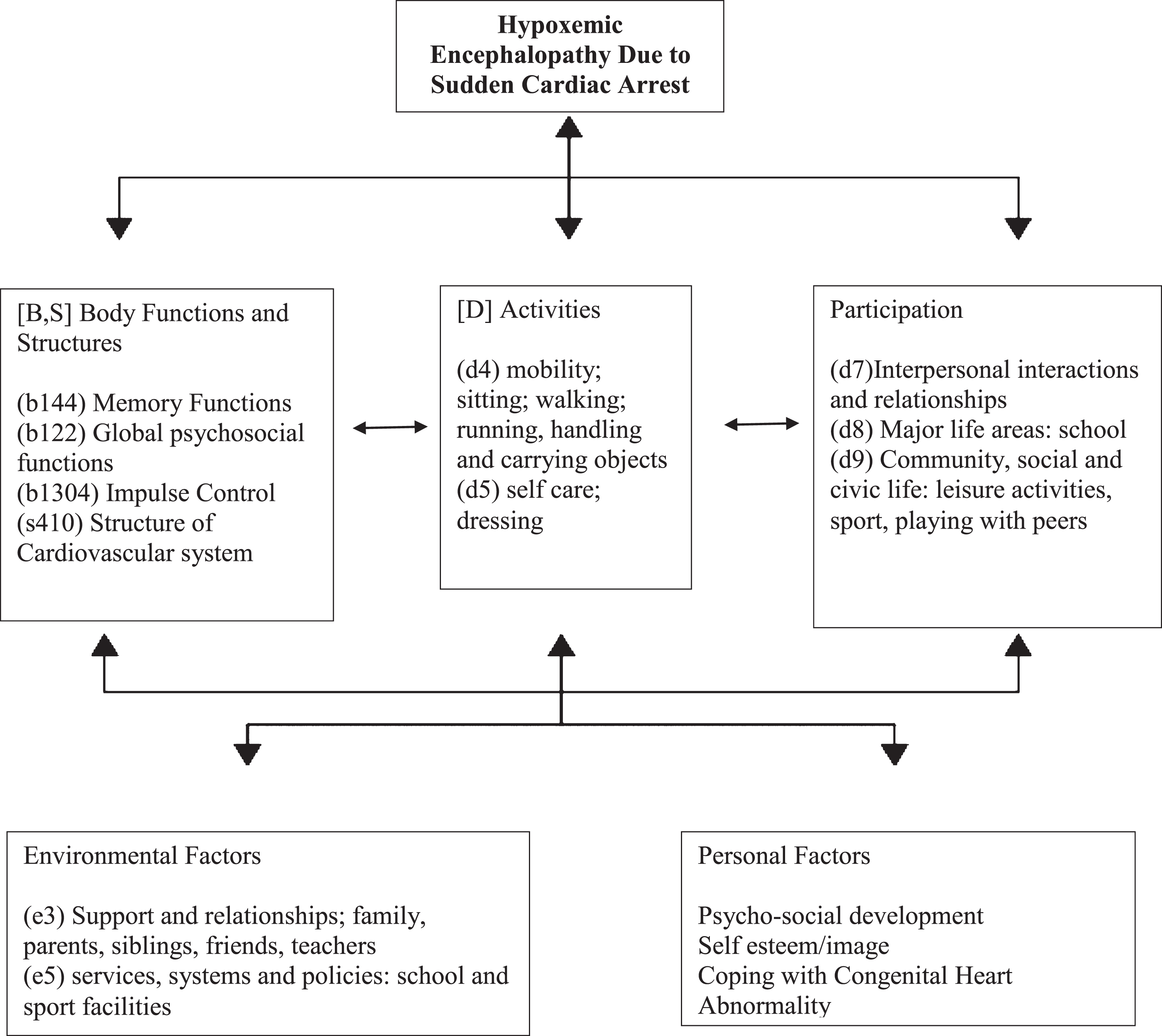
Model of Functioning and Disability for Hypoxemic Encephalopathy Based on the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY).
After recovery from cardiac surgery for correction of ALCAPA, the patient was transferred to acute inpatient rehabilitation, where the youth stayed for 8 weeks prior to discharge.
Functional mobility
At baseline, the patient had been fully independent with functional mobility and activities of daily living. On admission to rehabilitation, the patient required assistance to ambulate and also required an assistive device. The adolescent presented with deficits in dynamic and static balance and decreased lower extremity range of motion. While participating in physical therapy, the patient was monitored closely for tachycardia and required continued beta blockade. Therapy interventions included MotoMed, dynamic balance training, gait training, transfer training, and lower extremity strengthening. At the time of discharge, the patient was independent with bed mobility and ambulation to 150ft and could perform transfers with supervision.
Activities of daily living
The patient’s occupational therapy course centered on cognitive retraining. The patient presented with moderate cognitive impairments. There were new deficits in executive function, short term recall, and attention due to the hypoxic encephalopathy. Therapy included exercises in problem solving, sequencing, money management, and initiation of new tasks including organization, scheduling, and deduction. Therapies also focused on targeted use of internal and external recall strategies. By the time of discharge, the patient was more consistently oriented. However, the patient continued to have impairments in immediate and delayed recall along with carryover for new information. At the time of discharge, the patient was able to perform activities of daily living with setup and supervision. The patient required assistive devices including a wheelchair, shower chair, grab bar, and commode.
Speech and language
The patient had deficits in vocal expression and social interaction. The youth had reduced verbal output without focal language impairment, likely due to a behavioral component in addition to speech processing delays secondary to hypoxic encephalopathy. Disinhibition and impulsivity were also noted with occasional inappropriate verbal remarks. The adolescent struggled with pragmatic language skills including low initiation, limited spontaneous output, flat affect, decreased eye contact, and decreased verbal output while taking turns during conversation. Speech and language focused on verbal problem solving, verbal organization, and making inferences.
Dysphagia
The patient presented with mild oral dysphagia and severe pharyngeal dysphagia with frank silent aspiration of nectar thick fluids. Initially, the youth required a nasogastric tube but was able to progress to regular solids and thin liquids by the end of the rehabilitation course. The patient was evaluated by an ear, nose, and throat specialist and found to have moderate dysphonia due to vocal fold paresis. Vocal cord adduction exercises were targeted with improvement.
Behavioral Issues
The patient presented with flat affect, apathy, and loss of interest that differed from the youth’s premorbid behavior, and likely were sequelae of brain injury. The patient had no history of mental health disease other than a diagnosis of possible attention deficit hyperactivity disorder at the age of four that spontaneously resolved.
The adolescent also presented with agitation and nighttime delirium that was managed with risperidone at bedtime. This delirium resolved by discharge. The youth underwent formal neuropsychological evaluation and was found to have decreased awareness of new functional limitations, and deficits in social-emotional functioning. In a study of 52 survivors of PCA followed for a median of 5.6 years, many had attention and emotional/behavioral problems and required special education [16].
Follow-Up
After discharge from inpatient rehabilitation, follow-up was arranged with the local health care team, which consisted of a pediatric physical medicine and rehabilitation specialist, pediatrician, visiting nurse, physical therapist, occupational therapist, and social worker. The youth also required services at school due to ongoing disabilities.
Conclusion and summary
Pediatric rehabilitation is an essential component in improving functional, cognitive, and behavioral outcomes in children with severe neurological deficits secondary to SCA events. The WHO principles of rehabilitation should be implemented in all stages of medical care of these patients. After an intensive structured rehabilitation program tailored to the patient’s needs, this adolescent was able to make large functional gains that will increase the youth’s chances of a better transition into adulthood. This case was unusual in that the patient never presented with prior exertional cardiopulmonary symptoms while engaging in routine physical activity. Following rehabilitation, the patient required a physical activity evaluation of the frequency, intensity, and type of activity. The patient will need exercise testing to better define the risk of exercising based on the youth’s current level of fitness [4]. Rehabilitation specialists should be mindful of complications and be aware of comorbidities related to hypoxemic encephalopathy and iatrogenic factors precipitated by acute intervention. This patient also presented with new cognitive and behavioral deficits due to hypoxic injury that did not resolve by discharge from rehabilitation. These deficits will require ongoing monitoring and neuropsychological evaluation to assist in treatment and academic planning. A restorative goal-oriented and family-centered approach with the treatment of the whole person is the best approach for these complex patients. The use of ICF-CY WHO principles for rehabilitation allows a rehabilitation team to structure a complete rehabilitation program to benefit the patient.
Footnotes
Acknowledgments
We thank the patient’s pediatric rehabilitation team at Rusk Rehabilitation for their dedicated care of this adolescent.
Conflict of interest
The authors have no conflict of interest to report.