
Abstract
Postural management is a multi-disciplinary approach incorporating a comprehensive schedule of daily and night-time positions, equipment and physical activity to help maintain or improve body structures and function and increase activity and participation. Postural management may play a role in preventing contracture, deformity, pain, and asymmetry. This article provides an overview of the evidence supporting use of postural management to positively influence hip health in individuals with cerebral palsy, functioning as Gross Motor Classification System (GMFCS) levels IV or V. Sitting or lying without changing position for more than 8 hours, unsupported supine lying and asymmetrical or windswept postures are associated with pain and hip subluxation/dislocation. Although high-quality experimental research is still limited by many factors, there is limited evidence of harm, and most individuals at GMFCS IV or V require positioning supports to enable participation and function and ease caregiving. Clinical recommendations combining research and clinical opinion support the early use of comfortable positioning routines and/or equipment to reduce time spent in sustained asymmetrical or potentially harmful sitting and lying positions. Supported standing, active weightbearing and stepping are recommended to promote active movement and position change when possible, depending on individual, family and caregiver routines and preferences.
Introduction
Posture may be defined as the shape or alignment of body segments to each other, to the supporting surface and to the environment. Postural abilities allow individuals to stabilize and control body segments as appropriate to the task and environment [1]. Although individuals with cerebral palsy (CP) are not usually born with structural asymmetries, these often develop over time with limited postural abilities resulting in sustained asymmetric postures [2, 3, 2, 3]. These postures predispose development of secondary progressive deformities such as contractures of the hips and knees, scoliosis, pelvic obliquity, hip dislocation and windswept deformity [4–6].
In children and adults with CP, asymmetric postures have been shown to be more frequent at lower levels of function as classified with the Gross Motor Function Classification System (GMFCS), i.e., GMFCS levels IV and V [7, 8]. These individuals are also described as having non-ambulatory CP as they are dependent on wheelchairs for community mobility. Postural asymmetries are associated with hip and knee contractures and the inability to change position [7, 9]. Individuals who spend long periods of time in asymmetrical positions without being able to change their position are more likely to have contractures [7, 10], windswept hips and pain [8].
Hip joint structure is classified within the Body Structure component of the International Classification of Functioning, Disability and Health (ICF) while stability or mobility of the hip joint is classified as a Body Function. These are usually combined and defined as Body Structure and Function (BSF). However, the ability to maintain or change a body position such as lying, sitting or standing is classified at the Activity level [11]. Postural management programs are intended to maintain or improve body structures and function in order to increase activity and participation [1]. However, postural management equipment is used to assist with maintenance of position (Activity) and the equipment itself is defined as an environmental factor.
Postural management (also described as 24-hour postural management) is a multi-disciplinary approach that comprises a comprehensive schedule of positions, equipment use and activities. Appropriate support is provided in lying, sitting and standing as required to compensate for limited postural abilities [1]. Population-based data suggests that as many as 61–92% adults at GMFCS IV and V may require support to maintain an aligned and comfortable lying position. In the same study, all adults classified as GMFCS IV and V required adaptive seating within a wheelchair, while 61–70% used supported standing equipment [12].
In 2006, an expert consensus on postural management for children with CP recommended introducing support in lying from early infancy, sitting from 6 months, and standing from 12 months for children functioning at GMFCS IV or V [13]. However, in 2009, Gough [14] questioned whether strict 24-hour postural management programs achieved the stated goals and raised concerns about increased demands on the family and potential discomfort for the child. He concluded by suggesting a shift in focus from an emphasis on BSF to ensuring a greater focus on the environment, family needs and participation of the child.
Hip subluxation is commonly seen in GMFCS IV and V, and spasticity, muscle imbalance and lack of weight-bearing have been suggested as contributing factors [15]. Prolonged positioning interventions have been described as low-load passive stretch interventions [16] and recommended to prevent or delay the development of contractures and skeletal deformity including hip subluxation [17]. However, contracture in CP is not well understood, and there is debate in the literature, with various mechanisms proposed including immobilization, muscle fibre atrophy, spasticity, muscle imbalance and muscle or tendon structural changes [16, 18]. The relationship between hip instability and contracture or muscle length is unclear, and the influence of spasticity may be overemphasized since children with hypotonia and those without contractures also develop hip subluxation and dislocation [19, 20]. Rather than thinking of postural management in terms of stretching, recent population-based evidence would suggest promoting function and comfort in a variety of non-harmful positions throughout the 24-hour period [10, 12].
In 2012, Rosenbaum and Gorter reframed the ICF as the ‘F-words’ to promote Fitness (BSF), Function (activity), Friends (participation), Family (environmental factors), Fun (personal factors) and Future [21]. While the use of postural management to reduce the negative impact of sustained postures on hip health is typically focused at the BSF level [15, 22], the ‘F-words’ encourage a focus on optimizing functioning, activity and participation [23]. Intervening at the BSF level does not necessarily lead to improvements at the activity and participation level [24], so the goal should be primarily to increase comfort, reduce pain, and facilitate independent activity and participation with family and friends in meaningful and age-appropriate activities.
The purpose of this article is to synthesize evidence regarding use of postural management to positively influence hip health in children and adults with CP functioning at GMFCS IV or V. This is not a systematic review, but will combine evidence from published systematic reviews and experimental research studies (predominantly rated as low-level or low-quality) with other supporting evidence in order to develop evidence-informed recommendations for clinical practice. Inspired by the ICF and the ‘F-words’ framework, a shift to focusing on the potential of postural management programs and equipment to enhance the individual’s abilities to participate in life physically, mentally and socially is proposed.
Evidence supporting postural management programs will be described first, followed by evidence specific to lying or night-time positioning, adaptive seating and supported standing interventions. Active movement interventions and orthotics will be briefly discussed. Equipment to promote safe transfers and participation in activities of daily living should also be considered important components of postural management programs, although no research evidence is available. Since all experimental research evidence is considered low-level or low-quality, clinical recommendations at the end of the paper will be evidence-informed, combining research evidence with clinical opinion.
Evidence for postural management
The highest level of evidence currently available is an umbrella review of systematic reviews of interventions for children with CP [24]. Postural management to prevent hip displacement was found to be supported by an amber (‘probably do it’) level of evidence. This means that outcomes should be measured to ensure interventions are appropriate and effective for individual clients to achieve their desired goals. Although small effect sizes were found regarding use of any positioning, medical or even surgical intervention by itself to prevent hip displacement, the authors suggest that a comprehensive approach combining these interventions may be effective. This recommendation is based on longitudinal population-based studies from the Nordic countries (where there is a substantial decrease in hip displacement in comparison to other high-income countries), whose multi-disciplinary approach includes positioning, weight-bearing, botulinum toxin, surgeries and motor interventions [25]. The importance of surveillance to provide the right intervention at the right time and at the appropriate dose was stressed by Novak and colleagues [24], although clinical guidelines for positioning and postural management are not yet available.
Novak and colleagues’ amber rating of postural management intervention to prevent hip displacement was based on two systematic reviews. The reviews by Gmelig Meyling and colleagues [15] and Miller and colleagues [22] each included eight studies measuring outcomes of sitting, standing and lying positioning interventions and seven of these studies were included in both reviews. Although 7/8 studies reported positive outcomes, both author groups similarly concluded that the evidence supporting use of postural management to prevent or reduce hip migration in children with CP was limited by the lack of high-quality studies, and they were unable to make strong recommendations. Two newer systematic reviews evaluating impact of supported standing on hip stability have since been published in Spanish, but conclusions and rating of evidence is similar (despite all reviews having different inclusion criteria, methodologies for rating evidence level and study quality/conduct or risk of bias) [26, 27].
However, when considering the evidence supporting postural management, it is important to point out that conducting high-quality or higher evidence level studies is hampered by many problems. Firstly, it is impossible to blind participants to the use of postural management equipment. Although blinding assessors for a quantitative outcome such as hip migration percentage (MP) is possible, since the measurement is typically not taken in the equipment, other important issues related to hip health like comfort, tolerance, functional activity or pain are challenging or impossible to achieve blind assessment. Secondly, for individuals with CP who may be unable to achieve or maintain sitting, standing or symmetrical lying positions, the benefits may be clearly observable and withholding or delaying interventions that are either standard-of-care or have clearly observable benefits may be unethical [28].
Thirdly, CP is a heterogenous population and reliance on group means may mask benefits for complex individuals or prevent identification of benefits or harms in real world contexts. Preventing or limiting progression of deformities is an important outcome, but short-term randomized controlled studies are unlikely to show large effect sizes. Instead, long-term follow-up cohort studies, interrupted time-series, mixed methods or single subject research designs may be more appropriate strategies. Wang and colleagues have called for the development of new standards more appropriate for grading rigour of assistive technology and rehabilitation intervention research [28].
A retrospective cohort study suggests that children using postural support in all three positions (sitting, standing and lying) may maintain significantly better hip MP than those using support in only one or two of these positions [29]. Similarly, a prospective cohort study suggests that children using equipment at recommended and moderate levels had significantly less chance of both hips being subluxed than those using equipment at minimal levels at five years of age; additionally, the need for hip surgery or botulinum toxin interventions was reduced. The authors concluded that early provision of postural management equipment has a role to play in reducing hip problems [30]. However, there is debate as to whether the children who did not benefit were more severely affected and therefore unable to tolerate the total program [14].
Pountney and colleagues support the importance of maintaining symmetry without compromising function for those unable to change position and highlight the need for assessment of posture, and provision of postural support when needed, to prevent sustained asymmetric postures [30]. Since evidence supporting postural management is rated as amber due to low quality of research evidence, an appropriate measure of posture in the different devices is needed. The Posture and Postural Abilities Scale (PPAS) is a valid and reliable outcome measure for sitting, standing and lying postural interventions [31, 32]. It can be completed regularly to monitor changes over time, and score changes should result in program modifications with the goal of reducing or preventing further progression.
Lying or night-time positioning supports
Why is it important to consider positioning in lying?
Sustained asymmetrical postures are associated with hip deformities, and this asymmetry starts very early in life [3]. Preferred lying posture may also influence the direction of deformity for windsweeping and hip dislocation [6]. One in four adults with CP may only be able to use one lying position [9], and this finding may be as high as 50% for individuals functioning as GMFCS IV or V [7]. Both of these large population-based studies found that inability to change lying position was associated with postural asymmetries such as windsweeping. The more recent study of 830 adults found that odds of windsweeping were increased for individuals who could only be positioned in supine while lying and for those who spent more than eight hours in any lying position [9].
Evidence supporting provision of support in lying
A systematic review on the effectiveness of sleep positioning systems found low-quality evidence supporting improvements in hip stability [33], while no randomized controlled trials investigating this outcome were identified in the same author group’s Cochrane review [34]. An unpublished Delphi consensus by the same group supports use of sleep positioning systems to promote hip stability and postural alignment, increase comfort, reduce pain, and improve sleep quality in children functioning at GMFCS IV and V. They stress consideration of risk factors and provision of professional support to assist families implementing night-time supports. Since respiratory function may be compromised in individuals with severe CP, this should also be assessed when determining optimal positioning for children at night-time [35].
The highest evidence level intervention research supporting a positive impact from night-time postural management on hip stability is one small low-quality pilot study. A significant decrease in hip MP was demonstrated in one hip after being positioned in 20 degrees of hip abduction in a commercial sleeping system. However only seven of the 14 children were able to complete the one-year intervention. For those who could tolerate the lying system, significantly improved positioning for seating and toileting was reported by parents [36].
Clinical considerations for provision of support in lying
Ágústsson and colleagues recommend early introduction of postural control for individuals unable to change position due to increased risk factors for postural deformities [9]. However, it has been suggested that families are more likely to abandon sleep systems than other postural management equipment [37]. A negative impact on sleep or difficulties changing sleeping position may be causes for this abandonment [30, 36]. In a case-series of seven children with CP, quality of sleep improved in only two, while two of six who were thought to regularly experience pain from night-time positioning without support were more comfortable in their sleep system [37]. This reinforces that night-time postural support programs must be individually prescribed, developed with client and caregiver input and regularly reassessed.
While postural support and prevention of sustained asymmetrical lying positions may help reduce risk of windsweeping and hip dislocation, the importance of quality of sleep, comfort and reduction of pain cannot be overestimated. Casey and colleagues recently stressed the need to find non-harmful and comfortable sleeping positions rather than making recommendations to use rigid sleep positioning systems [10]. A full postural assessment is needed to identify the most appropriate lying positions for individuals. Once these positions are identified, different types of supports should be compared/trialled and caregiver education in varying lying positions provided. All recommendations should consider comfort to improve sleep as the primary outcome and strategies should be developed using a motivational interview with the parent or caregiver (who will be implementing the program).
Adaptive seating
Evidence supporting adaptive seating
Although a number of systematic reviews of adaptive seating have been completed, evidence tends to be inconclusive due to differences in participant characteristics, seating interventions and outcome measures [38]. For those classified as GMFCS IV or V, the benefits of seating may be self-evident, especially for those unable to maintain position without support. The most recent systematic review [39] found no evidence of harm and lower-level evidence to support use of adaptive seating to increase activity and participation for children with severe CP. Novak et al. [24] suggested there is weak positive evidence supporting the use of adaptive seating to improve postural support, hand function, pulmonary function, and pressure management, but impact on hip stability is not discussed.
In a before-and-after single group study, no significant improvement in hip MP was found in 27 children with CP who were provided with a moulded seating system. However, the authors felt that seating might slow progression of hip subluxation in developing children [40]. In a non-randomized group study, a statistically significant difference was observed in MP between treatment (moulded seat [siege moulé] 5 hours daily) and control groups [41]. Hip MP was stable (from 28.8 to 26.8) following two years of intervention while control group had worsening MP (from 23.0 to 37.7).
Picciolini and colleagues [41] suggest that conservative postural management of hip deformity through positioning the child in hip abduction in a moulded seating system is useful to prevent the natural progression of hip subluxation. However, Gmelig Meyling and colleagues’ review [15] suggests there may have been bias in selection procedures and that longer-term and larger studies would be needed to draw strong conclusions. A more recent non-randomized group study focused on standing interventions [42], which was not included in previous systematic reviews, reported maintenance of hip MP under 40% for children using adaptive seating with lateral trunk and pelvic supports and a pommel (abduction support) in combination with a daily standing program over 4–10 years.
Clinical considerations for adaptive seating
Although there is no strong research evidence, clinical practice consensus would support preventing hip adduction and windswept positions in sitting through use of moulded seating or pelvic and thigh laterals and an abduction support. There remains debate regarding the impact of hip abduction in sitting and angle needed, but 10–15 degrees is generally well tolerated and, for some children, increased hip abduction may help to decrease negative effects of spasticity and increase sitting tolerance. As with all postural management interventions, individualized assessment to identify a comfortable, non-harmful position that enhances activity and participation is essential, taking into account individual, family and caregiver preferences.
Supported standing
Evidence for supported standing
Weightbearing with the support of a standing frame has been suggested to improve bone mineral density (BMD) and range of motion (ROM) and to have a positive impact on hip stability in children with motor impairments [43]. In Novak and colleagues’ umbrella review [24], evidence regarding the impact of supported standing to reduce hip subluxation was not separated from the amber rating for all postural management interventions. Individual systematic reviews likewise conclude that strong recommendations cannot be made due to low-quality evidence [15, 27].
Evidence for standing in abduction
Increasingly, the clinical recommendation to stand children in abduction has been made, based on the theory that abduction positions the head of the femur to apply force to the growth plate and away from the acetabular rim, positively influencing hip stability. These recommendations are based on two studies [44, 45], although systematic reviews that evaluated impact of standing interventions on hip stability [15, 27] concluded that evidence was low-quality and inconclusive. The retrospective study of 26 children classified as GMFCS III, suggested that 13 children standing in abduction in a plaster mould over a 5-year period maintained stable hip MP in comparison to controls [44].
Martinsson and Himmelmann [45] compared an intervention group who stood in 15-30 degrees bilateral hip abduction in a Gazelle stander with a large control group from the Cerebral Palsy Follow-Up Program (CPUP) database. After 1 year, they concluded that children using straddled weight-bearing one hour daily had improved hip MP in comparison to those using standard-of-care standing, although children who stood in abduction following soft tissue lengthening surgery showed the greatest improvement in hip stability. The more recently published longer-term follow-up study [46] came to similar conclusions; however, dosage and position of standing is unclear for the large comparison groups.
While standing with feet together (hips adducted) is not recommended and may contribute to worsening hip MP in children with spasticity [47], standing in 10–15 degrees abduction appears to be more easily tolerated by most children who use standing frames. It also appears that, by itself, hip abduction does not ensure correct placement of the head of the femur in the acetabulum, as reported in a case study [48] in which the child required the addition of a trochanteric girdle to prevent subluxation during 20 degrees bilateral abducted standing.
Evidence for supported standing dosage
Another recent study including 36 children classified as GMFCS III-V [42] suggests that increased time in standing may have a positive influence on hip stability. There was a non-significant improvement in hip MP and acetabular index in those standing for 3 hours or more daily in comparison to children who stood less than 2 hours daily. However, even this time exceeds the most commonly reported dosage for supported standing of 1 hour, 5 times a week (McLean, Paleg and Livingstone, unpublished data) and less than 1 hour for adults with CP [12]. Htwe and colleagues’ study [42] does suggest that long-term (4–10 years) and consistent use of at least one hour of daily supported standing as part of a postural management program (that includes adaptive seating with laterals and pommel) can assist in maintaining hip stability. All children in this study were able to maintain hip MP under 40% without surgical intervention.
Clinical considerations for supported standing
Standing provides an important change of position for those who cannot change position independently and may reduce time spent in sustained lying and sitting positions [12]. Although supported standing may offer benefits in terms of improved alignment and maintenance of BMD, ROM and hip stability, it is essential that the standing program facilitates activity and participation and is successfully integrated into the child or adult’s daily routines. The opinions of the individual and family or caregivers, the rehabilitation team and other environmental factors must be taken into account when implementing a supported standing intervention.
Supported stepping
Supported stepping devices, also known as gait trainers, dynamic mobility devices and/or support walkers, have been shown to provide opportunity for children with CP GMFCS IV or V to increase physical activity, to take steps and to increase walking distance [49]. No studies have investigated impact on hip stability, although active weight shift is thought to be beneficial for BMD and hip joint development. All postural management programs should include opportunities for active movement to help reduce sedentary behaviors [50].
Orthotics
Knee flexion contractures appear to present earliest in children classified at GMFCS III-V [51], and hip and knee flexion contractures are associated with difficulties in sustaining a standing position or maintaining a symmetrical supine lying position [12]. Early intervention to prevent knee flexion contractures in children with CP should be considered [51] since windswept postures are associated with hip and knee flexion contractures [9, 12]. These contractures may be addressed using long leg bracing [52], supported standing [53] or commercially available standing device modifications [54]. Significant benefits from long-term use of hip abduction bracing following surgical soft tissue releases in young children have also been measured [55].
Although a small treatment effect was found, hip subluxation continued to progress, despite use of hip abduction bracing in combination with botulinum toxin injections in a randomized controlled study [56]. In a 10-year follow-up study, early use of hip abduction bracing combined with botulinum toxin was not shown to reduce the need for soft tissue and bony surgeries or improve hip morphology at skeletal maturity [57]. However, these interventions may delay surgeries, allowing growth and development. If hip abduction bracing allows independent sitting or movement in and out of position, it may enhance activity and participation for some individuals.
Summary
Sitting or lying without changing position for more than eight hours and asymmetrical or windswept postures are associated with pain, hip subluxation/dislocation and reduced abilities to lie, sit and stand [6, 58]. Although high-quality experimental research is still limited by many factors, evidence of harm is limited and most individuals at GMFCS IV or V require positioning supports to enhance participation and function and to ease caregiving. Experimental research, using appropriate longitudinal or single-subject designs, is required to provide more evidence for all postural management interventions. Postural assessment and evaluation of positioning and equipment use should be part of hip surveillance programs. Early detection of postural deficits and identification of the best positions, support and interventions are critical [10].
Clinical recommendations combining research and clinical opinion support early use of comfortable positioning or equipment to reduce time spent in sustained asymmetrical and potentially harmful lying or sitting positions. Supported standing and active weightbearing and stepping are recommended to promote active movement and position change when possible. The success of any postural management program depends on taking into account the needs and preferences of the individual, as well as ensuring that interventions enhance activity and participation and ease caregiving. Impacts of postural management programs are mainly positive but, since the experimental research evidence is limited, desired outcomes should be measured to ensure that interventions are effective for individual children and adults. An individualized and comprehensive program should be considered early in life for children functioning at GMFCS IV or V and continued across the lifespan as warranted.
Clinical recommendations
Promote comfortable and non-harmful positioning in lying and sitting. When possible, ensure the individual can sleep in more than one position. For children with increased tone, provide medial thigh support in lying and a pommel or moulded seating to prevent windsweeping and hip adduction. For children with hypotonia, full length pelvic and thigh lateral support is needed to limit frog leg (excessive bilateral hip abduction, flexion and external rotation) positions. Encourage supported standing in 10–15 degrees hip abduction bilaterally (20–30 degrees total) at least one hour daily as an important change of position from sitting or lying. Ensure that all positions and recommended equipment or supports promote functioning and participation in age-appropriate and meaningful activities. Encourage active weightbearing and movement, with a supported stepping device, to reduce sedentary behavior. Other active movement options include cycling, run biking and swimming. Decrease use of unsupported supine lying, particularly during daytime, and encourage more time in varied upright positions. Avoid more than 8 hours in one position. Postural management should be considered during all daily routines including transfers, toileting, bathing, dressing, eating and drinking to enhance function and participation and reduce negative consequences from harmful positions. See Fig. 1 for recommended age of introduction. Use a valid and reliable postural assessment such as the PPAS to identify asymmetries and intervene early [59].
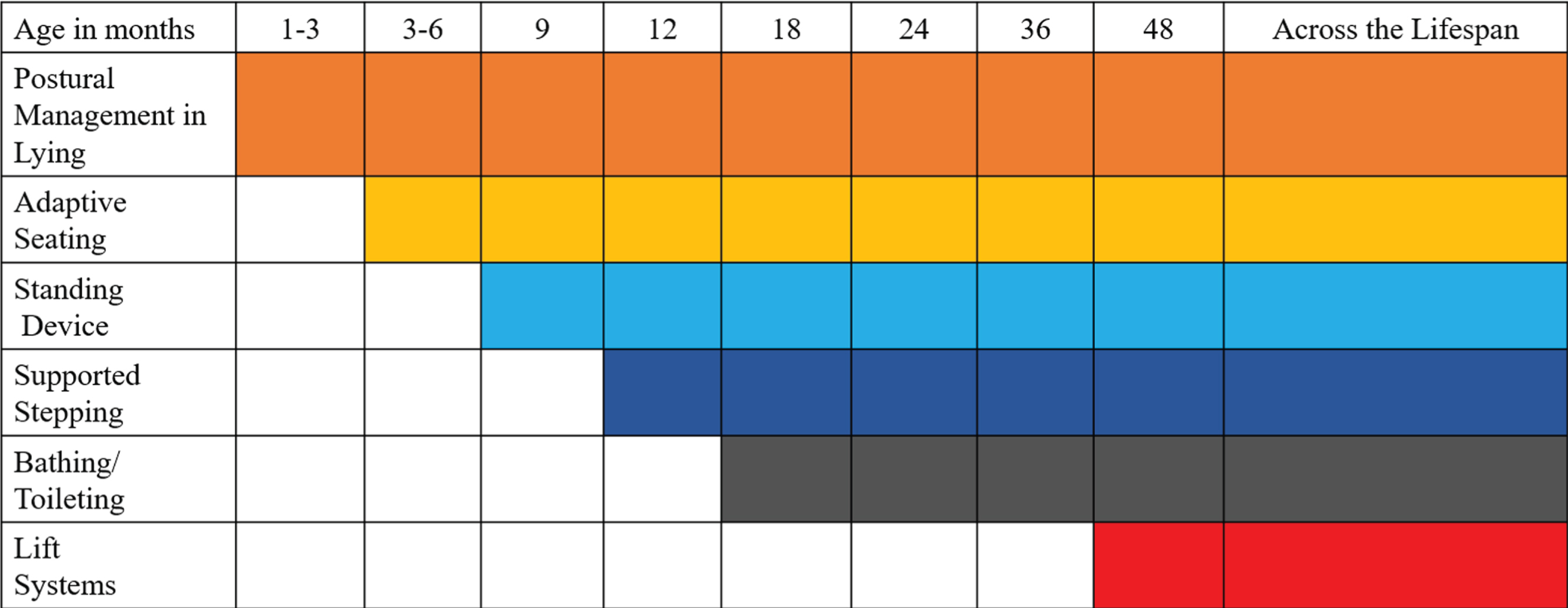
Recommended schedule of interventions.
Footnotes
Acknowledgments
This study was unfunded and did not receive any specific grant from any funding agency in the public, private or not-for-profit sector. RL declares no conflict of interest in relation to the research, conduct or authorship of this article. GP has worked as a paid educational consultant for various manufacturers of standers and gait trainers. Funding from these sources did not influence or bias the content of this work.