
Abstract
PURPOSE:
With children who are unable to stand or walk independently in the community, therapists commonly use standing devices to assist lower-extremity weight-bearing which is important for bone and muscle health. In addition, positioning in hip abduction may improve hip stability and range of motion. This is the first study to explore the effect of angle of inclination, hip abduction, body orientation, and tone on weight-bearing in pediatric standing devices.
METHODS:
This descriptive exploratory study used a convenience sample of 15 participants (2 with normal tone, 5 with generalized hypotonia, and 8 with hypertonia) (mean age of 5 years and 10 months, range of 3 years 4 months to 9 years 7 months); 13 of whom used standing devices at home, as well as 2 typically developing siblings (normal tone). Each child stood in 36 positions to measure the amount of weight-bearing through footplates.
RESULTS:
Weight-bearing was highest with 60 degrees of abduction and no inclination (upright) in supine positioning for children with low and normal tone. Children with high muscle tone bore most weight through their feet with no abduction (feet together) and no inclination (upright) in prone positioning. Overall, supine positioning resulted in more weight-bearing in all positions for children with low and normal tone. Prone positioning resulted in slightly more weight-bearing in all positions for children with high tone.
CONCLUSIONS:
Weight-bearing was affected by all three of the variables (inclination, abduction, and orientation) for participants with high, normal, and low tone. To determine optimal positioning, all standers should include a system to measure where and how much weight-bearing is occurring in the device.
Introduction and literature review
When children are unable to ambulate independently in the community, they are at risk for low bone mineral density (BMD), pathological fractures [1] and contractures [2]. Therapists often recommend standing programs for children who are limited ambulators or non-ambulatory and cannot stand unsupported for functional activities. Weight-bearing is one of the most often cited reasons for the use of standing devices in schools [3], yet only two prior studies have measured how much weight-bearing occurred [4, 5]. Load bearing through the legs with resultant muscle contractions is thought to be the mechanism for stimulating bone growth and thus increases BMD [6]. Standing five times a week may decrease spasticity, assist in maintaining hip and knee range of motion (ROM), and increase and/or maintain hip stability [7].
Pountney and colleagues described an association between improved hip stability and positioning in moderate hip abduction in standing, sitting, and lying positions [8, 9]. Three other studies [10–12] suggested standing with the legs abducted 60° (30° away from the midline for each leg) prevents and even improves hip subluxation as well as prevents hip ROM loss and adductor contractures in children with cerebral palsy. However, therapists and participants report 60° of total abduction can be uncomfortable [12]. The rationale for the influence of hip abduction on hip stability comes from the femoral head applying force to the growth plate of the acetabulum, with resultant bone response leading to more normal development. With abduction, the femoral head becomes more covered by the acetabulum and may lead to more normal development of the neck of the femur [13]. Although the research evidence is weak or very weak, systematic reviews suggest hip abduction may be considered as part of postural management programs [14, 15]. This has led to widespread use of hip abduction in standing programs without fully understanding its effects on weight-bearing.
Standing devices, commonly referred to as standers, are defined as durable medical equipment which support the feet, knees, hips, and trunk, so the user can remain upright in biomechanical alignment [16]. Standing devices are commonly used in schools, clinics, hospitals, homes, and other community settings to positively impact body structure and function [7]. Some models allow the user to transition from a sitting position to standing and some can accommodate up to 45° of flexion contracture at the hip, knee, and/or ankle. A few standing devices allow for hip abduction up to 30° on each side (60° total). Some standers are set in a fixed orientation (supine, upright, prone) while others allow for all three orientations (multi-positional). Recently, some dynamic models (ones that allow for active dorsiflexion, rocking anterior/posterior, and leaning in all directions) have been developed. There are also models that do not accommodate abduction but have wheels or power for independent mobility while standing, as well as wheelchairs that allow the person to be positioned in various stages of sit-to-stand, including upright.
Two prior studies that directly measured weight-bearing found that subjects bore 78% [4] and 68% [5] of their body weight in their feet while using standing devices. In these studies, positioning was neither described nor detailed. Also, the influence of inclination and orientation was not explored. Clinicians report many reasons for choosing prone versus supine positioning and/or varied inclination positions in standing devices [3]. There is little research to support this reasoning. To date, no studies have measured or compared weight-bearing during differing degrees of hip abduction or at different inclinations while standing. They also have not explored the influence of body orientation or tone on weight-bearing.
The purpose of this study was to explore the effects of three differing angles of inclination (upright [0°]/15°/30°), hip abduction (feet together [0°]/30°/ 60° total of bilateral hips), and body orientation (supine vs prone) in individuals with different types of muscle tone (high, low, normal) on amount of weight-bearing through the feet in two of three models of standers.
Methods
Institutional Review Board approval was obtained prior to data collection from Wheeling University.
This was an exploratory descriptive study. Participants were recruited from one therapist’s caseload as a convenience sample of all children who routinely used standing devices at home and received physical therapy at one outpatient physical therapy clinic. Participants were excluded if they had a history of uncontrollable seizures (>30 per day), autonomic dysreflexia, oxygen saturation measured by pulse oximetry below 90 percent, or skin concerns (redness or open lesions).
Typically developing siblings who attended clinic on the data collection day were also recruited as a comparison group. Children and their families were advised of the opportunity to participate during their therapy session immediately prior to the data collection day.
Descriptive data was collected on all participants at the start of the session including age, sex, diagnosis, weight, and muscle tone. Typically developing siblings were determined to have normal tone via physical exam. Hypertonia (or high tone) was defined as an “increased stretch reflex” [17] in both elbows and knees. Hypotonia was determined using the definition of “Hypotonia Syndrome” [18] in addition to the participant having at least 5 out of 8 of the following findings: decreased strength, hypermobile joints, increased flexibility, delayed motor skills, leaning on supports, rounded shoulders, decreased activity tolerance, or decreased attention/motivation. Participant’s total weight was measured immediately prior to data collection by placing the participant fully clothed (with shoes and orthotics) supine on a scale (WC Redmon Pet Scale from Amazon.com). This scale was calibrated with a five-pound weight before each child was weighed. Study risks and benefits were reviewed with each family and child. Parent consent and child assent to participate was obtained prior to start of data collection.
Each participant chose index cards from a tray which randomized their order of conditions including brand of standing device, inclination (0°/15°/30°), amount of abduction (0°/30°/60°), and orientation (prone/supine) (see Fig. 1 for study design and conditions). Total weight-bearing was measured by two digital postal scales mounted on the standing device footplate, one beneath each foot (Smart Weigh Digital Shipping and Postal Weight Scale from Amazon.com) on the standing devices. Weight measurements from both scales were added together and divided by participant’s total weight and represented as a percentage.
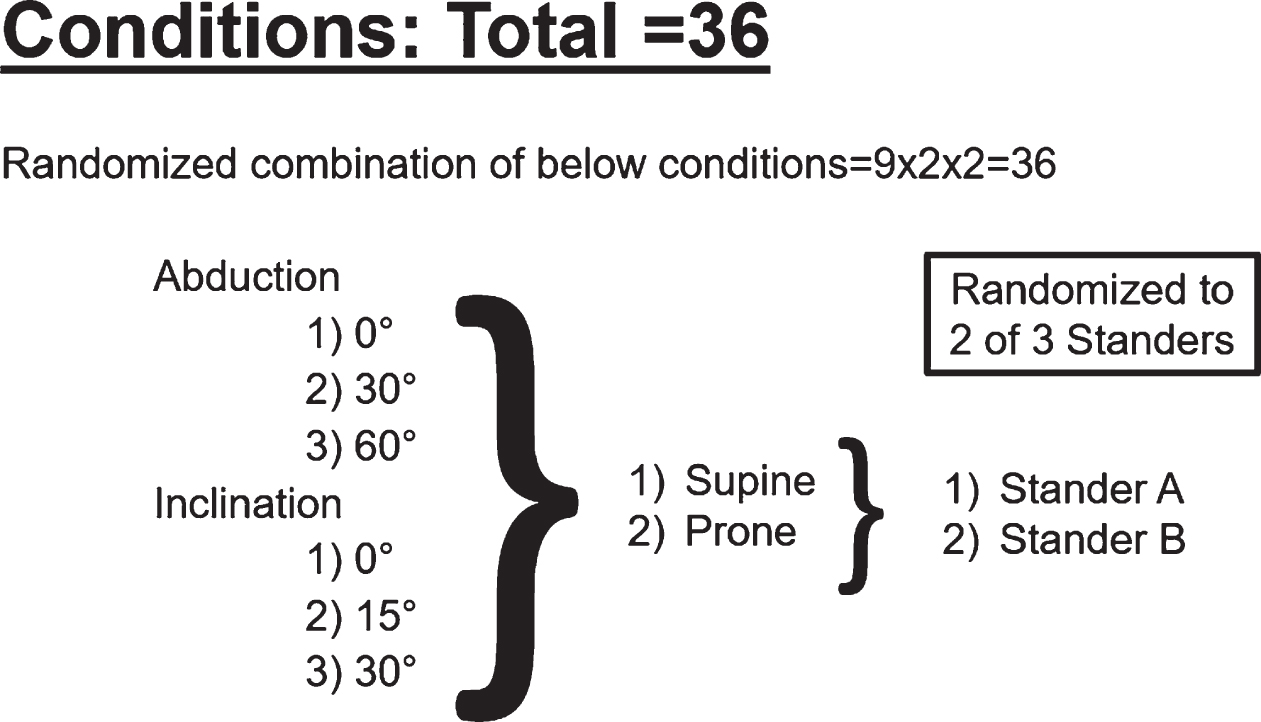
Conditions and Design of Study.
This study used three standing devices: 1) Jenx Standz, 2) EasyStand Zing, and 3) Prime Engineering HLT Superstand with Abduction System (see Fig. 2). They were all multi-positional standers allowing up to 30° hip abduction of each leg (60° total) and 30° of inclination. Each participant was positioned in two of the three standers. Devices were chosen out of convenience, as they were loaned free-of-charge by the manufacturers and their footplates accommodated the mounted scales. The investigators removed the heel cups and straps from all three models and mounted the digital scales on the footplates (See Figs. 3A and 3B).

Three Standers used in study; Zing, HLT Superstand, Stanz.
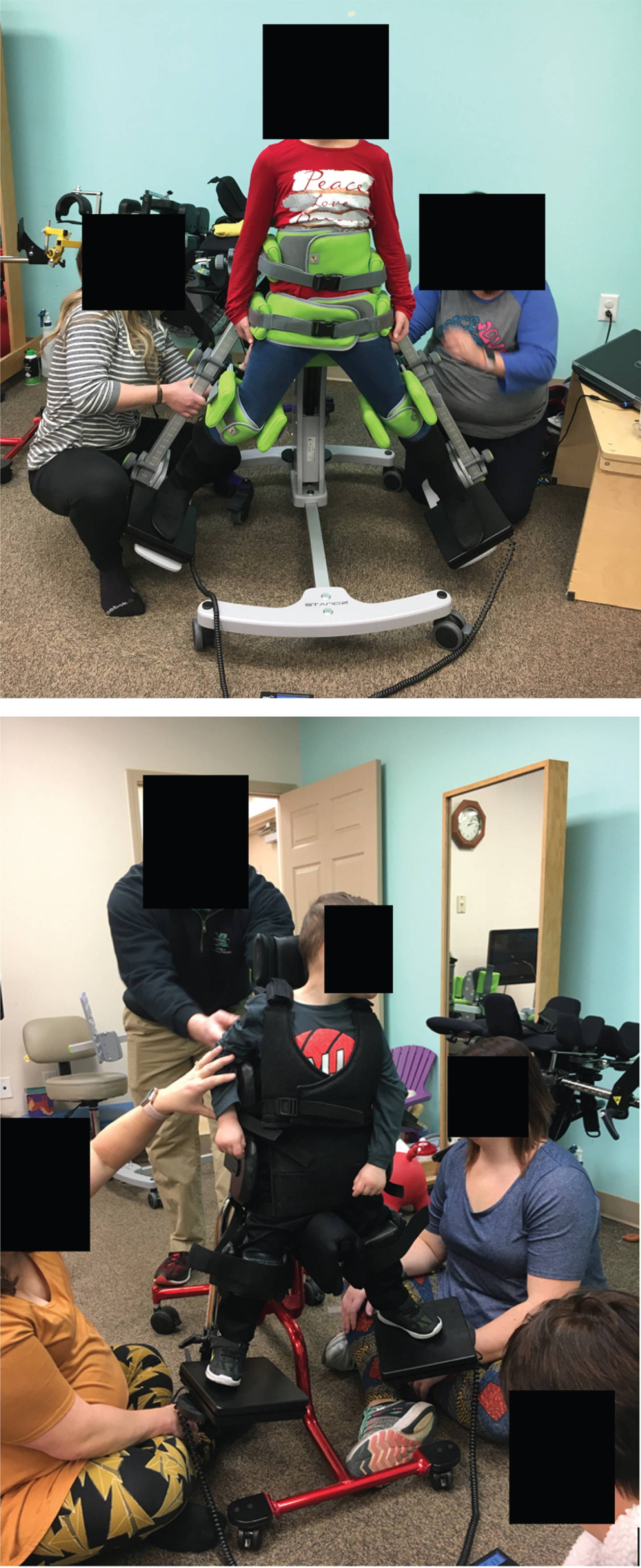
A Photo of Data Collection. B Stander Set-Up with Digital Scales Mounted on Footplates.
Five therapists were involved in data collection. One recorded all data while the other four positioned subjects and called out weight values. Inter-rater reliability was established during a practice session. Each scale was set to “zero” and calibrated with a 5-pound weight at the beginning of each measurement series. The child was placed in the stander by their regular therapist, who positioned feet, ankles, knees, hips, and pelvis in alignment. If the participant typically used orthotics during their standing program, these were used during data collection. The Face, Legs, Activity, Cry, and Consolability Scale (FLACC) scale was administered to ensure that children were comfortable and not experiencing pain (particularly for those children not able to express this verbally). The FLACC scale has been shown to be valid and reliable in measuring pain and non-pain distress in children [19].
After achieving body alignment in the standing device, the randomized conditions of inclination and abduction were applied. Leg internal/external rotation was not controlled. The sole of the shoe always maintained contact with the scale. The positioning therapist conducted the FLACC at each position to ensure the child was comfortable and willing to continue with the study. Inclination was measured at each position using an inclinometer (Tilt Meter App for iPhone). Angle of abduction was determined by measuring the inseam length and ensuring this equaled the distance between the feet. This configuration resulted in an equilateral triangle, in which each angle is 60°. When the distance between the feet was half the measurement of the inseam, the angle between the two femurs (abduction) was determined to be 30° total. This methodology was developed by Doug Nunn, PT at the Perlman Center at Cincinnati Children’s Hospital [20].
Each subject was randomized to be placed in prone or supine positioning and then moved passively in randomly assigned order of inclination (0°/15°/30°) and abduction (0°/15°/30°). This process was repeated for the second randomly selected stander for a total of 36 position combinations per stander (72 total per child). Each participant session lasted 45–60 minutes, with all 15 sessions taking place over a single day (see Fig. 4).
Weight-Bearing in All Positions.
The data were analyzed as a percentage calculated by dividing the total weight registered on the footplates (sum of two scale measurements) by the child’s total weight. Data were sorted by supine/prone position, amount of incline (0°/15°/30°), and amount of abduction (0°/30°/60°). Means, ranges, and standard deviations were calculated using Microsoft Excel 2020.
There is currently no published information about weight-bearing and clinically meaningful change. The literature does discuss non-weight-bearing and “toe-touch” weight-bearing in relation to adult orthopedics. In this body of literature, 10% weight-bearing and below is considered non-weightbearing [21], therefore we have used 10% change in weight-bearing as clinically meaningful change.
Results
Fifteen participants (13 who used standing devices regularly and two siblings) consented to and completed the study. Two presented with normal tone (typically developing siblings of participants used as a comparison group), 5 had hypotonia, and 8 had hypertonia. The average age of the sample was 5 years and 10 months (range 3 years 4 months to 9 years 7 months). Participants who regularly used standing devices had a variety of diagnoses including cerebral palsy with Gross Motor Functional Classification System Levels III-V, spinal cord injury, congenital cytomegalovirus infection, hypoxic ischemic encephalopathy, agenesis of the corpus callosum, and hydrocephalus (see Table 1). All 15 participants completed all 36 measurements. FLACC scores remained unchanged, and no children or parents requested to stop. There was no missing data.
Participant Characteristics
Participant Characteristics
Individual weight-bearing ranged from 35.0% to 133.0% (mean = 91.35%). Data points over 100% occurred in all groups, with the majority in participants with high tone in all positions and in all groups with feet together and no inclination (See Table 2). A weight measurement of over 100% cannot be fully explained. This may result when the child “pushes” on the body supports and down through their feet, as there would need to be some force production to get a reading over 100%. Readings over 100% were seen in two similar studies [11, 12] and were not unexpected. However, these data points may have skewed results to show more weight-bearing than occurred. Since these data points occurred in all groups, it should not have affected the overall findings.
Number of participants weight-bearing over 100% in each position
Key: H = High Tone, L = Low tone, N = Normal Tone.
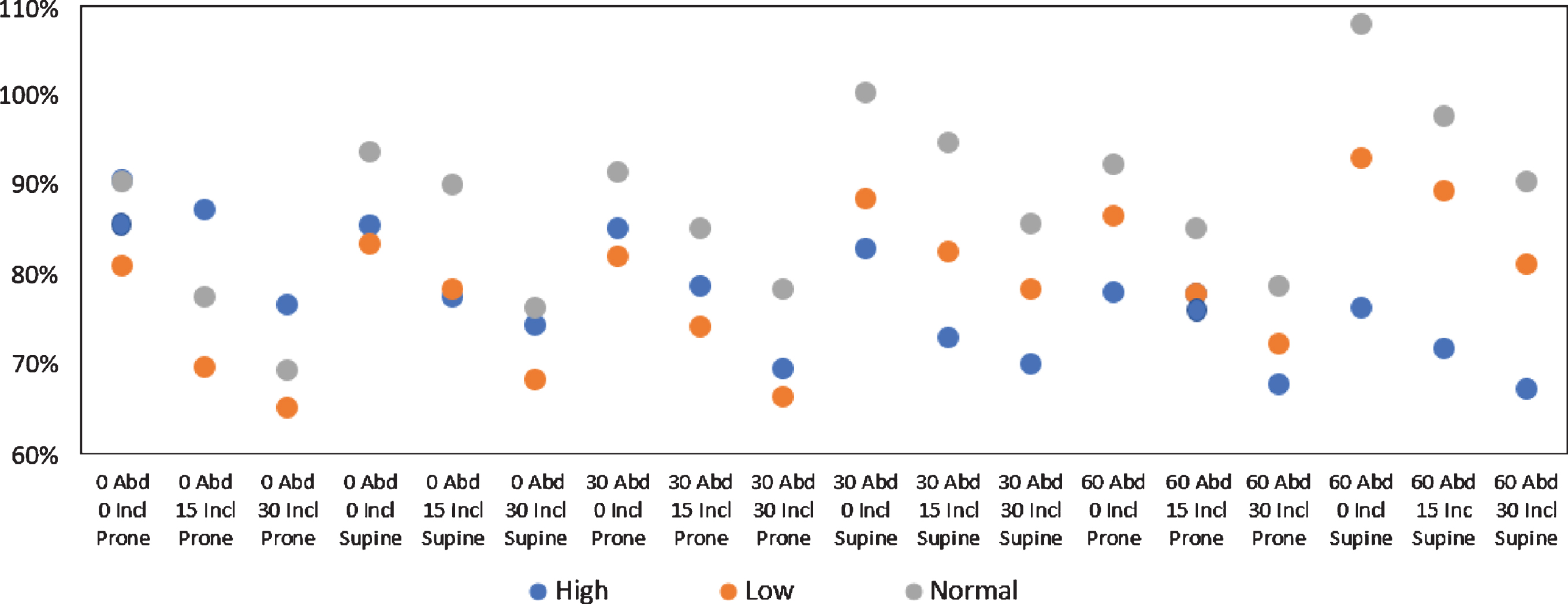
The high tone group demonstrated the most weight-bearing (91%) when upright with feet together in prone position, and the least weight-bearing (67%) with 30° of inclination and 60° of abduction in supine position (see Fig. 5). The low tone group showed the highest amount of weight-bearing (93%) when upright with 60° of abduction in supine position and the least (65%) with 30° of inclination, feet together in prone position (see Fig. 6). The children with typical tone demonstrated the most weight-bearing (108%) when upright with 60° of abduction in supine position and the least (69%) with 30° inclination, feet together in prone position (see Fig. 7). Supine positioning resulted in more weight bearing in all positions for the children with low and normal tone. Children with high tone bore slightly more weight in all positions when in prone position (see Figs. 8 9).
Weight-bearing for Participants with High Tone (%±standard deviation (range)).
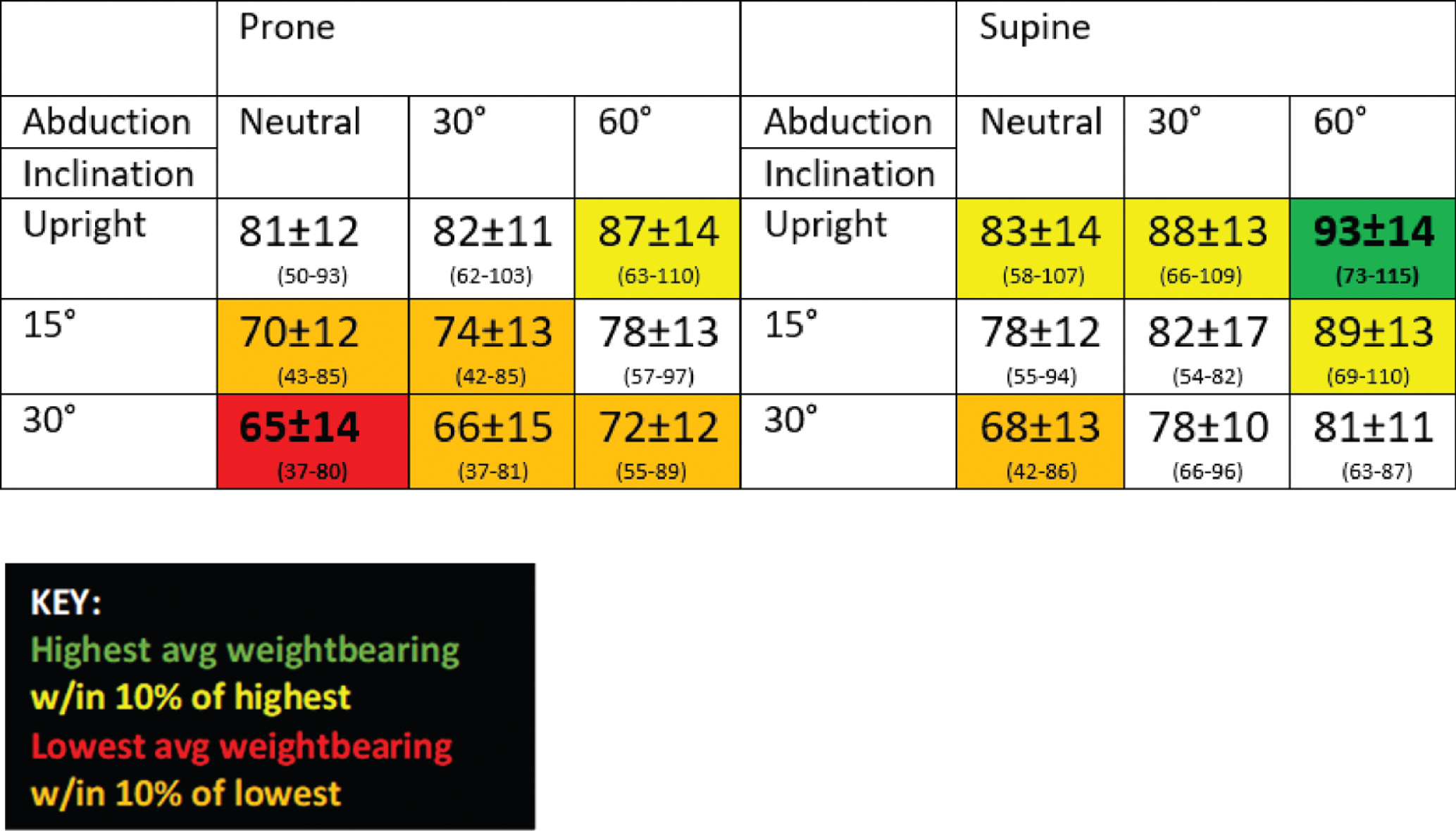
Weight-bearing for Participants with Low Tone (%±standard deviation (range)).
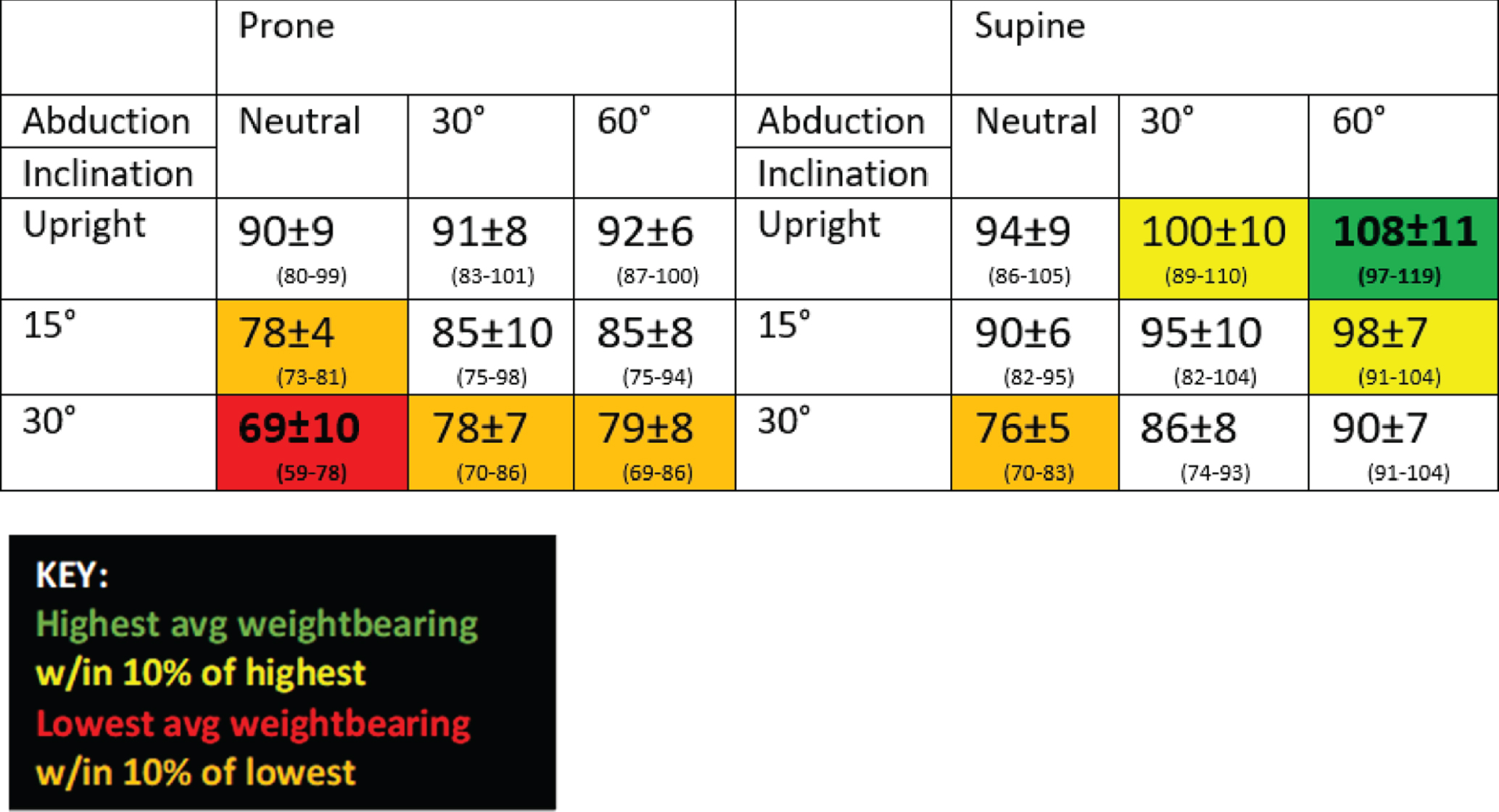
Weight-bearing for Participants with Normal Tone (%±standard deviation (range)).
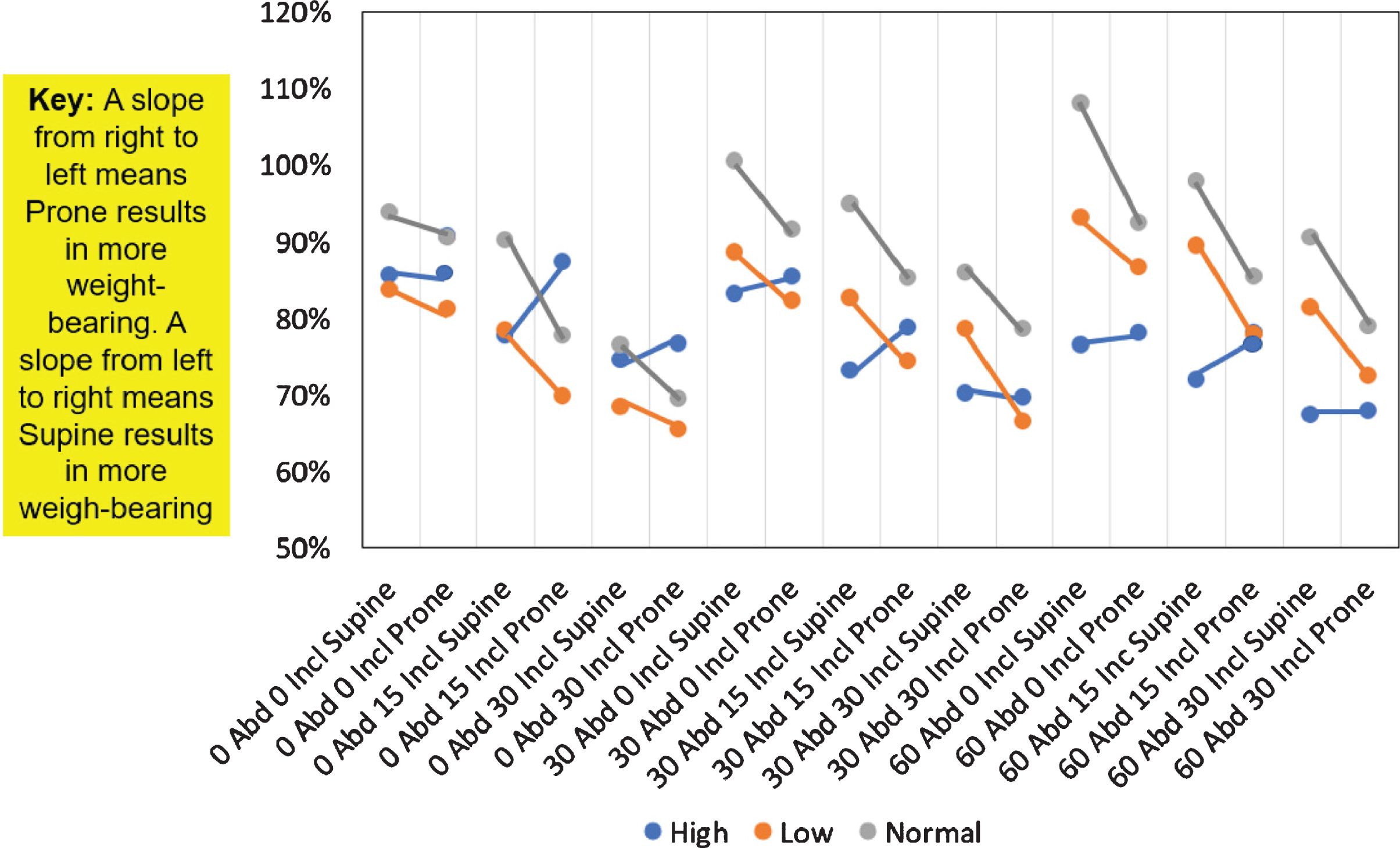
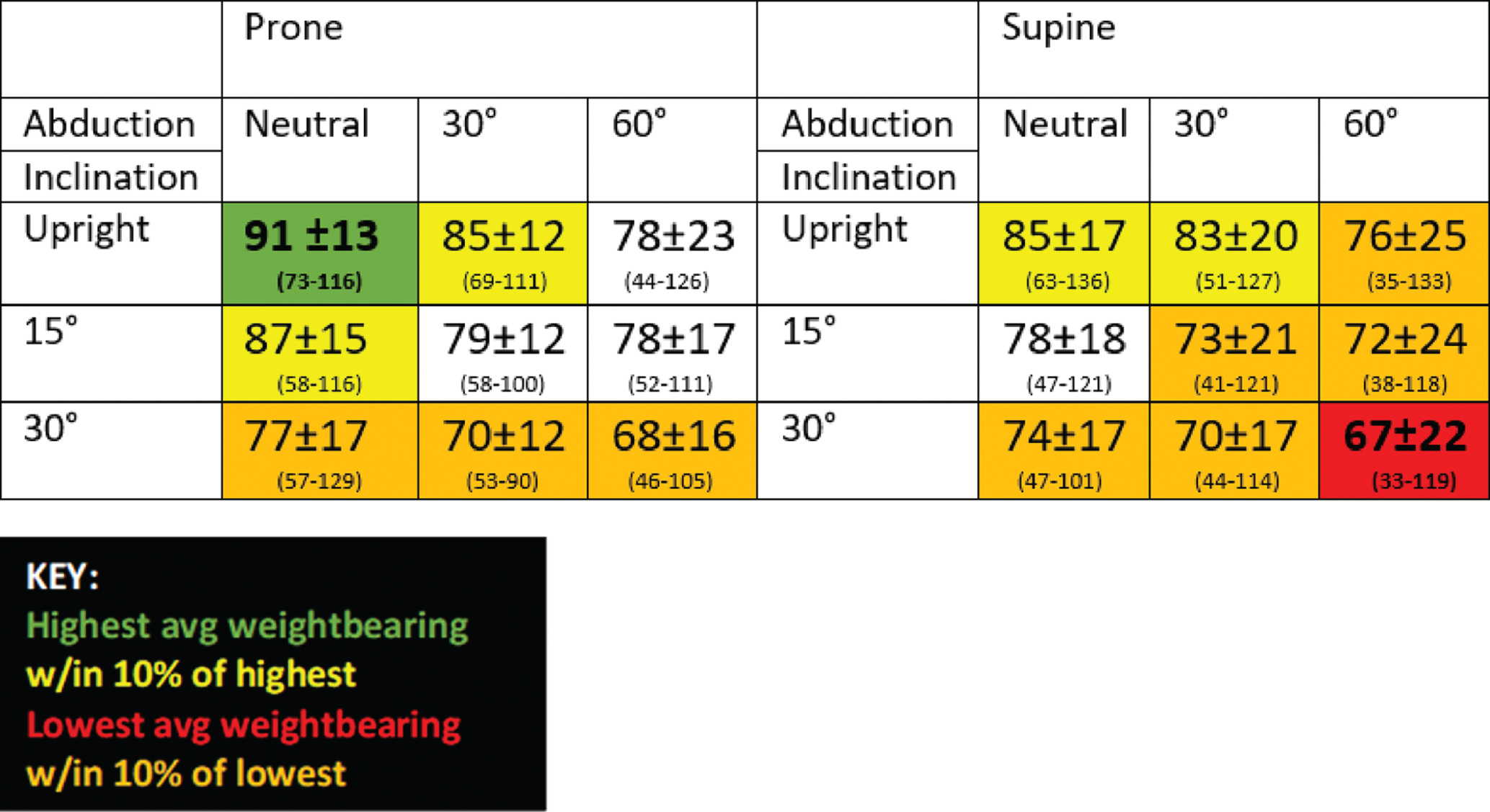
Weight-bearing in Supine vs. Prone Orientation.
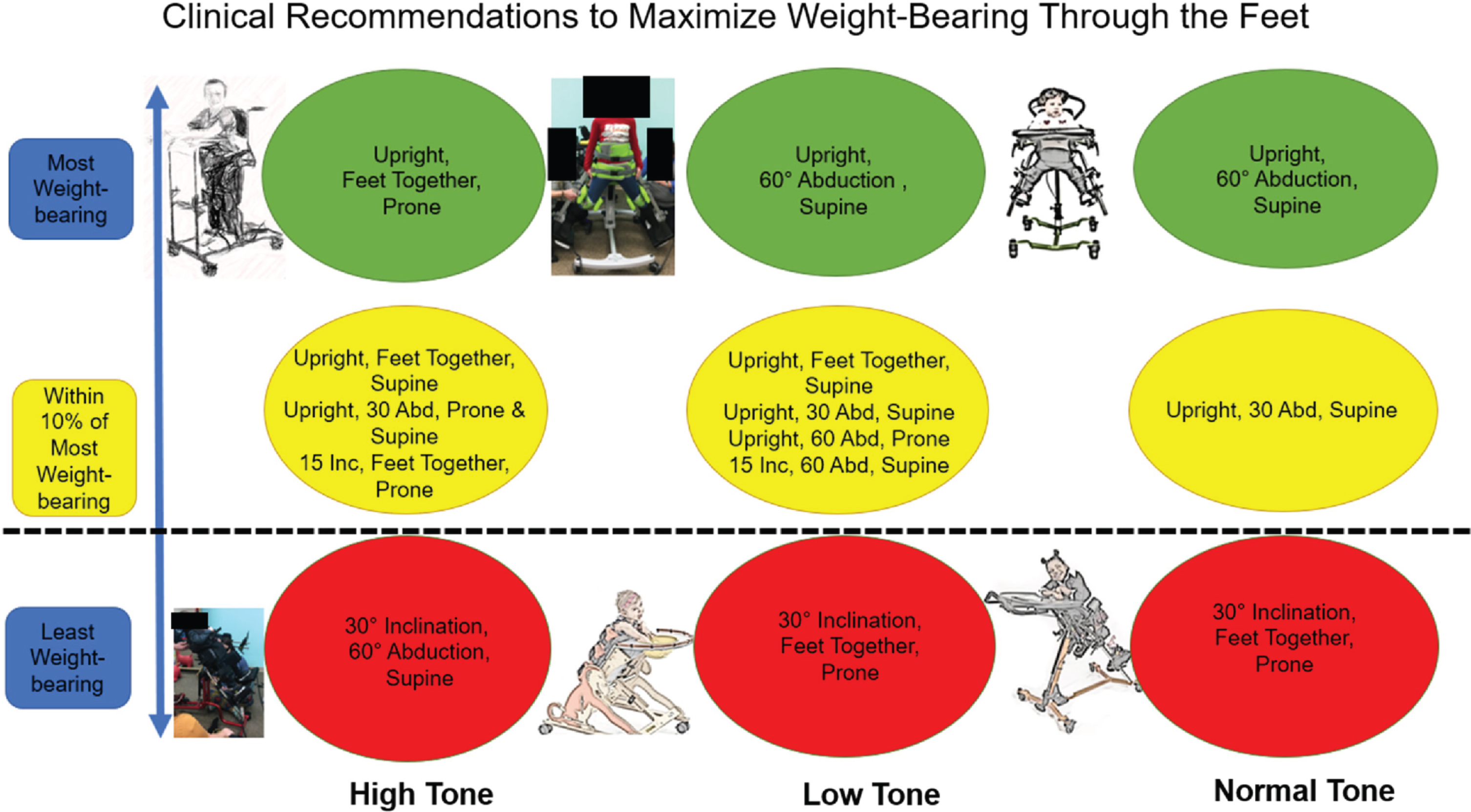
Clinical recommendations.
Tone affected weight-bearing through the feet in varied positions in this exploratory study. Children with normal and low tone behaved similarly in comparison to those with high tone. As predicted, any amount of inclination or abduction resulted in decreased weight bearing for children with high tone, with inclination resulting in a larger difference than abduction. Conversely, maximal abduction resulted in increased weight-bearing for the group with low and normal tone. These results suggest children with high tone respond differently to the various positions than children with low and normal tone. See Figs. 9 for Clinical recommendations.
These results demonstrate that one should avoid extremes in positioning (inclination and abduction) for children with high tone if weight-bearing is the main goal of the standing program. For children with high adductor tone, it is possible that increased abduction resulted in increased pressure or weight-bearing through the pommel or knee supports, although this was not measured. It is unknown if the reduction in weight-bearing through the feet that was measured is also accompanied by a similar reduction of forces through the acetabulum.
For children with low tone, it may be even more important to measure weight-bearing to ensure it is maximized. They have been described as “leaning into supports” [17] which may account for the differences. If the children with low tone “hung” or leaned on the lateral supports and surface of the stander, particularly in prone position, weight-bearing would decrease through the feet.
The data showed minor differences between the three standers. The standers differed in the amount of contact supports, with the Jenx Standz offering a solid posterior support similar to a tilt table. The Zing and HLT Superstand provided smaller support surfaces with open space between the supports. Sit-to-stand devices were not included because a previous study concluded that these devices demonstrated the lowest amount of weight bearing [5] and these models currently do not allow for abduction.
Limitations
This was a small exploratory descriptive study that measured weight-bearing through the footplates only. The convenience sample limits generalizability and the small heterogenous sample limits conclusions. It is possible that different results may have been found with larger samples. Forces through the head of the femur into the acetabulum may differ at the various angles and inclinations in comparison to weight-bearing through the feet, and weight may have transferred to other stander surfaces (such as the pommel or knee blocks). However, neither was measured in this pilot study and these factors may influence results.
Conclusion
In our small study population, angle of inclination, hip abduction, and orientation affected weight-bearing through the feet for children in standing devices. Clinicians should be mindful of these factors when developing a standing program for children and understand the cost-benefit relationship between postural alignment and weight-bearing in standing devices. If the goal is to increase weight-bearing in supported standing, it is recommended that children with hypertonia be placed in prone upright positioning with their hips in neutral (feet together) or slight abduction, and children with hypotonia should be placed in upright supine positioning with a moderate degree of hip abduction. Recommendations for future research include scheduling more time for each session, recording of stander use (e.g., journal of usage) to record whether weight-bearing changes over time, including a larger number of subjects, using only one brand of stander, and including whole body pressure mapping to document all weight-bearing surfaces.
Conflict of interest
Ginny Paleg received funding for travel to conduct this study from Prime Engineering. Dr. Paleg is also a paid educational consultant for Prime Engineering. She claims no bias in this study.
No other authors received funding or have any conflicts.
All products were provided free of charge from the manufacturers.