
Abstract
PURPOSE:
This study aimed to explore stander use in individuals with Duchenne Muscular Dystrophy (DMD).
METHODS:
This mixed method research study employed a survey with categorical and open-ended questions related to stander use. Categorical responses were analyzed quantitatively. Qualitative analysis of open-ended responses was linked to the International Classification of Function. Qualitative and quantitative results were merged to derive meta-inferences.
RESULTS:
Of 147 respondents, 28.6% (n = 42) reported stander use. Equipment used included sit-to-stand stander (n = 27), power standing feature in a wheelchair (n = 13), and unspecified equipment (n = 2). Economic services were the most common barrier to stander obtainment. Age of loss of ambulation (LOA) and age of start of stander use were positively correlated (r = 0.61, p < 0.0001, n = 36), with 59.5% initiating stander use after LOA. Twenty-nine respondents reported standing less than the recommended dose of 60–90 minutes at least five days a week, with frequency directionally less than five days per week (p = 0.06) and time significantly less than 60–90 minutes (p = 0.002). Respondents’ total dose was significantly lower than the recommended 300 minutes (p = 0.02). Lack of time and presence of contractures contributed to decreased duration of use.
CONCLUSION:
This study provides a greater understanding of stander use among individuals with DMD and can assist with decision making about stander use prior to complications of disease progression to promote optimal health despite reported barriers.
Introduction and purpose
Duchenne Muscular Dystrophy (DMD) is an x-linked disease stemming from mutations on the dystrophin gene resulting in impaired dystrophin protein production [1]. Occurring in an estimated 1 in 3500 to 5000 live male births [2], children with DMD present with progressive muscle weakness and degeneration culminating in loss of independent ambulation and eventual death in the second or third decade of life due to cardiac or pulmonary complications [3]. As weakness progresses so do associated comorbidities. Glucocorticoids have demonstrated efficacy in delaying these symptoms and are a staple of DMD treatment [4], but they may negatively impact bone mineral density [5] and only serve to delay the symptoms. Once a child loses the ability to ambulate, health can deteriorate due to lack of mobility, and the child may experience painful and costly complications (e.g., development or worsening of joint contractures, scoliosis, and respiratory decline) [3, 7]. In particular, scoliosis stemming from progressive muscle weakness has been associated with worsening pulmonary functioning and is particularly troublesome [6, 7].
In addition to the pathophysiologic effects of this progressive disease, DMD also impacts components of health more broadly. In a study of 50 boys with DMD and 25 unaffected age-matched boys, participation in physical activities was significantly lower in boys with DMD than unaffected boys [8]. Perceived quality of life was markedly diminished in children with DMD relative to unaffected controls. The amount of time boys engaged in an activity, as well as participation in social activities, declined for older boys with DMD while remaining stable for older unaffected boys. This study found that the decline in social participation occurred after the age of 10 years, around the time when individuals with DMD experience a decrease in motor abilities such as ambulation.
A supported standing program is an intervention for individuals with DMD to reduce or prevent the complications from loss of ambulation (LOA) discussed above [3]. It involves the use of a stander device to support the individual’s body in an upright position. Many benefits of supported standing are reported for individuals with DMD. In a study looking at 136 individuals with DMD, the rate of scoliosis progression was significantly reduced and forced vital capacity and peak expiratory flow rate significantly improved in those who accepted a standing regimen [9]. In a small sample of boys with DMD, hip and knee flexor muscle lengths also improved [10]. Lastly, participation in a supported standing program utilizing a standing device built into a power wheelchair was associated with short-term maintenance of musculoskeletal status and advantages to mental health in adolescents with DMD [11].
Due to the limited number of studies with low levels of evidence evaluating the use of supported standing programs in DMD, additional evidence regarding stander use in this population may be extrapolated from broader literature. A meta-analysis of 39 studies evaluating the use of supported standing programs for adults and children with neuromuscular conditions found that supported standing may reduce hypertonicity, improve range of motion and bowel function, and increase bone mineral density [12]. A subsequent meta-analysis of 30 studies evaluating the use of supported standing programs in a pediatric population with or without neuromuscular disorders demonstrated improvements in bone mineral density, lower extremity range of motion, hip biomechanics, and spasticity [13].
Based on the results of this meta-analysis across a multitude of diagnoses, standing has been recommended for a duration of 60 to 90 minutes at a frequency of five days per week to positively affect bone mineral density and increase range of motion [13]. A consensus statement for the prescription of power wheelchair standing devices in young people with DMD also supports use of the standing feature for at least 60 minutes for 4 to 5 days per week [14]. Additionally, a consensus statement for management of individuals with DMD recommends initiating use of supported standing devices when standing in good alignment becomes difficult, if contractures are not too severe to prevent positioning or tolerance [3].
Despite the potential health benefits associated with supported standing regimens, the use of standers in the DMD population is limited. One study reported that only 3.1% to 22.2% of individuals with dystrophinopathies, including DMD, had ever used a stander, but stander use varied significantly by region across five sites in the United States [15]. There appears to be a discrepancy between recommendations for standing programs and implementation. Therefore, further investigation of patient and family perspectives of stander use among individuals with DMD may elucidate barriers and provide opportunities to increase participation in supported standing programs. The purpose of this study was to obtain a comprehensive understanding of the use of supported standing programs in individuals with DMD to identify modifiable barriers to use.
Methods
Design
The current study utilized a mixed methods research (MMR) design to achieve the study aim. MMR utilizes both quantitative and qualitative data analysis and integrates the data to draw interpretations based on the combined strengths of both data sets to better understand the research problem [16, 17]. This study utilized a concurrent triangulation design, a validating quantitative data model of MMR. This model involves collecting quantitative and qualitative data simultaneously from a survey and using the qualitative information to validate the quantitative results [16, 18].
Upon approval from the Institutional Review Board, data collection occurred via administration of a cross-sectional survey (see Appendix 1) that included both categorical and open-ended questions and was administered online via Research Electronic Data Capture (REDCap) tools hosted at Cincinnati Children’s Hospital Medical Center [19, 20]. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources. Respondents’ consent was implied through completion of the survey. All responses were anonymous. Two versions of the survey were administered: one version for parents/caregivers of individuals diagnosed with DMD that will be referred to as the caregiver survey questionnaire (CSQ), and another version for adult individuals diagnosed with DMD that will be referred to as the DMD survey questionnaire (DMDSQ). Survey types differed in two ways. First, the CSQ included an item asking about the number of children in the household diagnosed with DMD. Respondents could take the survey multiple times to capture data relevant to each of their children diagnosed with DMD. Second, questions were framed differently between the two survey types to tailor them to the identity of the respondent (i.e., parent/caregiver vs. individual with DMD). Both survey types collected identical data.
Inclusion criteria for completing the survey was based on responses to screening questions 1–3 (refer to Appendix 1). Question 1 confirmed that the respondent was either a parent or caregiver of or an individual with DMD. The second question confirmed that the individual with DMD was male. The third question confirmed that the respondent was at least 18 years old and that the individual with DMD was at least 10 years old. The study excluded respondents who lacked the English literacy necessary to complete the survey.
All respondents who met the inclusion criteria were asked if they were familiar with the use of standers for individuals with DMD (Appendix 1: CSQ 1; DMDSQ 1) and answered demographic survey questions (Appendix 1: Demographic Questions). Those who were familiar with the use of standers, but who were not currently using a stander (Appendix 1: CSQ 3; DMDSQ 1), answered two additional questions: (1) reasons that may keep their child/themselves from using a stander and (2) any other thoughts they would like to share. Those respondents who were familiar with the use of standers and currently using a stander answered all survey questions.
Recruitment of participants
Recruitment occurred simultaneously through two sources. The first recruitment source was Parent Project Muscular Dystrophy (PPMD), a national public organization for DMD. The survey was sent to 1,660 unique email addresses of male PPMD registrants with DMD living in the United States. The second recruitment source was patients seen in the Comprehensive Neuromuscular Center at Cincinnati Children’s Hospital Medical Center, which serves patients both nationally and internationally. Four hundred and eighty-eight emails were sent to families of males with DMD via this recruitment source. Respondents were asked to follow an emailed link to the online survey. Follow-up emails were distributed at two and four weeks. Investigators allowed two months from the initial email distribution date to complete the survey.
Quantitative analysis
Quantitative analysis explored responses to categorical survey questions pertaining to stander acquisition, initiation of stander use, stander dose, and location of use (Appendix 1: CSQ 3–14; DMD 2–13). Where applicable (Appendix 1: CSQ 6, 8, 9, 13, 14; DMD 5, 7, 8, 12, 13), survey responses were categorized according to dose of stander use, utilizing the frequency, intensity, timing, and type (FITT) principle [21, 22]. Frequency was defined as the number of days per week of stander use. Intensity was determined by the amount of upright position achieved in the stander using pictures in the survey (Appendix 1: CSQ 13; DMDSQ 12). Timing was defined as the duration of stander use in number of minutes per day. Lastly, type was described by the type of stander, i.e., a power standing feature in a wheelchair (PSW) or sit-to-stand stander (STS).
Descriptive statistics were computed using Microsoft Excel (Microsoft Office 365 ProPlus 2013, Version 15.0.4893.1002) for analysis of ambulatory status, initiation of stander use, stander dose, stander acquisition, and location of stander use. Frequencies and percentages were derived for categorical variables. Comparative statistical analyses were conducted using SAS® version 9.4 (SAS Institute, Inc., Cary, NC) to compare LOA and start of stander use, reported dose versus recommended dose, and dose by stander type. Pearson’s correlation analysis was performed to compare LOA to start of stander use. Student’s t-tests were performed to determine if respondents’ stander use matched recommended dosing (a duration of 60–90 minutes at a frequency of at least five days per week), as well as the total dose equal to the product of the minutes per day and the days per week. Two-sample Student’s t-tests were used to measure differences in use between the two stander types (p < 0.05). Satterthwaite approximation was used for the two-sample t-tests. The relationship between dose and stander type was evaluated using Fisher’s Exact Test.
Two neuromuscular physical therapists reviewed open-ended survey responses related to liked or disliked features of the stander and what would make using a stander easier (Appendix 1: CSQ 16–18; DMDSQ 15–17) and utilized thematic analysis to analyze the data. Categories were analyzed using descriptive statistics in Microsoft Excel. Frequencies and percentages were derived for categorical variables.
Qualitative analysis
Open-ended survey responses related to problems encountered when trying to get a stander, reasons the individual with DMD does not use a stander, and perceptions around importance/usefulness of standers (Appendix 1: CSQ 15, 19–21; DMDSQ 14, 18–20) were analyzed using a deductive qualitative content analysis approach [23]. Responses were coded according to the International Classification of Function (ICF) for analysis. The ICF [24], a commonly used [25] and validated framework [26] that extends beyond medical diagnoses to classify functioning and disability on both the individual and population level, was used to create a categorization matrix following coding. The ICF framework is grouped into five domains: body functions, activities and participation, environmental factors, body structures and personal factors. Four of these domains have been classified into a hierarchically nested structure with up to four different levels (Fig. 1) that become more detailed as they unfold [24, 27].
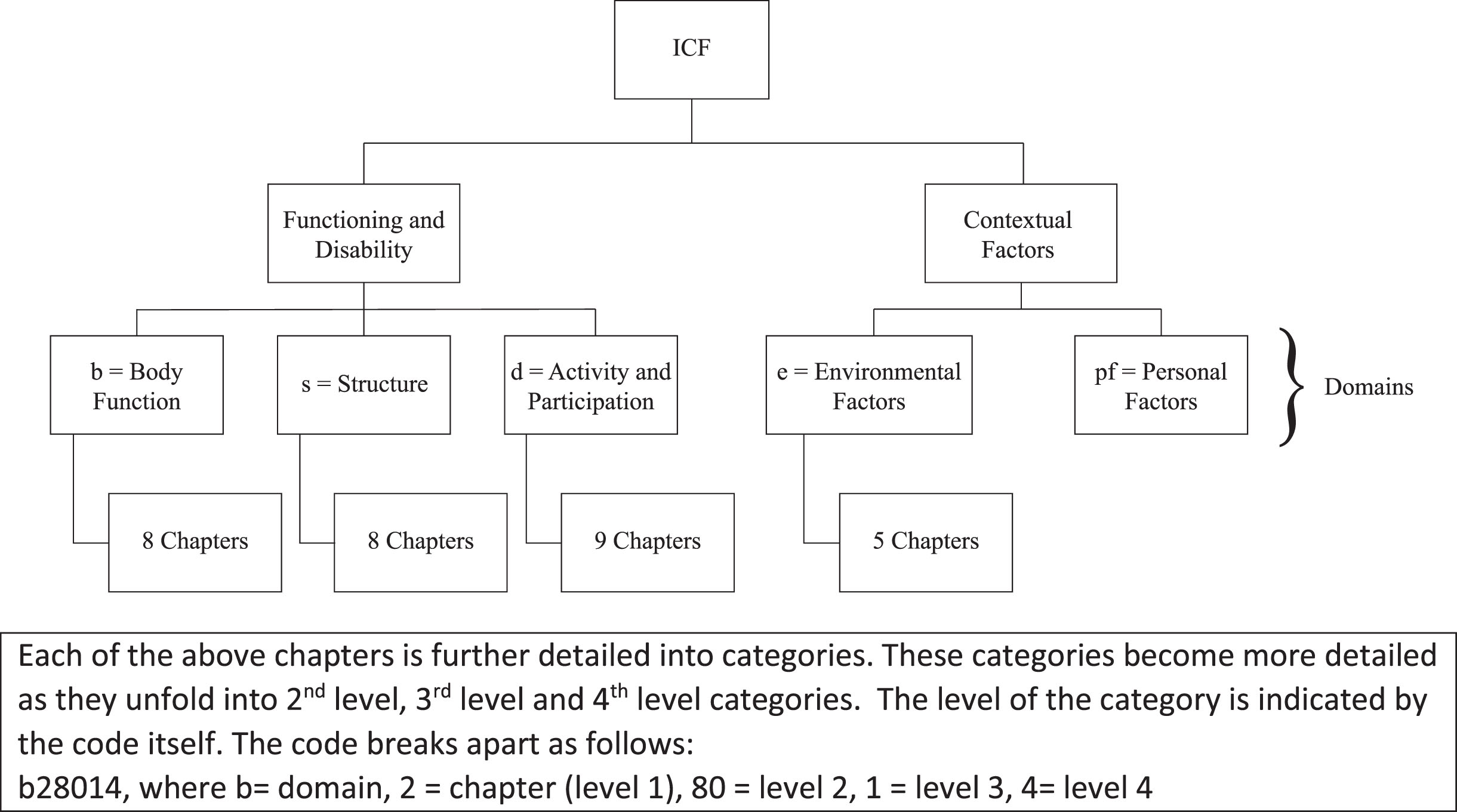
Taxonomy of the ICF.
Two neuromuscular physical therapists met multiple times to critically reflect on survey responses, review the responses for content, and code them to the first level (i.e., chapters) by using key words in the responses and aligning them with the chapter definitions [24, 26]. If responses contained information that was relevant across multiple chapters, then all relevant chapters were included. Descriptive statistics were computed using Microsoft Excel. Frequencies and percentages were derived for coded categorical variables.
Integration of the qualitative and quantitative results occurred as the categorical and open-ended survey responses were merged in a joint display [16, 28]. Meta-inferences (i.e., interpretations based on the qualitative and quantitative findings) were drawn to determine whether confirmation or disconfirmation occurred between the datasets [16, 28]. Confirmation occurred if the findings from both types of data reinforced the results from the other [28]. Disconfirmation occurred if the two datasets were inconsistent or disagreed with each other [28].
Results
One hundred and sixty-six respondents completed the survey (see Fig. 2). Fifteen surveys that were initiated were left blank, and four survey responses did not meet inclusion criteria and were therefore excluded. Of the 147 remaining surveys (response rate of 6.8%), 132 (89.8%) parents/caregivers and 15 (10.2%) adults with DMD completed the survey. Respondents’ characteristics can be found in Table 1.
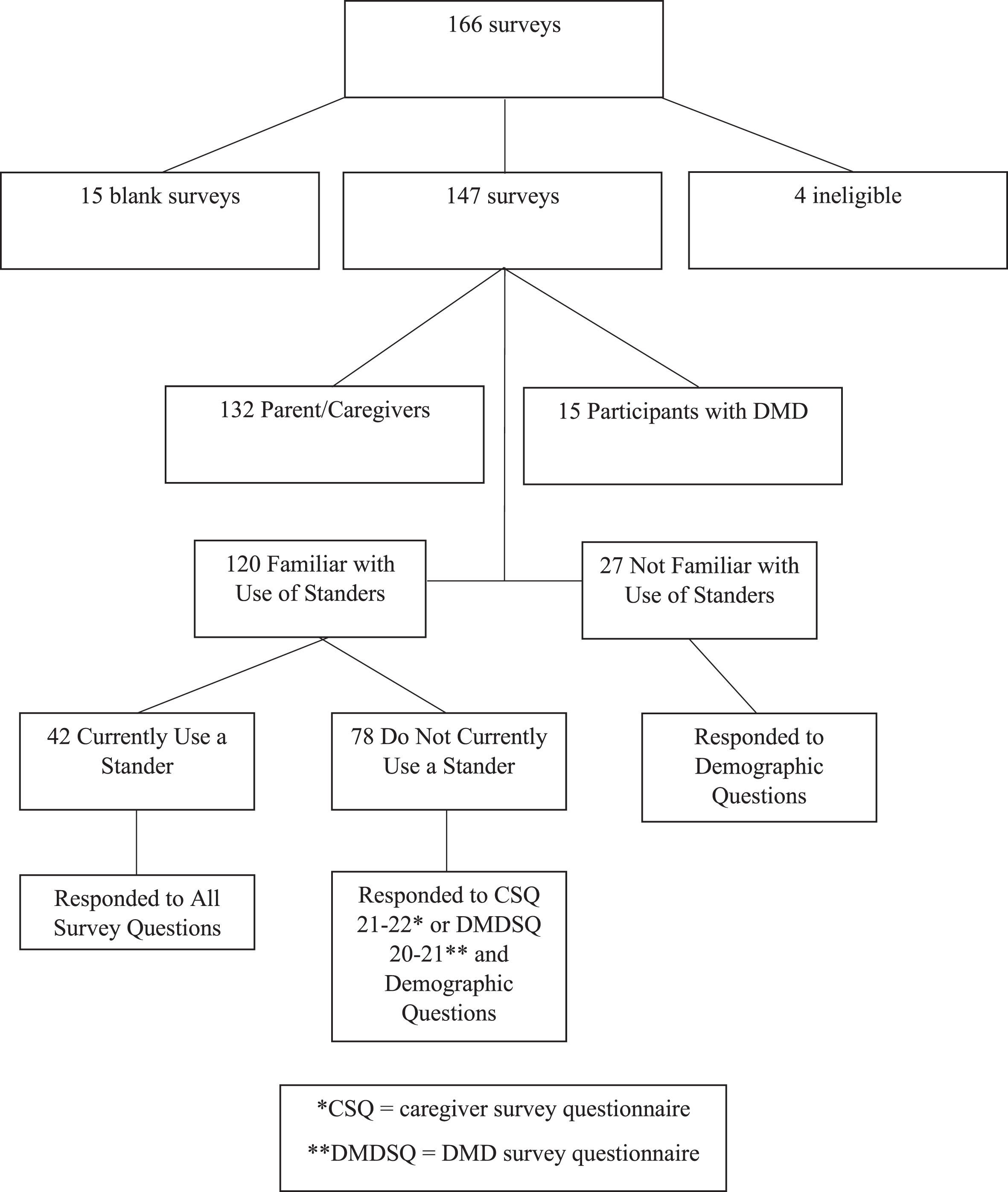
Eligibility flow chart.
Respondent characteristics
Note: Some survey respondents did not complete some demographic questions, so percentages may not total 100%. SD: standard deviation.
The analysis explored respondents’ familiarity with standers. One hundred twenty (81.6%) –108 parents/caregivers and 12 individuals with DMD –reported they were familiar with using standers for individuals with DMD. Forty-two respondents (28.6%) –38 parent/caregivers and 4 individuals with DMD –reported that the individual with DMD was currently using a stander. Hereafter, all responses from individuals with DMD and parents/caregivers are analyzed together. Statistics are reported for the total number of participants who responded to each question because respondents were not required to answer every question.
Questions specific to funding sources and parties who facilitated stander acquisition permitted multiple response options and are outlined in Table 2. Respondents reported similar methods of obtaining PSWs and STSs.
Respondents’ methods of obtaining standers
Respondents’ methods of obtaining standers
*Only 40 of 42 respondents commented on the type of stander they use. **Respondents selected all options that applied, so percentages do not total 100. PSW = power standing feature in a wheelchair. STS = sit-to-stand stander.
Participants were also asked to describe barriers to obtaining a stander (Table 3). Qualitative results coded according to the ICF revealed that environmental factors represented the most common hindrance, with nearly half (n = 16) of those who responded to this question reporting economic services challenges. These challenges were associated with cost, insurance approval/denial process, and time from ordering to delivery of the standing device. With seven respondents, activity and participation barriers related to furnishing a place to live (e.g., finding adequate space to store the stander) represented the second most common hindrance.
Survey responses categorized by International Classification of Function (ICF)
CSQ = Survey question for survey version administered to parents/caregivers; DMDSQ = Survey question for survey version administered to individuals with Duchenne Muscular Dystrophy.
The average age of LOA (defined here as the inability to walk 10 meters without assistance) for individuals with DMD was 13.6±3.0 years (range: 8–22). The average age at which individuals with DMD began using a stander was 13.9±4.0 years (range: 8–31). Seventeen of 42 respondents reported that the individual with DMD was ambulatory when stander use was initiated. Four of 42 respondents reported the individual with DMD using a stander was currently ambulatory. There was a positive correlation between age of LOA and age of start of stander use (r = 0.61, p < 0.0001, n = 36), with a later onset of LOA associated with a later initiation of stander use (see Fig. 3).
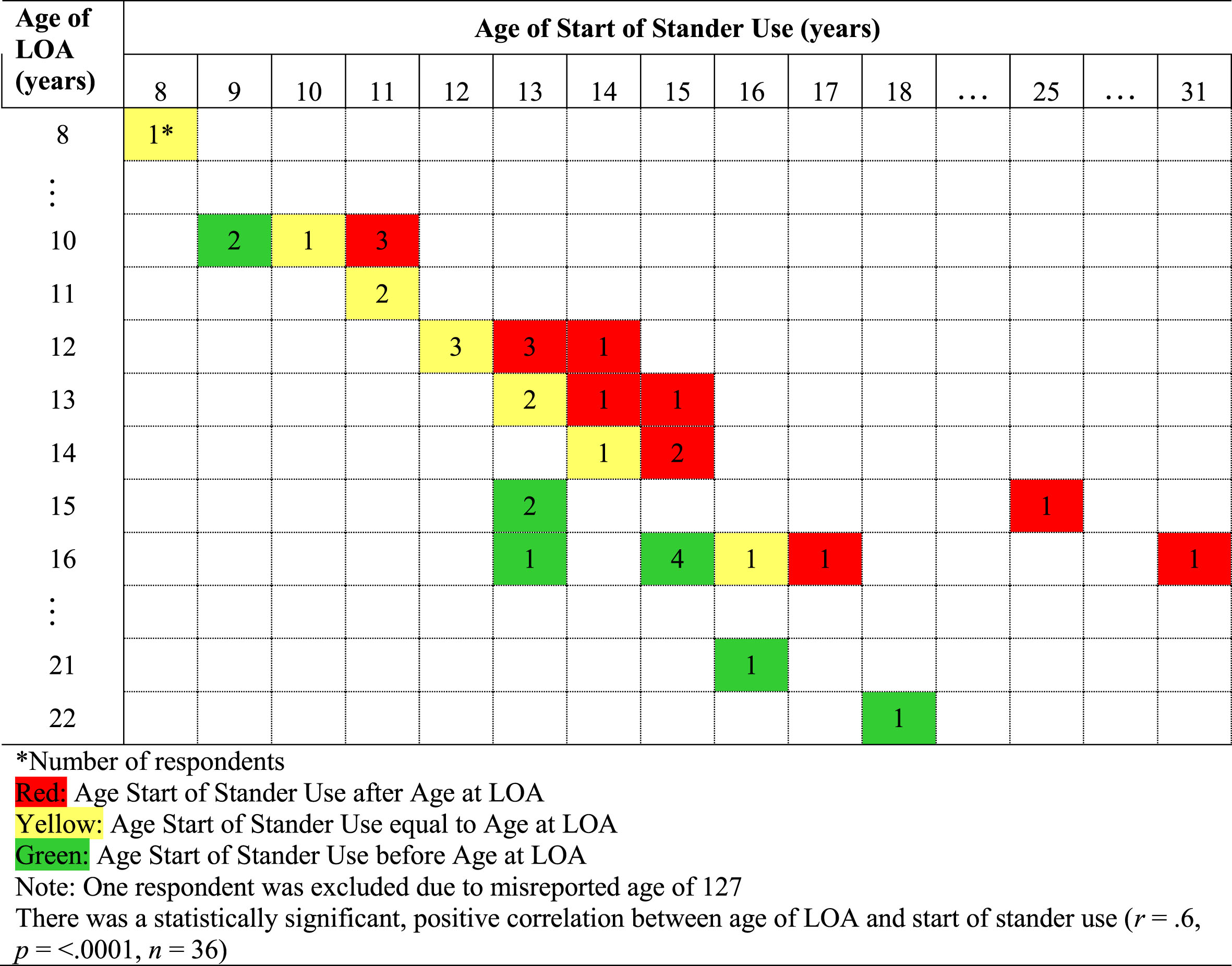
Comparison of Age of Loss of Ambulation (LOA) to age of start of stander use.
Of the 42 respondents who reported stander use, 13 reported using a PSW (including Permobil F5 and Permobil C400), and 27 reported using a STS as the stander type. Two respondents did not report the type they used. Regarding frequency and timing, respondents reported using the stander 4.5±1.7 days per week (range: 1–7) and 44.8±30.2 minutes per day (range: 10–180) on days when they used the stander. Most respondents (n = 31) reported spending their time in the stander all at once; fewer (n = 11) reported using the stander multiple times throughout the day. Half of the respondents (n = 21) reported the individual with DMD became fully upright when using the stander, seven became nearly upright, seven became moderately upright, and seven became mildly upright. Figure 4 illustrates comparisons of respondents’ frequency, intensity, and timing of use by stander type.
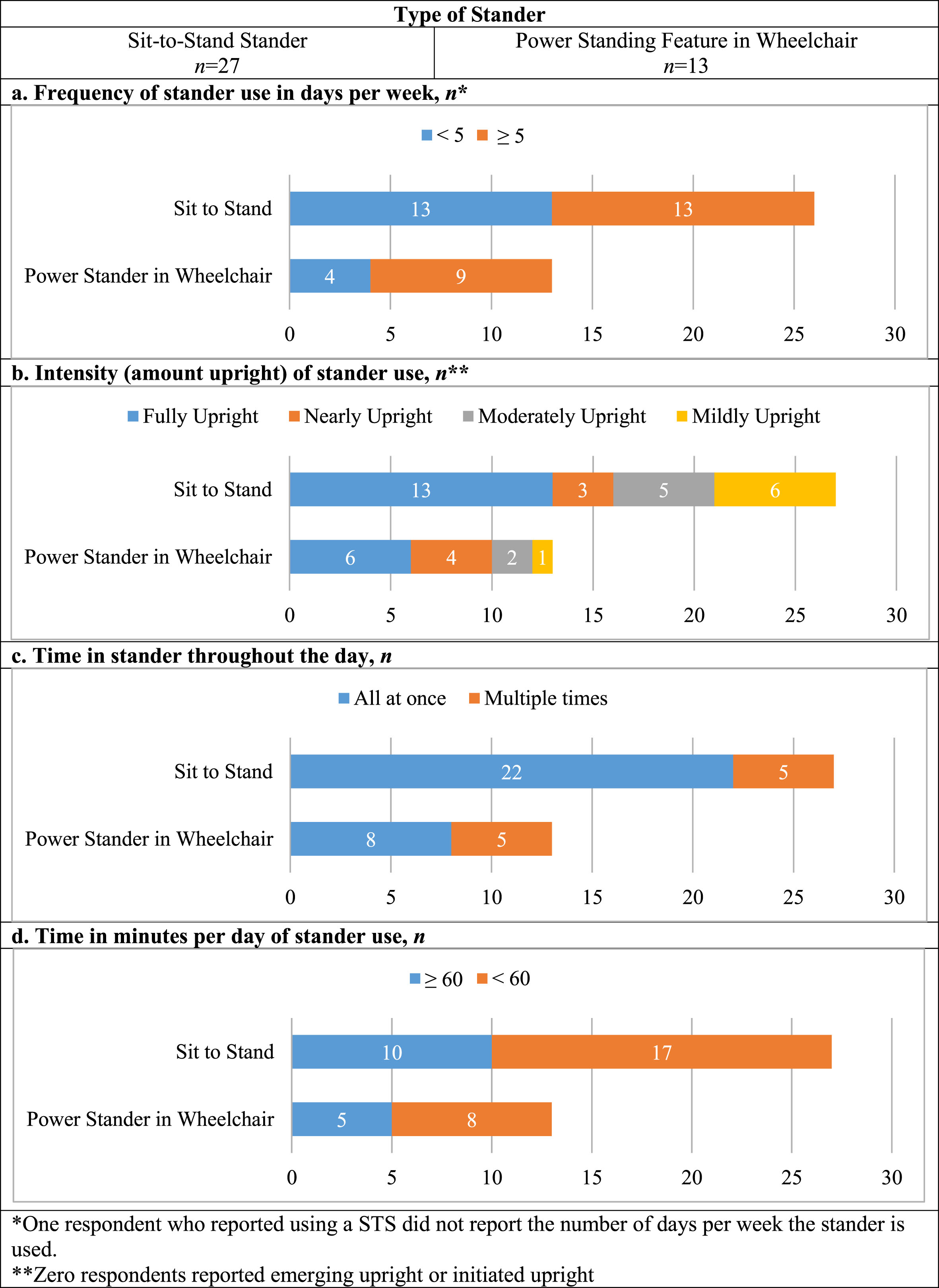
Comparison of Frequency, Intensity, and Timing by Type (FITT) of stander.
Of those who reported using a PSW or STS type, 10 participants reported standing at a dose of 60–90 minutes at least five days a week. Respondents’ number of days per week of stander use were not significantly less than five days per week (mean = 4.5, 95% confidence interval [CI] = 4.0–5.0, p = 0.06). Minutes per day of stander use were significantly less than 60–90 minutes (mean = 44.8, 95% CI = 35.4–54.2, p = 0.002). Similarly, respondents’ total dose was significantly lower than the recommended 300 minutes (mean value = 227, 95% CI = 165–289, p = 0.02). Additional analyses revealed no significant differences in use between stander types (STS or PSW) for either days per week (mean difference = –0.8, 95% CI = –1.9–0.4, p = 0.15) or minutes per day (mean difference = 1.5, 95% CI = –19.5–22.5, p = 0.87). The relationship between total dose and stander type was not significant (mean difference = –20.4, 95% CI = –154.7–113.9, p = 0.76).
Respondents were asked to report all locations in which they used their standers. Thirty-eight of the 42 respondents reported use at home, including 24 who used a STS, 12 who used a PSW, and two who reported using “other” stander types. Nine used their stander at school, one during therapy appointments, and four at “other” locations (e.g., “Voice rehearsal” [P3]). Seven respondents with a PSW and two with a STS reported stander use at multiple locations.
Perceptions regarding features of standers
Respondents also described preferred features of their stander. For the 42 respondents who were currently using a stander, the most preferred features in order of preference were the tray (n = 12), the ability to use the stander anywhere/anytime among PSW users (n = 9), the ease of adjustment and movement into the standing position among STS users (n = 8), the ability to move a STS within the environment (n = 2), and the supportive nature of the PSW (n = 1). While not directly “features” of a stander, some respondents reported benefits associated with stander use, including the ability to participate with peers and urinate while standing, as well as reporting that the stander helped with flexibility, bone density, and scoliosis prevention. One respondent also noted the stander was “fun to use” (P55).
Respondents also reported stander features they disliked. Nine respondents mentioned various components of the stander (e.g., arm rest height, tray height, head rest, knee pads, etc.). Equally disliked was the overall process for set up and optimal adjustment of the devices (n = 9). Other negative features included neither device being supportive enough (n = 3), the PSW not providing enough of a stretch (n = 2), the size/bulkiness of the STS (n = 5), and difficulty transferring into the STS (n = 5).
What would make using the stander easier
In response to the question, “What would make using the stander easier?” for those 42 respondents who were currently using a stander, 15 respondents reported overall improved design/product modification and reduced size of the devices would improve ease of use. Nine respondents reported that an altogether different product or incorporation of the stander into their power wheelchair would make it easier to use. Other responses included ease of transferring into the device (n = 4), nothing (n = 4), motivation for consistent use (n = 2), financial barriers (n = 2), and support for proper fitting of the device (n = 1).
Perceptions regarding importance/usefulness of standers
The 42 respondents who were currently using a stander also reported on the importance/usefulness of standers. Parents/caregivers completing the survey were asked why using a stander is important/useful from both their perspective and their child’s (Appendix 1: CSQ 19-20). Individuals with DMD completing the survey were also asked this question from both perspectives (Appendix 1: DMDSQ 18-19). When analyzing the results, the parent/caregiver perspectives were combined from both survey questions (Appendix 1: CSQ 20; DMDSQ 19), as were the individual with DMD perspectives (Appendix 1: CSQ 19; DMDSQ 18). Responses spanned all four domains of the ICF (Table 3). The majority of responses were best characterized in the body functions domain (n = 54), specifically within the mobility of joint functions chapter, with 24 from the individual with DMD’s perspective and 30 from the caregiver’s perspective. The second most common response (n = 32) was best characterized in the body structures domain, specifically the bones (i.e., bone health) chapter, with 12 from the individual with DMD’s perspective and 20 from the caregiver’s perspective. Additionally, there were multiple responses that spanned many chapters of the activities and participation domain (n = 39), 23 from the individual with DMD’s perspective and 16 from the caregiver’s perspective.
Reasons stander not used
All 120 survey respondents who were familiar with stander use for individuals with DMD were asked to share reasons that may prevent stander use, regardless of stander use history, and 111 responded (Table 3). Responses spanned the four domains of the ICF. The greatest number of responses aligned with the mobility of joint functions chapter (i.e., range of motion) of the body functions domain (n = 19) and the economic services chapter of the environmental services domain (n = 19). Other commonly reported barriers included the time management chapter of the body functions domain (n = 14) and the ensuring one’s physical comfort (n = 15) and walking (n = 13; e.g., “currently he is still ambulatory. . . ” [P117]) chapters of the activity and participation domain.
Integration of quantitative and qualitative results
The qualitative findings confirmed the quantitative results regarding initiation of stander use and the frequency and timing (duration) of stander use. The quantitative results informed when stander use was initiated and the frequency and timing of stander use. The qualitative analysis provided insights into why stander use was primarily initiated after LOA and at less than the recommended frequency and duration.
As illustrated in Table 4, individuals with DMD delayed stander use until after LOA due to a lack of education and awareness about the benefits of early initiation, perceptions of stander use prior to LOA, and difficulties with insurance approval. Lack of time and energy to complete a supported standing program and the presence of contractures that made it difficult for the individual with DMD to tolerate standing contributed to decreased duration of stander use.
Joint display of quantitative, qualitative, and mixed methods meta-inferences of stander use
Joint display of quantitative, qualitative, and mixed methods meta-inferences of stander use
The qualitative findings also confirmed the quantitative results indicating primary use of the stander within the home regardless of stander type and the use of the PSW in multiple locations. The preference for use of the stander in the home may be due to the time it takes to get set up comfortably in the stander and the perception of others when in the stander (Table 4). The versatility of a PSW to assist with specific activities outside of the home was consistent with the use of the PSW in multiple locations compared with those using a STS.
Other qualitative findings disconfirmed the quantitative results regarding stander type. Whereas the quantitative results revealed that more participants reported having a STS, the qualitative analysis revealed preferences for the PSW. Reported space limitations and difficulties with transferring in and out of a separate device (STS) illustrated these preferences. Economic and health services barriers, including limited insurance coverage, prolonged process for obtaining standers, and cost of a PSW, may explain this discrepancy (Table 4).
Despite evidence suggesting the efficacy of a supported standing program to improve the health of individuals with DMD [3, 9–14] and the perceptions of caregivers of and individuals with DMD on the importance/usefulness of standers demonstrated in this study, this work suggested that implementation is limited due to several barriers. This study reported on stander use in individuals with DMD including standing obtainment, initiation, dose, and type related to consistency and success of participating in a supported standing program. These results can help to inform clinical practice when analyzed in the context of the literature.
Families are best served by working with both a therapist and a medical equipment company when obtaining custom rehabilitative equipment such as a stander [30–32]. The role of the therapist may include awareness of the individual’s condition, expected progression, and optimal posture and alignment. The role of the medical equipment company may include knowledge of stander capabilities and options, as well as the ability to provide demonstrations. Although most respondents in the current study reported using a therapist in addition to a medical equipment company to assist in obtainment of the stander, the results suggested that medical providers and caregivers of and individuals with DMD still have decreased awareness around stander use, including the benefits of early initiation [3], delaying the process for stander acquisition.
Progressive muscle weakness and eventual LOA are hallmark symptoms of DMD [3]. As individuals reach the late ambulatory stage and approach LOA, decreased range of motion and knee contractures are associated with increased time spent in a static, seated position. Specifically, knee contractures greater than 20 degrees may develop soon after LOA [29]. Given that stander use may improve range of motion [12, 13], it may be beneficial to initiate stander use in the late ambulatory stage [3], prior to LOA and contracture development, to promote the best tolerance to a standing program. However, the current study revealed that most respondents initiated stander use after LOA.
Perceived quality of life is also markedly diminished in children with DMD as they experience declines in motor function and is associated with decreased participation in physical activities [8]. Participation in a supported standing program is associated with advantages to mental health in adolescents with DMD [11]. Individuals in the current study perceived supported standing to positively impact activity and participation. Caregivers of and individuals with DMD reported standers to be important and useful for many areas of activity and participation including standing at eye level with others and standing for daily living, school, and recreational activities. This highlights the potential positive impacts of supported standing on quality of life and mental health and should be further explored.
Furthermore, the majority of respondents were not participating in a standing program at the recommended dose of five days per week for 60–90 minutes per day [13, 14]. Many respondents commented that barriers included pain, pressure, discomfort, and contractures. Further prospective research is needed to explore whether initiation of a standing program prior to LOA would minimize these barriers and allow obtainment of the recommended dose. Additionally, the burden of time also limits the ability to complete the recommended stander dose. This emphasizes the need for health care providers to work with families to explore options for reducing the overall healthcare burden and to develop a reasonable plan for implementation of a standing program.
When comparing STS to PSW, respondents reported preferences for the PSW due to its advantages of mobility and lack of need to transfer into the device. However, the number of PSW and STS users who reported using their standers within the recommended duration were comparatively similar. This suggests the advantages of the PSW may not necessarily make it easier to use throughout the day or do not outweigh other barriers reported, including perceptions of others while standing in the stander and the time it takes to get set up comfortably in the stander.
Many respondents reported difficulties related to funding and insurance processes in obtaining a stander. More individuals had the STS than the PSW due to economic and health services barriers, including insurance limitations, that delayed acquisition of the stander. Some respondents also reported structural barriers that impacted their ability to obtain and use the stander, including the size of the equipment impeding use in built environments. The responses provided by caregivers of and individuals with DMD highlight the need for advocacy regarding the benefits of stander use in individuals with DMD to insurance companies. Responses also emphasized the need for policy change to promote earlier access to standers and accessibility of standers in built environments.
In summary, given the totality of the results, clinicians should consider how DMD impacts all domains of the ICF and use this information when discussing disease progression and potential interventions, including supported standing. Clinicians should specifically promote open dialogue around how caregivers of and individual’s with DMD might implement a supported standing program into their daily routine, how it might provide positive benefits to their quality of life, and any perceived barriers to implementation. These discussions should occur well in advance of LOA to allow optimal time for decision making to occur and to determine if and when a supported standing program should be initiated. If a supported standing device is pursued, clinicians should use a team approach in which the family, therapist, and medical equipment provider collaborate to select the most appropriate device for the individual with DMD to support all areas of the ICF. Knowledge translation of the key clinical findings from this study can assist in clinical uptake of these recommendations.
Strengths and limitations
Combining the quantitative data with the qualitative data in the mixed methods analysis provided a better understanding of stander use than either form alone and allowed for triangulation of findings [17]. By expanding on the quantitative data, the qualitative findings provided greater insight into potentially modifiable barriers to stander use. This study was limited by factors inherent in any cross-sectional survey [33]. Specific to this study, individuals may have received the survey through two different recruitment methods, thus reducing the response rate. As this study utilized a sample of convenience and the response rate was low, it may not be representative of the DMD population at large. When responding to demographic questions, the majority of respondents reported having private rather than public insurance and reported an annual household income of over $80,000, which may have influenced the variability of responses.
Consistent with prior research [15], few respondents reported stander use, which further limited the generalizability of the findings. While there were limited responses from individuals with DMD, it is possible that a caregiver and their adult child with DMD may have both completed the survey and thus potentially overrepresented their experiences. While two authors participated in the qualitative analysis, independent coding was not feasible. However, due to the clarity of the codes based on the definitions available for the ICF chapters, this does not likely constitute a substantial limitation.
Conclusions
This mixed methods study provides a greater understanding of stander use among a select group of respondents with DMD and their caregivers. It provides insight to overall utilization and compliance as well as perceived benefits and barriers to consistent use and is the first study to report on these factors. It is important that clinicians discuss and consider perceived challenges and benefits with individuals with DMD prior to experiencing complications of disease progression that suggest limited stander tolerance, as reported by the respondents of this survey. This information may allow better informed decision making about the device that is best for the individual with DMD to optimize use prior to onset of body structure and function complications and reduce the urgency of obtaining the equipment. Awareness of perceived barriers and benefits may give the individual with DMD a greater opportunity to meet stander dosing recommendations to promote optimal health despite heavy economic and health services burdens. Medical professionals who manage individuals with DMD may utilize this data to further aid in discussions and individual treatment plans surrounding supported standing programs.
Footnotes
Acknowledgment
Authors thank Parent Project Muscular Dystrophy (PPMD) for their assistance recruiting participants, and we thank the families who participated in this study.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
Respondents were informed that completion of the survey implied consent. The study was reviewed and approved by the Institutional Review Board with initial approval date of January 19, 2019, and approval number 2018-8021.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.