
Abstract
Background:
Mother-to-child transmission of the HIV remains the main source of HIV infection in children. Targeting pregnant women attending antenatal care follow-up provides a unique opportunity for implementing prevention of mother-to-child transmission programs against HIV infection in newborn babies.
Objective:
The objective of this study was to assess the prevalence of HIV infection and associated factors among infants born to HIV-positive mothers in the prevention of mother-to-child transmission clinic in the Gondar city health institutions, Northwest Ethiopia, 2021.
Methods:
Documents were reviewed at the facility. Infants who had been exposed to HIV were enrolled in the study from 1 May–20 June 2021 prevention of mother-to-child transmission service in Gondar health institutions. To collect data from the charts, a structured data extraction tool was developed. The data were entered and analyzed with SPSS version 25 software. Both bivariate and multivariate logistic regression models were fitted to identify factors associated with HIV infection. The crude and adjusted odds ratios with a 95% confidence interval were calculated to determine the significance level.
Result:
The prevalence of HIV infection among infants born to HIV-positive mothers at the prevention of mother-to-child transmission level was found to be 8.1% (95% confidence interval = 7.3–12.9). Mixed infant feeding practice (adjusted odds ratio = 5.15, 95% confidence interval = 1.82–14.56), mothers’ lack of education (adjusted odds ratio = 3.43, 95% confidence interval = 2.26–5.0), absence of antenatal care follow-up (adjusted odds ratio = 1.82, 95% confidence interval = 1.17–4.02), and home delivery (adjusted odds ratio = 2.24, 95% confidence interval = 2.10–7.45) were statistically significantly associated with infants’ HIV infection.
Conclusion:
The prevalence of HIV infection in babies born to HIV-positive mothers was found to be high. Significant factors include mixed infant feeding practice, mothers’ lack of education, antenatal care follow-up, and home delivery. We also proposed that skilled delivery care and community education could reduce HIV transmission from mother to child.
Keywords
Introduction
In 2011, approximately 330,000 children were infected with HIV worldwide, with over 90% of these infections occurring in sub-Saharan Africa, primarily through mother-to-child transmission. Twenty-two countries account for more than 90% of the global burden. Ethiopia is one of these priority countries, where one in every three children born to HIV-positive mothers is infected with the virus.1,2
In Ethiopia, an estimated 5.74% of pregnant women have HIV and one in every three children born to these women has HIV. HIV testing during pregnancy and taking antiretroviral drugs (ARTs) help prevent HIV transmission from mother to child (MTCT).3,4 However, in Ethiopia’s Amhara region, only 24% of HIV-positive pregnant women have received the medication needed to prevent MTCT. 5
Disease progression is aggressive in the first months of life in infants who acquired the infection in utero or around delivery. 6 If left untreated, almost half of these children will die before 2 years of age and 75% by 5 years. Most of these deaths in children with HIV could have been avoided through early infant diagnosis (EID) and the provision of effective care and treatment.7,8 Interventions such as the use of ART by infected pregnant women, safe delivery practices, and safe infant feeding have helped reduce the risk of transmission to infants (from 40% to 5%).3,6 Observing this, the Government of Ethiopia has been accelerating the expansion of the prevention of mother-to-child transmission (PMTCT) of HIV service by promoting antenatal care (ANC), free of charge.9,10 To eliminate the infection in children and keep mothers alive, a comprehensive package of interventions, including but not limited to preventing women from becoming infected with HIV; eliminating MTCT throughout pregnancy, delivery, and breastfeeding by providing effective medications; and providing appropriate HIV treatment, care, and support for mother and children, has been underscored. 11
Ethiopia is one of the largest epidemic countries in sub-Saharan Africa. The national HIV prevalence estimate was 1.5%, but the prevalence in women was 1.9% in 2011.12,13 Increased incidence of HIV in a pregnant woman would ultimately lead to increased incidence of HIV in children. Among the total of 137,494 new HIV infections, 10% were children infected mainly due to vertical mother-to-child transmission of HIV. 14 Therefore, this study assessed the prevalence of HIV infection and associated factors among infants born to women living with HIV attending PMTCT service at Gondar town health institutions.
Methods
Study design and period
This is a facility-based retrospective cross-sectional study designed from 15 May to 30 June 2021 to collect data from registration and follow-up log books in the PMTCT and HIV-exposed infants (HEIs) follow-up units.
Study area and settings
This study was carried out in Gondar town health institutions. Gondar is located in the northwest part of the Amhara regional state and is 728 km northwest of Addis Ababa, the capital city of Ethiopia, and 175 km from Bahar-Dar, the capital of the Amhara regional state. Gondar town has 22 Kebele with a projected population of 327,668 (Gondar Zonal Statistics Office). In this town, there is one governmental referral hospital and seven health centers that provide PMTCT services, and the study was conducted at each of these locations.
Study population
Source population
All infants born to HIV-positive mothers attended PMTCT services in the Gondar city health institutions.
Study population
All infants born to HIV-positive mothers attended PMTCT services in the Gondar city health institutions during the study period.
Inclusion and exclusion criteria
Inclusion criteria
All HEIs born from HIV-positive mothers in Gondar town health institutions were included in the study.
Exclusion criteria
All infants exposed to HIV during breastfeeding who did not have confirmatory HIV tests until the end of data collection and all infants who do not have alive mothers were excluded.
Sample size estimation
Sample determination size for prevalence
The sample size for the study was determined using an Open-Epi Version 2 software considering the following assumptions: According to the study done at the University of Gondar hospital, Northwest Ethiopia in 2013, the prevalence of HEIs was 10.1%. 7 Based on this assumption, the actual sample size for this study is computed using the single population proportion formula as follows: 5% marginal error and 95% confidence interval (95% CI). The sample size was determined using the following formula: n = (z2p (1 – p)) / d2, where single population proportion z = 95% confidence interval = 1.96, p = 10% single population proportion, d = 5% margin of error, so ((1.96)2 (0.110–0.899)) / (0.05)2 = 140; total sample size = design effect = 2 × 140 = 280; adding 10% no respondent rate, the final sample size is 311.
Sampling procedures
A total of 311 samples were allocated proportionally to the municipal health institutions of Gondar.
The sample was selected using a systematic random sampling technique. The sampling interval (K) was determined by dividing the number of units in the population by its desired sample size. And the first number in K was selected randomly. Finally, the sample was selected for this first number. The value of K = 8 of numbers 1 to 8, one being the number, was randomly selected and the patients at this number were selected according to their arrival order
K = N / n = 2488 / 311 = 8
Among Gondar town, there were eight health institutions. These are the Gondar referral hospital, Azezo, Woleka, Maraki, Besnite, Beteseb Memoria, Polie, and Gebreale health institutions. Among these Gondar referral hospitals, Maraki, Azezo, and Polie were selected by a simple random sampling method.
Study variables
Dependent variable
Dependent variable is HIV-positive test results (positive /negative).
Independent variables
Independent variables include sociodemographic variables, namely, age of the child, residence, occupation status of mothers, marital status of mothers, number of pregnancies, number of births, and educational status of mothers; health-related factors, namely, infants’ age at diagnosis, infant feeding practice place of delivery, infant ARV prophylaxis, mother’s treatment, duration of treatment, and mothers received ART/ARV prophylaxis; obstetric factors, namely, ANC follow-up, antepartum complications such as Antepartum hemorrhage (APH) and Premature rupture of membranes (PROM), duration of membrane rupture, duration of labor, and mode of delivery, gravidity, parity; and psychosocial factors, namely, stigma and discrimination.
Data collection tools and procedures
To collect data from the charts, a structured data extraction tool was developed. The tool was adapted from the national standard HEI follow-up formats and the PMTCT registration logbook, which includes sociodemographic information, information on ARV prophylaxis for mother and infant, delivery site, infant feeding practices, and other important variables. To collect the data, each health facility recruited one ART-trained nurse and one ART-trained midwife.
Data quality and control measures
Data collectors and supervisors were given one day of training.
Data management and analysis
The collected data were checked for completeness and clarity, coded, entered, and analyzed using SPSS version 25. Descriptive, bivariate, and multivariate analyses were performed. All variables were significant at p < 0.25 for the crude odds ratio and at p value ⩽ 0.05 for the adjusted odds ratio. Logistic regressions were used to control for possible confounders and examine the association between independent variables. The generated result was presented using tables and text was set for further discussion.
Result dissemination
The finding of this study was presented in the form of a presentation, and the hard copy was given to University of Gondar, the research center, and to respective stakeholders.
Results
Three hundred eleven study participants were involved making the response rate 100%.
Sociodemographic and economic characteristics
The participant’s mean age is 32.23 (SD =+5.42) years old. A majority of participants (50.8%) were Orthodox Tewahedo followers. A substantial number of the participants are currently married. About half of them are housewives by occupation (Table 1).
Sociodemographic and economic characteristics of participants attending PMTCT in Gondar town health institution, northwest Ethiopia, 2021 (n = 311).

PMTCT: prevention of mother-to-child transmission; ETB: Ethiopia Birr.
Obstetric-related characteristics
More than half, 253 (81.4%), of the participants were multigravida. A majority, 243 (78.1%), of women living with HIV were attending ANC follow-ups. Among these, 170 (70%) start their visits early or at <16 weeks’ gestation (Table 2).
Obstetrics-related characteristics of participants attending PMTCT in the town health institution, northwest Ethiopia, 2021 (n = 311).
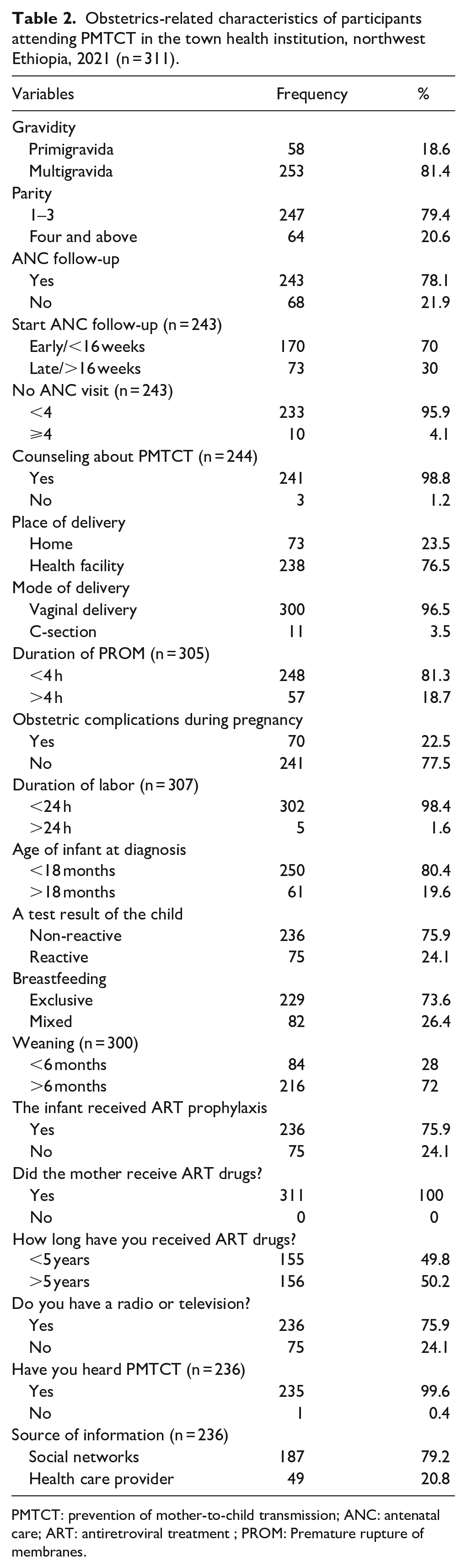
PMTCT: prevention of mother-to-child transmission; ANC: antenatal care; ART: antiretroviral treatment ; PROM: Premature rupture of membranes.
Prevalence of HIV infection
The prevalence of HIV infection among infants born to HIV-positive mothers was found to be 8.1 (95% confidence interval = 7.3–12.9).
Factors associated with infant HIV infection
The finding from the bivariate logistic regression analysis showed the mother’s age, residence, marital status, educational status, occupational status, gravidity, having ANC visit, the start of ANC visit, number of ANC visits, place of delivery, mode of delivery, duration of PROM, obstetrics complication, duration of labor, age of the child at diagnosis, test result, infant feeding practice, weaning time, prevention, and duration of ART were associated with HIV infection.
However, the multivariable analysis found that the following factors were strongly associated with HIV infection: infant feeding practice, educational status of mothers, having ANC visits, and the place of delivery (Table 3).
Factors associated with HIV infection among babies born to HIV-positive mothers attending PMTCT in Gondar City Health Institutions, northwest Ethiopia, 2021 (n = 311).

PMTCT: prevention of mother-to-child transmission; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ANC: antenatal care.
Indicates p values ⩽ 0.001.
Discussion
This section looked at the prevalence and related variables of HIV infection in infants born to HIV-positive mothers. In Ethiopia, DNA testing services have been created as a standard testing mechanism to identify HIV infection.
According to this study, the prevalence of HIV infection among infants was revealed to be 8.1% (95% CI = 7.3–12.9). This demonstrates that MTCT continues to affect a large number of infants, although the World Health Organization (WHO) and the Ethiopian Federal Ministry of Health planned and designed MTCT’s abolition. The findings of the current study were higher than the previous studies in Gondar Specialized Hospital (5.5%), 1 West Gojjam (6.1%), 14 Tigray (2.1%), 7 Awasa (4.16%), 15 Ukraine (1.6%), 11 Kenya (5%), 16 Malawi (4.1%), 17 Zambia (6.5%), 18 Nigeria (2.74%), 19 and France (1.5%). 20 The disparity could be attributed to the high coverage of PMTCT interventions in high-income countries versus limited access, lack of awareness, poor service quality, and other factors in resource-limited countries such as Ethiopia.
Our finding is markedly lower than those of studies conducted in Dire Dawa (15.7%), 21 Jima (17%), 13 and Nigeria (34.4%). 22 This study used a modified WHO guideline (option B+) and applied combined ART drug regimens in health facilities, while the other studies used the previous WHO guideline with Prevention of Mother-to-Child Transmission (PMTCT) option A+ and B implementation programs.
However, a similarity in the prevalence of this study to the study reports from Gondar (10.2%), 23 Cameron (7.1%), 24 and Brazil (11.8%) could be due to the implementation of a similar PMTCT service program, 25 and the difference could be due to HIV awareness, policies and strategies for HIV control and prevention, methodology and sample size, socioeconomic status, good access to health information (especially option B+ MTCT could be higher), and the pastoral nature of life in the study area.
Infants who received mixed breastfeeding were at more than 5 times higher risk than those who received only breastfeeding. This could be due to food contamination during preparation or feeding, resulting in gastrointestinal infection and laceration, causing mucosal barrier breakage and subsequent viral entry into the bloodstream, leading to the progression of HIV infection progression. 11 The observed mixed feeding practice that may be influenced by mothers’ lack of knowledge about the sufficiency of breastfeeding to meet the nutritional demands of their (6-month) infants might contribute to the observed feeding malpractice. There might be missed opportunities to advise mothers of HEIs on infant feeding during the antepartum or postpartum period. As breastfeeding is the most preferred nutritional option for HEIs younger than 6 months, 11 we must ensure that every mother has the right information and means to make the appropriate decisions.
HIV transmission from mother to child is 1.36 times stronger among infants of uneducated mothers compared with those of educated mothers. This could be because as a mother’s educational level increases, so does her understanding of mother-to-child HIV transmission. 11
ANC visits were found to be strongly related to HIV MTCT in this study. Infants with mothers who did not attend ANC were more likely to get a good result than those whose mothers did. This could be because standard HIV testing at ANC visits allows early detection and the beginning of antiretroviral therapy (ARV) for HIV-positive mothers, as well as continuous counseling for institutional delivery preparation throughout follow-up. 26 This was in line with findings from other investigations. 11 An explanation is that part of the ANC program includes health education and raising awareness of HIV transmission from mother to child. 26
Infants born at home had a 2.24 times greater chance of contracting the virus than those born in a hospital. HIV-exposed newborns would be able to receive ARV prophylaxis as soon as they were born, reducing their chances of contracting the virus. 11
Strengths and limitations of the study
We used the probability sampling technique to ensure that the findings could be generalized to the study population.
We performed analyses using a logistic regression model, demonstrating the relationship between the predicted and response variables.
The model controlled the effect of confounders to prevent bias from being introduced at the analysis stage.
The fact that not all potential characteristics were included and tested in this study may have influenced predictor generalization. Despite these flaws, this study offered preliminary findings on the efficacy of routine PMTCT interventions in public health institutions in the study area.
Conclusion
The prevalence of HIV infection in babies born to HIV-positive mothers was found to be high. Mixed infant feeding practice, lack of education, lack of follow-up ANC, and home delivery are significant factors. We also proposed that skilled delivery care and community education could reduce mother-to-child HIV transmission.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221117407 – Supplemental material for Prevalence of HIV infection and associated factors among infants born to HIV-positive mothers in health institutions, northwest Ethiopia, 2021
Supplemental material, sj-docx-1-whe-10.1177_17455057221117407 for Prevalence of HIV infection and associated factors among infants born to HIV-positive mothers in health institutions, northwest Ethiopia, 2021 by Gebrehiwot Ayalew Tiruneh and Emawayish Zeleke Dagnew in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.