
Abstract
PURPOSE:
Currently, there is a paucity of studies on the prevalence of Elimination Disorders among Iranian children and adolescents. Due to the ongoing need to monitor the health status of these children and adolescents, the present study aims to investigate the prevalence of Elimination Disorders and comorbid disorders in Iranian children and adolescents.
METHODS:
In this cross-sectional study, 29,781 children and adolescents age 6 to 18 years old were selected and studied from all the provinces in Iran. The sampling was carried out by employing a multistage cluster sampling method, and several clinical psychologists using semi-structured interviews collected the data. Furthermore, clinical psychologists collected demographic information (including information about gender, age, place of residence, education level, and parental education level). The collected data were analyzed using SPSS version 20.
RESULTS:
Generally, the prevalence of Elimination Disorders was found to be 5.4% covering both enuresis (
CONCLUSION:
The prevalence of Elimination Disorders in Iranian children and adolescents is moderate compared to similar studies elsewhere. As for comorbid disorders, ADHD and Separation Anxiety were found to be the most prevalent disorders. Since Elimination Disorders coexist with psychiatric disorders in children, further studies of these comorbidities may give better insight into the treatment and prognosis of Elimination Disorders.
Introduction
A health issue in children and adolescents is Elimination Disorders, which include the urinating disorder (enuresis and encopresis) and the defecating disorder (encopresis). They are associated with the loss of bladder/bowel control and seem to be related to the age and physical development of children [1]. Enuresis can be described as the release of urine during sleep without any organic cause in children beyond the age of 5. This disorder is commonly seen in three types: nocturnal, diurnal, and the combination of both. The diagnostic standard for enuresis in children is based on the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders-American Psychiatric Association, 2013). According to the DSM-5, enuresis refers to the repeated voiding of urine at least three times a week for three or more consecutive months, or when it is accompanied with other clinical criteria such as anxiety and dysfunction [2]. The prevalence of enuresis has been reported to be 5% to 10% in 5-year-old children, 1.5% to 5% in children aged between 9 and 10, and 1% in adolescents aged 15 and older [3]. Another Elimination Disorder is encopresis which refers to repeated defecation occurring intentionally or unintentionally in places other than the toilet in children over 4 years old [3]. The prevalence of encopresis has generally been reported to be 0.8% to 7.8% [4].
A study in the Netherlands (2005) on the Elimination Disorders (population
It is well established that Elimination Disorders have multifactorial etiology. Some contributing factors include arousal disorders, changes in the secretion of anti-urogenital hormones, psychological factors, genetic factors, delayed puberty, and parents’ ages and education levels [8, 9]. A study investigated the factors influencing Elimination Disorders and reported parental education level, income of the family, and age of the children as the main factors contributing to enuresis [10]. In the UK, the prevalence of enuresis was found to be 14.2% and the total prevalence of Elimination Disorders was estimated at 11.4% per 8,000 children younger than 7 years old [11].
Diagnosis of Elimination Disorders requires assessing several factors including checking the history of symptoms (e.g., frequency, periodicity, and duration of symptoms), assessing children’s mental status (children’s views and misconceptions), and physical examinations [12]. In addition, the presence and absence of factors such as comorbid psychiatric disorders need to be taken into account as these factors can significantly affect the treatment options for children with Elimination Disorders. For instance, enuresis is more difficult to treat in children with ADHD (Attention Deficit Hyperactivity Disorder). It has been reported that children with ADHD suffering from nocturnal enuresis are less responsive to alarm treatment [13]. Alarms include moisture sensors that give signals (sound or vibration) to avoid enuresis. In the Iranian context, Elimination Disorders are mainly diagnosed and treated by urologists and psychiatrists. First, a urologist does the physical examinations and then a psychiatrist does the psychological assessment. Patients either personally visit the urologists or they are referred by other health professionals. However, less attention is paid to the comorbid disorders of the patients.
Clinical evidence has shown that there is a relationship between psychiatric problems (such as chronic fatigue and ADHD) and Elimination Disorders [12]. Comorbid psychological problems are found in 20% to 40% of children with diurnal urinary incontinence [14, 15]. A study on 8,213 children aged 7.5 to 9 years old found that ADHD (24.8%), separation anxiety (11.4%), conduct problems (11.8%), and Oppositional Defiant Disorder (ODD) (10.9%) coexist with daytime urinary incontinence [16]. A treatment approach that focuses on symptoms may suffice for most children. However, when there are psychiatric disorders co-occurring with Elimination Disorders, more than a symptom-oriented approach is needed. For proper treatment, additional therapies such as psychotherapy, counseling, and pharmacotherapy could be needed [15].
The health status of children and adolescents needs to be monitored continuously. The present study focused on Elimination Disorders and the comorbidities in Iranian children and adolescents. It is the first epidemiological investigation of Elimination Disorders and psychiatric comorbidities in a large statistical population of Iranian children and adolescents. Given that diagnosis and treatment of Elimination Disorders requires assessing and handling the comorbid disorders as well, knowing about the prevalence of comorbid disorders in children with Elimination Disorders would be helpful in deciding how much priority and consideration should be directed to the assessment of comorbid disorders for treating Elimination Disorders.
Method
Study design
The present study is part of a national project for estimating the prevalence of psychiatric disorders in Iranian children and adolescents. It was a cross-sectional survey carried out in 29 provinces of Iran with the aim of investigating the prevalence of psychiatric disorders in children and adolescents aged 6–18 years old [17].
Subjects
In total, 29,781 children and adolescents aged 6 to 18 were selected to participate in the study. Before selecting the subjects (sample) for the study, it was deemed necessary to estimate the sample size and determine the inclusion criteria. The participants were selected using a multi-stage cluster sampling method from the 6 to 18 year-old population living in urban and rural areas (proportional to population size) of all the provinces of Iran. Clusters of houses (170 clusters) were randomly selected using postal codes. In each cluster, blocks of 6 children and adolescents were randomly selected equally from each gender and age group (6–9 years, 10–14 years, and 15–18 years).
Data collection instrument
Kiddie-Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL)
K-SADS-PL is a semi-structured interview to collect data on psychiatric disorders in children [18]. It has been designed and written by Kaufman et al. and is compatible with the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV. The DSM is the diagnostic tool for mental disorders published by the American Psychiatric Association (APA). In many parts of the world including Iran, the DSM serves as the principal authority for diagnosing psychiatric disorders. The current study used K-SADS-PL DSM IV for identifying the psychiatric disorders in children and adolescents although K-SADS-PL DSM V is more commonly used nowadays. The reason for the use of K-SADS-PL DSM IV in the current study was the availability of its valid and reliable Farsi version for the Iranian population when the study was initiated. Accordingly, data collection and diagnosis were based on the DSM IV. It should be noted that diagnoses were made by the interviewers but the researchers made the final scoring and analysis.
K-SADS-PL is used for children aged 6–18 and has been designed to assess the current and past episodes of psychiatric disorders in children and adolescents. It includes five diagnostic categories: 1) Mood Disorders including Depression (major Depressive disorder and Dysthymia), Mania, and Hypomania; 2) Psychosis Disorders; 3) Anxiety Disorders including Social Phobia, Agoraphobia, Specific Phobia, Obsessive-Compulsive Disorder, Separation Anxiety Disorder, Generalized Anxiety Disorder, Panic Disorder, and Post-Traumatic Stress Disorder; 4) Behavioral Disorders including ADHD, Conduct Disorder, ODD; and 5) Substance Abuse, Tic Disorders, Eating Disorders, enuresis, and encopresis [18, 19]. The consensual validity of all of the categories of Persian K-SADS-PL has been reported to be good to excellent and test-retest reliabilities of the categories have reported to be between 0.56 and 0.81 [20]. The Kappa interrater reliabilities of K-SADS-PL have been reported between 0.66 and 0.81 (
Procedure
Training the interviewers
Data collection was performed by 250 interviewers who were trained in proper data collection using the K-SADS-PL. The training included instructions on how to interview the children and their parents using the K-SADS-PL items and also how to observe interviewing ethics such as using polite tone, focusing on the purpose of the interview, and observing privacy. In addition, interviewers were instructed to inform the interviewees about the data collection process and to ensure the parents about the confidentiality of the collected information. The interviews were done with children and their parents (particularly mothers).
Data collection
After gaining the informed consent of the participants, the data for the project were collected through clinical interviews with children and their parents using the K-SADS-PL. To do so, the K-SADS-PL was installed on the interviewers’ tablets and was completed for each participant through interviewing the children and their parents. The collected data were sent to a central server for analysis. The interview began with some demographic questions followed by questions about previous psychiatric complaints. To collect data from children, parents were initially interviewed; adolescents were interviewed directly.
It should be noted that a monitoring process was also delineated to ensure that data were collected from all the sample clusters. This monitoring process included a GPS tracking mechanism that tracked all the traveling locations of the interviewers. Furthermore, interviewers were frequently called to make sure that data were collected properly.
Ethics
Informed consent for participation in the study was obtained from the participants (for children younger than 15 years, informed consent was obtained from their parents, and for those aged between 15 and 18, informed consent was obtained from the children themselves or their parents). To encourage participation in the study, confidentiality of the participants’ information was assured. In addition, families were assured that they would receive free consultation for their children’s conditions by the psychiatrists if their children were suspected to be suffering from Elimination Disorders and comorbid conditions. The consultations were given immediately after the interviews. This research was approved by the ethics committee of National Institute for Medical Research Development (NIMAD) (code of ethics: IR.NIMAD.REC.1395.001) and sponsored by the National Institute for Medical Research Development (NIMAD).
Data analysis
The data were analyzed using SPSS v. 20. Descriptive analyses were used to determine the frequency of psychiatric disorders and Elimination Disorders in children and adolescents. The confidence interval was considered 95% (
Rates of comorbid disorders in Elimination Disorders in children and adolescents in Iran (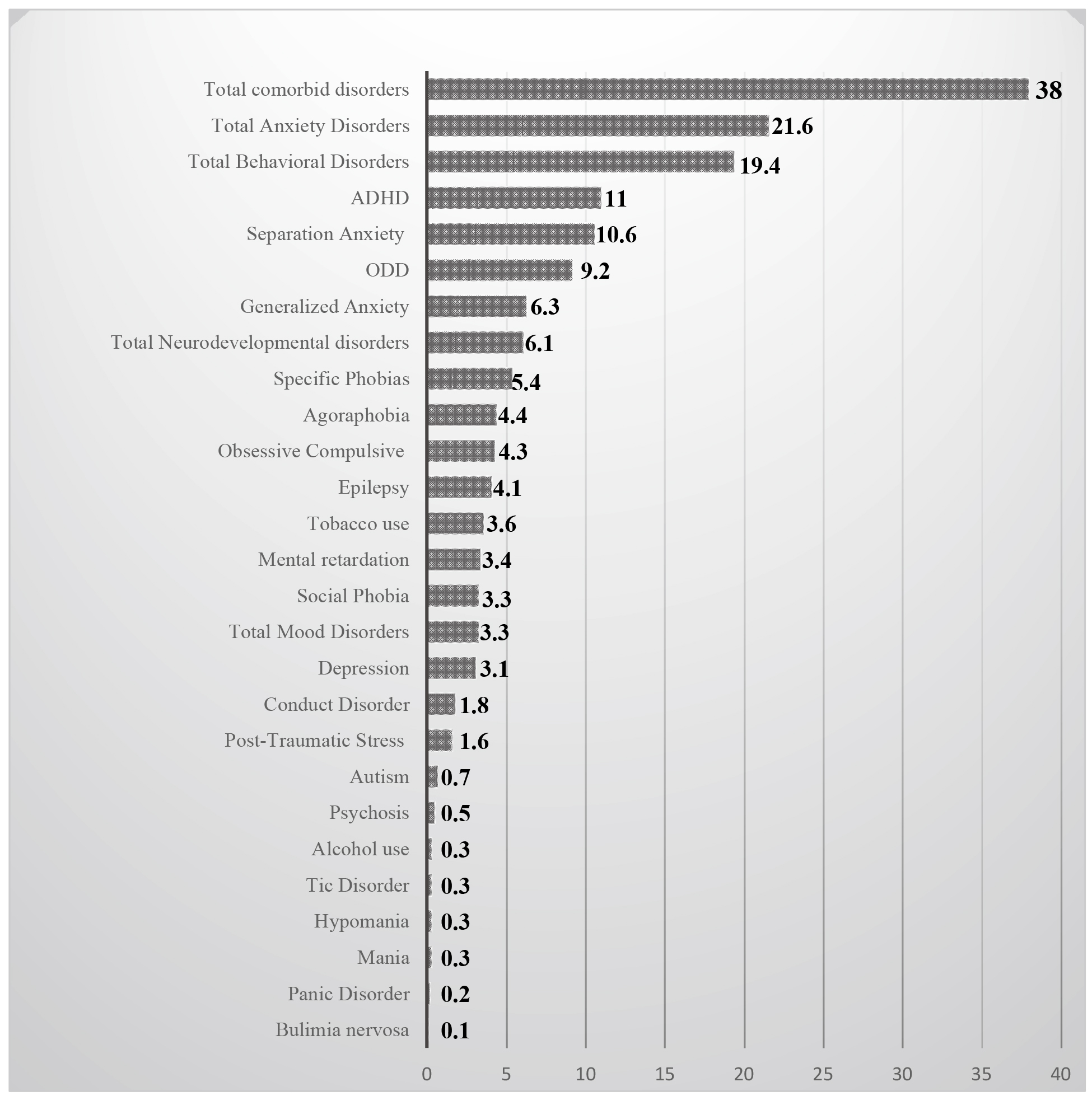
In total, 29,781 individuals participated in the study and fully completed the K-SADS-PL. Based on the results of the data analysis, 1,535 individuals were diagnosed with Elimination Disorders (5.4%) and 28,246 individuals without (94.8%). In general, the prevalence of Elimination Disorders was estimated to be 5.4%. The prevalence of enuresis was found to be 5.4% and that of encopresis 0.13% (Table 1).
Frequency and prevalence of types of Elimination Disorders in children and adolescents in Iran (
29781)
Frequency and prevalence of types of Elimination Disorders in children and adolescents in Iran (
The results of the analyses indicated that the prevalence of Elimination Disorders was
Socio-demographic characteristics of the children and adolescents
Odds ratios (95% CI) for Elimination Disorders based on socio-demographic characteristics in children and adolescents in Iran
OR adjusted: Odds Ratio. CI: Confidence Interval.
Prevalence of comorbid psychiatric disorders in children and adolescents with Elimination Disorders in children and adolescents in Iran
The results of the Chi-square test showed a significant relationship between gender and Elimination Disorders (
The investigation of comorbid psychiatric disorders in 583 children and adolescents with Elimination Disorders showed a total prevalence of
The current epidemiological study with a sample size of 29,781 can adequately reflect the prevalence of Elimination Disorders in Iranian children and adolescents. It is the first study of its kind in the Iranian population with such a large number of participants. We found the total prevalence of 5.4% for Elimination Disorders in children that included a prevalence of 5.4% for enuresis and 0.13% for encopresis. Similar studies in Germany have explored the prevalence of Elimination Disorders and reported a prevalence of 9.5% for enuresis and 1.2% for encopresis [20, 21]. Similar studies conducted in England and Australia reported the prevalence of enuresis to be 17% and the prevalence of encopresis to be 10% in children older than 7 years old [9, 22]. Findings of other studies in countries like the United States (4.45%), Hong Kong (3.1%), and Sudan (3.44%) are relatively in line with the results of the present study (23–25). The prevalence of Elimination Disorders has been reported to be 37% in Nigeria [8], 11.5% in Egypt, and 20.8% in Ethiopia [26], all of which are much higher than the prevalence reported in the current study. Aside from the contextual differences between the countries mentioned above, methodological differences (differences in sampling, participants’ age groups, data collection procedure, etc.) between the studies may account for differences in the prevalence of Elimination Disorders in these countries. For instance, studies in Sudan and Ethiopia included 816 and 1547 individuals respectively while the current study included a sample of 29,781 individuals.
Factors related to Elimination Disorders
In this study, the sex ratio of the prevalence of Elimination Disorders was found to be 1.2 (the ratio of girls to boys) [OR
The analysis of Elimination Disorders in connection with the place of residence (urban/rural areas) suggests that the chance of having Elimination Disorders is higher in children living in urban areas compared to those living in rural areas (OR
The analysis of the survey on the level of parental education indicates remarkable results. The adjusted odds ratio of the prevalence of Elimination Disorders especially enuresis is 2.5 times higher in children with parents with a primary school education level compared to other education levels (OR
Based on the results of the present study, the prevalence of comorbid psychiatric disorders alongside Elimination Disorders are observed in 38% of the children. This finding further supports the previous literature on prevalence of comorbid disorders in children with Elimination Disorders [15, 30, 38, 39]. The current study showed that the category of anxiety disorders is the most prevalent comorbid psychiatric disorder (21.6%) followed by Separation Anxiety (10.6%), which is in line with previous findings [3, 15, 23, 39, 40]. Similar studies have been conducted in Germany and show that Anxiety and Depression are more prevalent in children with Elimination Disorders (17.8%) compared to children without Elimination Disorders (12.7%) [11, 20, 41, 42]. A study carried out by Jensen et al. reviewing the comorbidity of mental disorders in children and adolescents showed that Elimination Disorders are strongly related with ADHD and Conduct Disorders [43].
Implications
The findings of the current study have implications for both diagnosis and treatment of Elimination Disorders in children and adolescents. The prevalence of Elimination Disorders was 5.4% in children and adolescents. The initial step for proper diagnosis and treatment of Elimination Disorders could be increasing parents’ awareness about this health problem. A study found that only 9.8% of the parents are aware of enuresis as a health problem [30]. Since parents are mainly responsible for seeking treatment, adequate instructions are needed for raising family awareness about enuresis and encopresis as health problems.
The prevalence of Elimination Disorders varies with age, sex, parental education, and family’s place of residence (urban and rural areas). This indicates that treatment policies should prioritize treatment components with such variations. Elimination Disorders were more prevalent in boys, which suggests making families with male children more aware of enuresis and encopresis. Mothers with higher levels of education had fewer children with Elimination Disorders. One possible explanation could be that parents with higher levels of education may have access to more sources of information for raising their children and dealing with their problems. However, more empirical studies are needed to confirm the relationship between parents’ education levels and the prevalence of Elimination Disorders in children and adolescents.
All these issues point to the inclusion of variations in the prevalence of Elimination Disorders in health decision making processes for proper management of Elimination Disorders in children and adolescents. Currently, a systematic procedure for diagnosis and treatment of Elimination Disorders seems to be missing in Iran. For future plans, decision makers may attend to, not only the symptoms of Elimination Disorders, but also to sources of variations such as parents’ levels of education and gender of the children. For instance, families with lower levels of education may need more surveillance and education, and families with male children need to be made more sensitive to Elimination Disorders and related problems.
Another finding was the presence of comorbid disorders in children and adolescents. The fact that Elimination Disorders are comorbid with different types of psychiatric disorders suggests that a thorough diagnosis requires not only seeking the symptoms and physical examinations but also a complete survey of the comorbid disorders. We particularly found that Separation Anxiety and ADHD were the most prevalent comorbid disorders. Accordingly, special attention needs to be paid to Anxiety Disorders and ADHD in the diagnosis and treatment of Elimination Disorders. It is quite possible that these two comorbid disorders are among the major risk factors for Elimination Disorders. Diagnosis of psychiatric disorders can be done through proper psychiatric assessment. A child’s psychiatric assessment could be done by identifying the psychological problems using standardized classification schemes such as the DSM and psychological tests. Therapeutic intervention needs to be started after complete diagnosis of the comorbid problems [15]. A child with ADHD may not be a good candidate for enuresis alarm therapy as the comorbid ADHD lowers the success rate of enuresis alarm. Disorders that are comorbid with enuresis and encopresis may affect both prognosis and response to therapies [15].
Conclusion
The prevalence of Elimination Disorders, mainly enuresis in Iranian children and adolescents is moderate compared to similar studies elsewhere (see the Introduction section). These disorders are significantly related to the child’s age and sex as well as parental education, family’s place of residence (urban and rural areas), and the children’s comorbid conditions such as anxiety disorders (e.g., separation anxiety), and behavioral disorders (e.g., ADHD). The findings also indicate that the prevalence of comorbid psychiatric disorders (e.g., ADHD and Anxiety Disorders) is high in children with Elimination Disorders. Given the comorbidity of Elimination Disorders and psychological problems, further studies are needed to determine proper management of Elimination Disorders in children and adolescents with comorbid psychiatric disorders. It is also suggested that screening for Elimination Disorders be part of children’s health screening. Such screening may facilitate the timely diagnosis and treatment of Elimination Disorders in children and adolescents.